Recognition and Management of Acute Pesticide Poisoning WILLIAM M
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Fipronil Poisoning Presenting As Sinus Bradycardia - a Rare Case Report
Jemds.com Case Report Fipronil Poisoning Presenting as Sinus Bradycardia - A Rare Case Report Abhijit Wadekar1, Sreekarthik Pratapa2, Maharshi Patel3, Shilpa Gaidhane4, Nazli Khatib5, 1, 2, 3, 4 Department of Medicine, Acharya Vinoba Bhave Rural Hospital, Sawangi, Wardha, Maharashtra, India. 5 Department of Physiology, Acharya Vinoba Bhave Rural Hospital, Sawangi, Wardha, Maharashtra, India. INTRODUCTION Fipronil is an N-phenylpyrazole insecticide, a second-generation insecticide which is Corresponding Author: relatively new and now commonly used in cotton growing community of rural Central Dr. Shilpa Gaidhane, India. Farmer suicide and deliberate self-poisoning is menace to the Vidarbha region Department of Medicine, of rural Central India. There is paucity of research published on fipronil poisoning, Acharya Vinoba Bhave Rural Hospital, Sawangi, Wardha, Maharashtra, India. clinical features, complications and treatment data. It is scarcely documented E-mail: [email protected] worldwide. Agricultural insecticides are common household items in rural areas of DOI: 10.14260/jemds/2021/247 developing countries. Because of their easy availability, insecticides became a major source of deliberate self-poisoning. As per World Health Organization (WHO), around How to Cite This Article: 3 million poisoning cases with around 0.2 million deaths are noted annually in the Wadekar A, Pratapa S, Patel M, et al. world.1 About 99 % of these deaths occur in developing countries. Insecticide Fipronil poisoning presenting as sinus poisoning is an important public issue in India. Around 168,000 deaths occurred from bradycardia - a rare case report. J Evolution Med Dent Sci 2021;10(16):1166-1168, DOI: pesticide self-poisoning which totals to almost 19.7 % of the global suicides.2 The 10.14260/jemds/2021/247 most common cause of self-poisoning in Central India is ingestion of organophosphorus compounds (OPC). -

Signs and Symptoms of Pesticide Poisoning
University of Nebraska - Lincoln DigitalCommons@University of Nebraska - Lincoln Historical Materials from University of Nebraska-Lincoln Extension Extension 1997 EC97-2505 Signs and Symptoms of Pesticide Poisoning Larry D. Schulze University of Nebraska - Lincoln, [email protected] Clyde Ogg University of Nebraska - Lincoln, [email protected] Edward F. Vitzthum University of Nebraska - Lincoln, [email protected] Follow this and additional works at: https://digitalcommons.unl.edu/extensionhist Part of the Agriculture Commons, and the Curriculum and Instruction Commons Schulze, Larry D.; Ogg, Clyde; and Vitzthum, Edward F., "EC97-2505 Signs and Symptoms of Pesticide Poisoning" (1997). Historical Materials from University of Nebraska-Lincoln Extension. 1225. https://digitalcommons.unl.edu/extensionhist/1225 This Article is brought to you for free and open access by the Extension at DigitalCommons@University of Nebraska - Lincoln. It has been accepted for inclusion in Historical Materials from University of Nebraska-Lincoln Extension by an authorized administrator of DigitalCommons@University of Nebraska - Lincoln. University of Nebraska Cooperative Extension EC97-2505-A Signs and Symptoms of Pesticide Poisoning Larry D. Schulze, Extension Pesticide Coordinator Clyde L. Ogg, Extension Assistant, Pesticide Training Edward F. Vitzthum, Coordinator, Environmental Programs z Manage Your Risk z Signal Words z Read the pesticide Label z Routes of Exposure z Pesticide Toxicity z Recognizing Signs and Symptoms of Poisoning z Recognizing Common pesticide Poisonings { Organophosphate and Carbamate Insecticides { Organochlorine Insecticides { Synthetic Pyrethroid Insecticides { Plant-derived Insecticides { Inorganic Insecticides { Microbial Insecticides { DEET Repellent { Bipyridyl Herbicides { Chlorophenoxy Herbicides { Arsenical Herbicides { Wood Preservatives { Fumigants { Rodenticides { Fungicides z What To Do When Pesticide Poisoning Occurs z References z Pesticide Safety Telephone Numbers Accidental exposure or overexposure to pesticides can have serious implications. -

