1 Minutes of the Cradlehall PPC Hearing Friday
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Inverness Active Travel A2 2021
A9 To Wick / Thurso 1 D Ord Hill r Charleston u m s m B it el M t lfie i a ld ll F l A96 To Nairn / Aberdeen R b e Rd Recommended Cycle Routes d a r r Map Key n y City Destinations k B rae Craigton On road School / college / university Dual carriageway Railway Great Glen Way Lower Cullernie Main road Built up area On road - marked cycle lane South Loch Ness Trail Business park / other business Blackhill O a kl eigh R O road - shared foot / cycle path Bike shop dRetail park INVERNESS ACTIVE TRAVEL MAP Minor road Buildings 1 Mai Nutyle North n St 1 P Track Woodland O road - other paths and tracks Bike hire Kessock Visitor attraction o int Rd suitable for cycling Bike repair Hospital / medical centre Path / steps Recreation areas 78 National Cycle Network A9 Balmachree Ke One way trac Church Footbridge Railway station ss Dorallan oc k (contraow for bikes) Steep section (responsible cycling) Br id Bus station ge Allanfearn Upper (arrows pointing downhill) Campsite Farm Cullernie Wellside Farm Visitor information 1 Gdns Main road crossing side Ave d ell R W d e R Steps i de rn W e l l si Railway le l d l P Carnac u e R Crossing C d e h D si Sid t Point R Hall ll rk i r e l a K M W l P F e E U e Caledonian Thistle e d M y I v k W i e l S D i r s a Inverness L e u A r Football a 7 C a dBalloch Merkinch Local S T D o Milton of P r o a Marina n Balloch U B w e O S n 1 r y 1 a g Stadium Culloden r L R B Nature Reserve C m e L o m P.S. -

Inverness Local Plan Public Local Inquiry Report
TOWN AND COUNTRY PLANNING (SCOTLAND) ACT 1997 REPORT OF PUBLIC LOCAL INQUIRY INTO OBJECTIONS TO THE INVERNESS LOCAL PLAN VOLUME 2 CITY OF INVERNESS Reporter: Janet M McNair MA(Hons) M Phil MRTPI File reference: IQD/2/270/7 Dates of the Inquiry: 14 April 2004 to 20 July 2004 INTRODUCTION TO VOLUME 2 This volume deals with objections relating primarily or exclusively to policies or proposals relating to the City of Inverness, which are contained in Chapter 2 of the local plan. Objections with a bearing on a number of locations in the City, namely: • the route of Phase V of the Southern Distributor Road • the Cross Rail Link Road; and • objections relating to retailing issues and retail sites are considered in Chapters 6-8 respectively. Thereafter, Chapters 9-21 consider objections following as far as possible the arrangement and order in the plan. Chapter 22 considers housing land supply in the local plan area and the Council’s policy approach to Green Wedges around Inverness. This sets a context for the consideration of objections relating to individual sites promoted for housing, at Chapter 23. CONTENTS VOLUME 2 Abbreviations Introduction Chapter 6 The Southern Distributor Road - Phase V Chapter 7 The Cross Rail Link Road Chapter 8 Retailing Policies and Proposals Chapter 9 Inverness City Centre Chapter 10 Action Areas and the Charleston Expansion Area 10.1 Glenurquhart Road and Rail Yard/College Action Area 10.2 Longman Bay Action Area 10.3 Craig Dunain Action Area and the Charleston Expansion Area 10.4 Ashton Action Area Chapter 11 -
Appendix A15.1 FINAL.Pdf
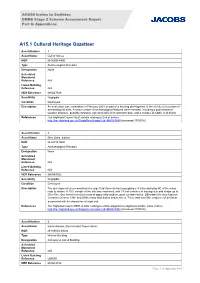