Sound Management of Pesticides and Diagnosis and Treatment Of
* Revision of the“IPCS - Multilevel Course on the Safe Use of Pesticides and on the Diagnosis and Treatment of Presticide Poisoning, 1994” © World Health Organization 2006 All rights reserved. The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement. The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by the World Health Organization in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters. All reasonable precautions have been taken by the World Health Organization to verify the information contained in this publication. However, the published material is being distributed without warranty of any kind, either expressed or implied. The responsibility for the interpretation and use of the material lies with the reader. In no event shall the World Health Organization be liable for damages arising from its use. CONTENTS Preface Acknowledgement Part I. Overview 1. Introduction 1.1 Background 1.2 Objectives 2. Overview of the resource tool 2.1 Moduledescription 2.2 Training levels 2.3 Visual aids 2.4 Informationsources 3. Using the resource tool 3.1 Introduction 3.2 Training trainers 3.2.1 Organizational aspects 3.2.2 Coordinator’s preparation 3.2.3 Selection of participants 3.2.4 Before training trainers 3.2.5 Specimen module 3.3 Trainers 3.3.1 Trainer preparation 3.3.2 Selection of participants 3.3.3 Organizational aspects 3.3.4 Before a course 4. -

Aluminium Phosphide Poisoning: a Case Report
International Journal of Medical Toxicology and Forensic Medicine. 2014;4(4): 149-53. Aluminium Phosphide Poisoning: a Case Report 1 1 Vaghefi SS *, Emamhadi MA 1 Department of Forensic Medicine and Toxicology, Loghman Hakim Poison Center, Shahid Beheshti University of Medical Sciences, Tehran, Iran A R T I C L E I N F O A B S T R A C T Article Type: Background: Aluminum phosphide as pesticide commonly Case Report used to protect crops from pests. Despite the limited number of cases of poisoning with this substance, it is Article History: important due to the high risk of being fatal. The major Received: 9 April 2014 cause of the poisoning is suicide attempt. Due to the lack of Revised: 14 April 2014 specific treatment in poisoning, taking more than 500 mg is Accepted: 9 May 2014 fatal. Case Report: The patient was a 16-year-old woman who Keywords: attempted suicide by consuming some 4.5gram aluminum Aluminum Phosphide phosphide tablets. Within half an hour after consumption Poisoning she had vomiting and nausea then smoking cigar, followed Hearing Loss closely by smoking in her mouth flames around his mouth is created which will burn (grade II). Subsequently she had argument with her husband and injured her right ear. During the admission she was alert, 2nd degree burn were observed on the upper lip and around the mouth and nose and ears areas. Physical examination was normal, when she arrived she had severe hypotension and her oxygen saturation was 69% with tachycardia. The patient was immediately intubated and received mechanical ventilation. -

Vol 3 No 2 Mar Apr 2003 Online.P65
School Pesticide Monitor A Bi-monthly Bulletin on Pesticides and Alternatives Vol. 3 No. 2 March/April 2003 Beyond Pesticides / National Coalition Against the Misuse of Pesticides 701 E Street, SE, Suite 200 Washington, DC 20003 202-543-5450 [email protected] www.beyondpesticides.org Three New Reports Reveal Children’s Chemical Exposure Evidence Continues to Mount for School Pesticide Reform U.S. EPA released their second edi-tion of tion letters to students and teachers. bicides, pest repellents and disinfectants. America’s Children and the Environment: The Environmental Working Group (EWG), Measures of Contaminants, Body Burdens, The Centers for Disease Control and Preven- in partnership with Mt. Sinai School of Com- and Illnesses (www.epa.gov/envirohealth/ tion (CDC) released the second National Re- munity Medicine and Commonweal, released children) in February. Included in the report port on Human Exposure to Environmental a similar study, Body Burden: The Pollution are the results of a Minnesota study of pes- Chemicals (www.cdc.gov/exposurereport), In People (www.ewg.org/reports/ ticides in schools, which found that some which measured blood and urine samples for bodyburden/index.php). Published in the pesticides have been detected at indoor con- 116 chemicals that found their way into the peer-reviewed journal Public Health Reports, centrations potentially hazardous to chil- human population through pollution or con- the study offers an up-close and personal dren weeks and months after application. sumer products. look at nine individuals whose bodies were tested for 210 chemicals. Subjects contained Forty percent of the responding custodians The report found positive results for 89 an average of 91 compounds, most of which reported that their schools provided no no- chemicals in the volunteers tested, including did not exist 75 years ago. -

A Review of Aluminium Phosphide Poisoning and a Flowchart to Treat It Arh Hig Rada Toksikol 2016;67:183-193 183
Hashemi-Domeneh, et al. A review of aluminium phosphide poisoning and a flowchart to treat it Arh Hig Rada Toksikol 2016;67:183-193 183 Review DOI: 10.1515/aiht-2016-67-2784 A review of aluminium phosphide poisoning and a flowchart to treat it Behrooz Hashemi-Domeneh1,2, Nasim Zamani1,2, Hossein Hassanian-Moghaddam1,2, Mitra Rahimi1,2, Shahin Shadnia1,2, Peyman Erfantalab1,2, and Ali Ostadi1,2 Toxicological Research Center, Department of Clinical Toxicology, Loghman-Hakim Hospital, Shahid Beheshti University of Medical Sciences1, Excellence Center of Clinical Toxicology, Iranian Ministry of Health2, Tehran, Iran [Received in February 2016; CrossChecked in February 2016; Accepted in September 2016] The use of pesticides such as aluminium phosphide (AlP) has increased in the recent years and improved the quantity and quality of agricultural products in a number of developing countries. The downside is that AlP causes severe chronic and acute health effects that have reached major proportions in countries such as India, Iran, Bangladesh, and Jordan. Nearly 300,000 people die due to pesticide poisoning in the world every year. Poisoning with AlP accounts for many of these deaths. Unfortunately, at the same time, there is no standard treatment for it. The aim of this article is to give a brief review of AlP poisoning and propose a treatment flowchart based on the knowledge gained so far. For this purpose we reviewed all articles on the management of AlP poisoning published from 2000 till now. Using a modified Delphi design, we have designed a handy flowchart that could be used as a guide for AlP poisoning management of patients in emergency centres. -
Managing Pesticide Poisoning Risk and Understanding the Signs and Symptoms Clyde L
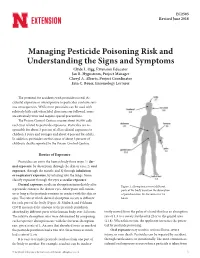
EC2505 Revised June 2018 Managing Pesticide Poisoning Risk and Understanding the Signs and Symptoms Clyde L. Ogg, Extension Educator Jan R. Hygnstrom, Project Manager Cheryl A. Alberts, Project Coordinator Erin C. Bauer, Entomology Lecturer The potential for accidents with pesticides is real. Ac- cidental exposure or overexposure to pesticides can have seri- ous consequences. While most pesticides can be used with relatively little risk when label directions are followed, some are extremely toxic and require special precautions. The Poison Control Centers receive about 90,000 calls each year related to pesticide exposures. Pesticides are re- sponsible for about 3 percent of all accidental exposures to children 5 years and younger and about 4 percent for adults. In addition, pesticides are the cause of about 3 percent of children’s deaths reported to the Poison Control Centers. Routes of Exposure Pesticides can enter the human body three ways: 1) der- mal exposure, by absorption through the skin or eyes; 2) oral exposure, through the mouth; and 3) through inhalation or respiratory exposure, by inhaling into the lungs. Some classify exposure through the eyes as ocular exposure. Dermal exposure results in absorption immediately after Figure 1. Absorption rates of different a pesticide contacts the skin or eyes. Absorption will contin- parts of the body based on the absorption ue as long as the pesticide remains in contact with the skin or of parathion into the forearm over 24 eyes. The rate at which dermal absorption occurs is different hours. for each part of the body (Figure 1). Maiback and Feldman (1974) measured the amount of the pesticide parathion absorbed by different parts of the human body over 24 hours. -