A9/A96 Inshes to Smithton DMRB Stage 2 Scheme Assessment Report Part 6: Appendices A15.1 Cultural Heritage Gazetteer Asset Number 1 Asset Name Dell of Inshes NGR NH 6890 4400 Type Archaeological Remains Designation None Scheduled Monument Reference N/A Listed Building Reference N/A HER Reference MHG47840 Sensitivity Negligible Condition Destroyed Description An evaluation was undertaken in February 2003 as part of a housing development in the vicinity of a number of archaeological sites. A small number of archaeological features were revealed, including a post-medieval wooden structure, possibly industrial, two small pits of an unknown date, and a number of rubble field drains. References The Highland Council HER, details relating to Dell of Inshes http://her.highland.gov.uk/SingleResult.aspx?uid=MHG47840 (accessed 17/05/16) Asset Number 2 Asset Name Nine Oaks, Inshes NGR NH 6910 9520 Type Archaeological Remains Designation None Scheduled Monument Reference N/A Listed Building Reference N/A HER Reference MHG49952 Sensitivity Negligible Condition Destroyed Description The development area consisted of a large field (formerly two) occupying c 4.93ha and lying NE of the minor road to Inshes. A 10% sample of the site was examined, with 13 trial trenches of varying size and shape up to 20 x 40m. One trench revealed a row of apparently modern, post- or stake-holes. Otherwise the only features encountered were 19th- and 20thcentury land drains and services. There was very little evidence of artefacts associated with the deposition of night-soil. -

Inverness Active Travel
S e a T h e o ld r n R b d A u n s d h e C R r r d s o o m n d w M S a t e a l o c l l R e R n n d n a n a m C r g Dan Corbett e l P O s n r yvi P s W d d l Gdns o T Maclennan n L e a S r Gdns l e Anderson t Sea ae o l St Ct eld d R L d In ca Citadel Rd L d i o ia a w S m d e t Ja R Clachnacudden r B e K t e S Fire Station n Kilmuir s u Football s s l Ct r o a PUBLIC a i c r Harbour R WHY CHOOSE ACTIVE TRAVEL? k d Harbour Road R u Club ad S d m t M il Roundabout TRANSPORT K t S Cycling is fast and convenient. Pumpgate Lochalsh n Ct Ct o t College H It is often quicker to travel by bike than by bus or Traveline Scotland – s S a r l b o car in the city. Cycle parking is easy and free. www.travelinescotland.com t e n W u r S N w al R o 1 k o r t er a copyright HITRANS – www.scotrail.co.uk d ScotRail e B S Rd H It helps you stay fit and healthy. t Pl a a Shoe Walker rb e d o Ln G r CollegeInverness City Centreu Incorporating exercise into your daily routine helps Stagecoach – www.stagecoachbus.com r R r a Tap n o R mpg Telford t t d you to achieve the recommended 150 minutes of Skinner h t u S – www.decoaches.co.uk t e Visitor information Post oce D and E Coaches Ct P Ave Waterloo S exercise a week which will help keep you mentally n r Upper Kessock St Bridge Longman Citylink – www.citylink.co.ukCa u Museum & art gallery Supermarket and physically healthy. -
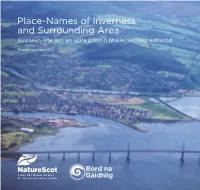
Place-Names of Inverness and Surrounding Area Ainmean-Àite Ann an Sgìre Prìomh Bhaile Na Gàidhealtachd
Place-Names of Inverness and Surrounding Area Ainmean-àite ann an sgìre prìomh bhaile na Gàidhealtachd Roddy Maclean Place-Names of Inverness and Surrounding Area Ainmean-àite ann an sgìre prìomh bhaile na Gàidhealtachd Roddy Maclean Author: Roddy Maclean Photography: all images ©Roddy Maclean except cover photo ©Lorne Gill/NatureScot; p3 & p4 ©Somhairle MacDonald; p21 ©Calum Maclean. Maps: all maps reproduced with the permission of the National Library of Scotland https://maps.nls.uk/ except back cover and inside back cover © Ashworth Maps and Interpretation Ltd 2021. Contains Ordnance Survey data © Crown copyright and database right 2021. Design and Layout: Big Apple Graphics Ltd. Print: J Thomson Colour Printers Ltd. © Roddy Maclean 2021. All rights reserved Gu Aonghas Seumas Moireasdan, le gràdh is gean The place-names highlighted in this book can be viewed on an interactive online map - https://tinyurl.com/ybp6fjco Many thanks to Audrey and Tom Daines for creating it. This book is free but we encourage you to give a donation to the conservation charity Trees for Life towards the development of Gaelic interpretation at their new Dundreggan Rewilding Centre. Please visit the JustGiving page: www.justgiving.com/trees-for-life ISBN 978-1-78391-957-4 Published by NatureScot www.nature.scot Tel: 01738 444177 Cover photograph: The mouth of the River Ness – which [email protected] gives the city its name – as seen from the air. Beyond are www.nature.scot Muirtown Basin, Craig Phadrig and the lands of the Aird. Central Inverness from the air, looking towards the Beauly Firth. Above the Ness Islands, looking south down the Great Glen. -

2 Bus Time Schedule & Line Route
2 bus time schedule & line map 2 Croy View In Website Mode The 2 bus line (Croy) has 8 routes. For regular weekdays, their operation hours are: (1) Croy: 8:40 AM - 1:35 PM (2) Inverness: 2:44 PM - 7:25 PM (3) Inverness: 5:40 PM - 9:23 PM (4) Kinmylies: 6:10 PM - 8:25 PM (5) Leachkin: 6:15 AM - 5:07 PM (6) Piperhill: 6:05 AM - 4:35 PM (7) Tornagrain: 6:10 PM - 7:40 PM (8) Westhill: 6:35 AM - 5:05 PM Use the Moovit App to ƒnd the closest 2 bus station near you and ƒnd out when is the next 2 bus arriving. -
Housing Application Guide Highland Housing Register
Housing Application Guide Highland Housing Register This guide is to help you fill in your application form for Highland Housing Register. It also gives you some information about social rented housing in Highland, as well as where to find out more information if you need it. This form is available in other formats such as audio tape, CD, Braille, and in large print. It can also be made available in other languages. Contents PAGE 1. About Highland Housing Register .........................................................................................................................................1 2. About Highland House Exchange ..........................................................................................................................................2 3. Contacting the Housing Option Team .................................................................................................................................2 4. About other social, affordable and supported housing providers in Highland .......................................................2 5. Important Information about Welfare Reform and your housing application ..............................................3 6. Proof - what and why • Proof of identity ...............................................................................................................................4 • Pregnancy ...........................................................................................................................................5 • Residential access to children -

2A Bus Time Schedule & Line Route
2A bus time schedule & line map 2A Balloch View In Website Mode The 2A bus line (Balloch) has 3 routes. For regular weekdays, their operation hours are: (1) Balloch: 8:15 AM - 5:15 PM (2) Inverness: 6:17 PM (3) Kinmylies: 9:17 AM - 5:17 PM Use the Moovit App to ƒnd the closest 2A bus station near you and ƒnd out when is the next 2A bus arriving. Direction: Balloch 2A bus Time Schedule 48 stops Balloch Route Timetable: VIEW LINE SCHEDULE Sunday 8:15 AM - 5:15 PM Monday Not Operational Blarmore Avenue, Kinmylies Blarmore Avenue, Scotland Tuesday Not Operational Kinmylies Way, Kinmylies Wednesday Not Operational Leachkin Road, Scotland Thursday Not Operational Suilven Way, Kinmylies Friday Not Operational Suilven Way, Inverness Saturday Not Operational Charleston Shopping Centre, Kinmylies Post O∆ce, Kinmylies Charleston View, Kinmylies 2A bus Info Direction: Balloch Charleston View, Kinmylies Stops: 48 U4605, Scotland Trip Duration: 61 min Line Summary: Blarmore Avenue, Kinmylies, Mile End Place, Kinmylies Kinmylies Way, Kinmylies, Suilven Way, Kinmylies, U5253, Scotland Charleston Shopping Centre, Kinmylies, Post O∆ce, Kinmylies, Charleston View, Kinmylies, Charleston Torvean Golf Course, Kinmylies View, Kinmylies, Mile End Place, Kinmylies, Torvean Golf Course, Kinmylies, Tomnahurich Bridge, Tomnahurich Bridge, Ballifeary Ballifeary, Cemetery Gates, Ballifeary, Maxwell Drive, Ballifeary, Glenurquhart Road, Ballifeary, Council Cemetery Gates, Ballifeary Buildings, Ballifeary, Planeƒeld Road, Inverness, King Street, Inverness, Queensgate, -