Recognition and Management of Pesticide Poisonings: Fungicides
CHAPTER 16 HIGHLIGHTS Numerous fungicides in use with varying levels of toxicity Fungicides Most are unlikely to cause systemic poisonings, exceptions being Fungicides are extensively used in industry, agriculture and the home and garden for: • Organomercury 1. protection of seed grain during storage, shipment and germination; compounds • Triazoles 2. protection of mature crops, berries, seedlings, flowers and grasses in the field, in storage and during shipment; • Some copper compounds 3. suppression of mildews that attack painted surfaces; • Isolated EBDC 4. control of slime in paper pulps; and exceptions 5. protection of carpet and fabrics in the home. Approximately 500 million pounds of fungicides are applied worldwide annu- ally (see Chapter 1, Introduction). Fungicides vary enormously in their potential for causing adverse effects in humans. Historically, some of the most tragic epidemics of pesticide poisoning occurred by mistaken consumption of seed grain treated with organic mercury or hexachlorobenzene. However, most fungicides currently in use and registered for use in the United States are unlikely to cause frequent or severe acute systemic poison- ings for several reasons: (1) many have low inherent toxicity in mammals and are inefficiently absorbed; (2) many are formulated as suspensions of wettable powders or granules, from which rapid, efficient absorption is unlikely; and (3) methods of application are such that relatively few individuals are intensively exposed. Apart from systemic poisonings, fungicides as a class also cause irritant injuries to skin and mucous membranes, as well as some dermal sensitization. The following discussion considers the recognized adverse effects of widely used fungicides. In the case of those agents that have caused systemic poisoning, some recommendations for management of poisonings and injuries are provided. -

Organochlorine ( Endosulfan) Poisoning Annil Mahajan,Vishal R Tandon*, Rajesh Sharma**, Davinder Singh
JK SCIENCE TOXICOLOGY REVIEW Organochlorine ( Endosulfan) Poisoning Annil Mahajan,Vishal R Tandon*, Rajesh Sharma**, Davinder Singh Endosulfan (C9H6Cl6O3S) is a highly toxic The predominant toxicological effect is over-stimulation organochlorine which belongs to cyclodienes group widely of the CNS. One of the case series reported that seizures used in agriculture (1, 2). It induces T-cell apoptosis, began within one hour after ingestion in (52.2%), in the mitochondrial dysfunction, oxidative stress (3, 4) and lipid second hour in (39.1%), and in the third hour in (8.7%). peroxidation (5, 6).The predominant toxicological effect Seizure are generalized tonic-clonic in (84.2 %) and focal is over-stimulation of the central nervous system (CNS) seizures in (15.8%) (10). The most likely reason for in the form of seizures. Hypoglycemia or Hypergycemia, continuous sustained status epilepticus could be cerebral edema, metabolic abnormalities, & multiple organ hypoglycemia, cerebral edema, hypoxic injury & toxicities involving brain, liver, blood & kidney are common metabolic abnormalities, particularly causing metabolic with this poison (7-10). Their exist dilemmas among acidosis and raised CO2 levels in brain which may casue emergency clinicians and intensive care units team, further aggravation of CNS stimulation leading to status difference of opinion & lack of consensus in treatment epilepticus (7-10). guidelines, of this relatively uncommon poisoning which Thus, ES poisoning should be suspected in the presence often lead to permanent lifelong morbidity or even of primary central nervous system manifestations including mortality. No specific antidote exists. Role of PAM is seizures. It is very important to follow basic principles of controversial in organochlorine poisoning. -