2019 Urban Series Event Details
2019 Urban Series Event Details Event 1: Lochardil – Friday 6th Sept 2019 Event 2: Kinmylies – Friday 13th Sept 2019 Event 3: Dalneigh – Friday 20th Sept 2019 Starts: 5.30pm TO 6.15pm. Courses close 7.15pm **Please note the course closing time for Dalneigh has been brought forward to 7.15pm** Please check http://invoc.org.uk/ before setting off in case of poor weather conditions and other last-minute information that may affect the event. The Urban Series: Consists of three low key urban races set to test your route choice and quick decision making. All within Inverness. The events are suitable for newcomers to the sport, as navigation is more straightforward than in the forest. The challenge for the experienced orienteer is making quick and correct route choice decisions. The organisation will be low-key using minimal volunteer manpower. Relax and enjoy yourself on these late summer evenings. Urban league and results: Results will be combined into a league. Winner gets 100pts, 2nd place 99pts,etc. Total score over the three events. One league for each course (short and long leagues). Event results and updated leagues will be published on the website as soon as practical after the event www.invoc.org.uk. Courses: There are 2 courses at each event. Long and Short. Winning times are expected to be in the region of 20 to 25 mins, though will vary by event. Juniors: The events are on public roads and the courses have been risked assessed as follows: • Long is suitable for 16 year olds and over only • Short is suitable for 14 year olds and over (other older juniors can run it as well) 13 years and younger can only take part if they are closely accompanied by an adult at all times; this adult must take responsibility for road crossing decisions. -
Consultation of Proposals for Overprovision Statement 2013-16
The Highland Licensing Board Agenda 4 Item Meeting – 27 August 2013 Report HLB/107/13 No Consultation on Proposals for Overprovision Statement 2013-16 Report by the Clerk to the Board Summary Following receipt of the evidence and recommendations submitted by NHS Highland attached at Appendix 1 and a further assessment of crime statistics submitted by Police Scotland attached at Appendix 2, the Board is invited to agree options in relation to proposals for an Overprovision Statement on which to consult statutory consultees and the public and to agree an appropriate consultation period. 1. Background 1.1 On 7 August 2013, the Board agreed proposals for the process of developing a statement under section 7 of the Licensing (Scotland) Act 2005 (the “Act) as to the extent to which the Board considers there to be overprovision of licensed premises, or licensed premises of a particular description, in any locality within the Board’s area. This process involved first ingathering evidence, where available, in relation to all of the five licensing objectives, with the assistance, in particular, of NHS Highland and Northern Constabulary – now part of Police Scotland. 1.2 The ingathering and analysis of evidence has taken longer than was initially anticipated and has not been an easy task. This is particularly because of the differences in the way in which data on alcohol-related harm is and has been collected by the various agencies in Highland, some being collected at intermediate geography/data zone level but some being collected at multimember ward level or, in the case of crime statistics, at police area level or police beat level. -

Demand for Inverness City (Based on First Choice) Carse Central/Crown
Demand for Inverness City (based on first choice) Carse Central/Crown/Raigmore Dalneigh/Springfield Hilton Kinmylies/Muirtown Merkinch Housing Transfer Housing Transfer Housing Transfer Housing Transfer Housing Transfer Housing Transfer List List List List List List List List List List List List 1 bed 67 14 394 101 155 45 109 44 142 35 51 23 2 bed 6 7 91 27 24 24 46 22 41 23 9 7 3 bed 3 2 42 21 17 27 22 6 28 22 11 11 4+ bed 3 25 6 4 11 12 7 6 4 3 4 Total 79 23 552 155 200 107 189 79 217 84 74 45 Demand for Inverness City (based on first choice) Milton of South Kessock Wester Inshes Culcabock Housing Transfer Housing Transfer Housing Transfer Total List List List List List List 1 bed 27 5 21 3 79 10 1325 2 bed 9 4 6 2 41 9 398 3 bed 9 3 2 24 9 259 4+ bed 2 1 1 1 3 2 95 Total 47 13 28 8 147 30 2077 Demand for Inverness City (using all choices) Carse Central/Crown/Raigmore Dalneigh/Springfield Hilton Kinmylies/Muirtown Merkinch Housing Transfer Housing Transfer Housing Transfer Housing Transfer Housing Transfer Housing Transfer List List List List List List List List List List List List 1 bed 423 87 1149 246 877 189 721 138 886 205 482 88 2 bed 85 41 284 94 223 99 219 64 245 98 108 39 3 bed 52 27 146 78 110 83 97 42 132 89 52 43 4+ bed 21 11 55 37 42 36 45 28 41 34 29 12 Total 581 166 1634 455 1252 407 1082 272 1304 426 671 182 Demand for Inverness City (using all choices) Milton of South Kessock Wester Inshes Culcabock Housing Transfer Housing Transfer Housing Transfer Total List List List List List List 1 bed 605 120 351 49 714 149 7479 -

The A9-A96 Inshes to Smithton CPO Schedule
THE A9 and A96 TRUNK ROADS (INSHES TO SMITHTON) COMPULSORY PURCHASE ORDER 201[ ] Made 201[ ] The Roads (Scotland) Act 1984 and the Acquisition of Land (Authorisation Procedure) (Scotland) Act 1947. The Scottish Ministers (hereinafter referred to as “the acquiring authority”) in exercise of the powers conferred by sections 103 to 108 inclusive as read with section 110(2) of the Roads (Scotland) Act 1984 hereby make the following compulsory purchase order- 1. This Order may be cited as the A9 and A96 Trunk Roads (Inshes to Smithton) Compulsory Purchase Order 201[ ]. 2. Subject to the provisions of this Order, the acquiring authority are hereby authorised to purchase compulsorily for the purpose of improving the A96 Aberdeen – Inverness Trunk Road and the M9/A9 Edinburgh – Stirling – Thurso Trunk Road by constructing the new Inshes to Smithton Road between Inshes in the vicinity of Culloden, Inverness-shire and Smithton Roundabout, Inverness, the land and servitude rights which are described in the Schedule hereto and are numbered and shown delineated in red and coloured pink and blue respectively, on the map signed with reference to this Order and marked “Map referred to in the A9 and A96 Trunk Roads (Inshes to Smithton) Compulsory Purchase Order 201[ ]”. 3. In relation to the foregoing purchase section 70 of the Railways Clauses Consolidation (Scotland) Act 1845 and sections 71 to 78 of that Act as originally enacted and not as amended for certain purposes by section 15 of the Mines (Working Facilities and Support) Act 1923 are hereby incorporated with the enactment under which the said purchase is authorised, subject to the modifications that references in the said sections to the company shall be construed as references to the acquiring authority and references to the railway or works shall be construed as references to the land authorised to be purchased and any building or works constructed or to be constructed thereon.