Recognition and Management of Pesticide Poisonings: Sixth Edition: 2013: Chapter 9 Other Insecticides
HIGHLIGHTS CHAPTER 9 Multiple agents with widely varying toxicity Agents of concern Other Insecticides and Acaricides include borates, fluorides, pyrethroids Neonicotinoids are a newer class that merits attention This chapter concerns insecticides and acaricides having toxicologic characteris- due to widespread use and tics distinct from the insecticides discussed in previous chapters. It discusses benzyl toxicity benzoate, borates, chlordimeform, chlorobenzilate, cyhexatin, fluorides, fipronil (an n-phenylpyrazone insecticide), haloaromatic substituted urea compounds, metho- prene, neonicotinoids, propargite and sulfur. SIGNS & SYMPTOMS Variable and highly related BENZYL BENZOATE to the specific agent Incorporated into lotions and ointments, this agent has been used for many years in Boric acid, fluorides, veterinary and human medicine against mites and lice. n-phenylpyrazones and neonicotinoids should be suspected in cases with Toxicology CNS symptoms Apart from occasional cases of skin irritation, adverse effects have been few. The effi- ciency of skin absorption is not known. Absorbed benzyl benzoate is rapidly biotrans- formed to hippuric acid that is excreted in the urine. Oral toxicity in animals is low, TREATMENT with LD50 values in the 2-3 grams/kg range in rats and cats. When given in large doses to laboratory animals, benzyl benzoate causes excitement, incoordination, paralysis of Specific to agent the limbs, convulsions, respiratory paralysis and death.1 Very few human exposures Skin/eye decontamination have been reported to the National Poison Data System. Consider GI decontamination based on Treatment quantity and time interval factors 1. If significant irritant effect appears, discontinue use of product and cleanse skin with soap and water. Treat eye contamination by irrigating exposed eyes with Severe CNS symptoms copious amounts of clean water or saline for at least 15 minutes. -

Occupational Pesticide Illness Surveillance in Michigan: 2001-2003
Occupational Pesticide Illness and Injury Surveillance in Michigan June 2001 - December 2003 August 2005 Division of Environmental and Occupational Epidemiology Michigan Department of Community Health Occupational Pesticide Illness and Injury Surveillance in Michigan June 2001 – December 2003 State of Michigan Governor – Jennifer M. Granholm Michigan Department of Community Health Director – Janet Olszewski, MSW Surgeon General – Kimberlydawn Wisdom, MD, MS Director, Division of Environmental and Occupational Epidemiology – David R. Wade, PhD Authors Abby Schwartz, MPH Martha Stanbury, MSPH Contributor Kenneth Rosenman, MD Acknowledgements The Occupational Pesticide Illness and Injury Surveillance Program wishes to acknowledge those who have contributed to the development and implementation of the surveillance program and this report: Michigan Department of Community Health Jill Granger, MPH Lorraine Cameron, MPH, PhD Tom Largo, MPH Michigan Department of Agriculture Brian Rowe, BS Brian Hughes, PhD, MPH, DABT Pollyanne Kapala, MPA Tom Benner, BS Robin Rosenbaum, BS National Institute for Occupational Safety and Health Geoffrey Calvert, MD, MPH Permission is granted for the reproduction of this publication, in limited quantity, provided the reproductions contain appropriate reference to the source. This publication was supported by grant number 5 U01 OH007306 from the U.S. Centers for Disease Control and Prevention – National Institute for Occupational Safety and Health (CDC-NIOSH). Its contents are solely the responsibility of the authors and do not necessarily represent the official views of CDC-NIOSH. Occupational Pesticide Illness and Injury Surveillance in Michigan: June 2001 - December 2003 Summary This is the first report on surveillance of acute, work-related pesticide illnesses and injuries in Michigan. It summarizes data collected from mid-2001 through 2003. -
Honeybee Pesticide Poisoning
Background Honeybee pesticide poisoning A risk management tool for Australian farmers and beekeepers © 2012 Rural Industries Research and Development Corporation. All rights reserved. ISBN 978-1-74254-386-4 ISSN 1440-6845 Honeybee pesticide poisoning: a risk management tool for Australian farmers and beekeepers Publication No. 12/043 Project No. MT10060 The information contained in this publication is intended for general use to assist public knowledge and discussion and to help improve the development of sustainable regions. You must not rely on any information contained in this publication without taking specialist advice relevant to your particular circumstances. While reasonable care has been taken in preparing this publication to ensure that information is true and correct, the Commonwealth of Australia gives no assurance as to the accuracy of any information in this publication. Products have been included on the basis that they either contain a bee related warning on the product label, or they have the same active constituent(s), active constituent(s) concentration, application rate and intended use as products which contain a bee related warning on the label. The Commonwealth of Australia, the Rural Industries Research and Development Corporation (RIRDC), the authors or contributors expressly disclaim, to the maximum extent permitted by law, all responsibility and liability to any person, arising directly or indirectly from any act or omission, or for any consequences of any such act or omission, made in reliance on the contents of this publication, whether or not caused by any negligence on the part of the Commonwealth of Australia, RIRDC, the authors or contributors. The Commonwealth of Australia does not necessarily endorse the views in this publication.