Improving Policing Across Scotland Progress Review of Provision Of
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Inverness Active Travel A2 2021
A9 To Wick / Thurso 1 D Ord Hill r Charleston u m s m B it el M t lfie i a ld ll F l A96 To Nairn / Aberdeen R b e Rd Recommended Cycle Routes d a r r Map Key n y City Destinations k B rae Craigton On road School / college / university Dual carriageway Railway Great Glen Way Lower Cullernie Main road Built up area On road - marked cycle lane South Loch Ness Trail Business park / other business Blackhill O a kl eigh R O road - shared foot / cycle path Bike shop dRetail park INVERNESS ACTIVE TRAVEL MAP Minor road Buildings 1 Mai Nutyle North n St 1 P Track Woodland O road - other paths and tracks Bike hire Kessock Visitor attraction o int Rd suitable for cycling Bike repair Hospital / medical centre Path / steps Recreation areas 78 National Cycle Network A9 Balmachree Ke One way trac Church Footbridge Railway station ss Dorallan oc k (contraow for bikes) Steep section (responsible cycling) Br id Bus station ge Allanfearn Upper (arrows pointing downhill) Campsite Farm Cullernie Wellside Farm Visitor information 1 Gdns Main road crossing side Ave d ell R W d e R Steps i de rn W e l l si Railway le l d l P Carnac u e R Crossing C d e h D si Sid t Point R Hall ll rk i r e l a K M W l P F e E U e Caledonian Thistle e d M y I v k W i e l S D i r s a Inverness L e u A r Football a 7 C a dBalloch Merkinch Local S T D o Milton of P r o a Marina n Balloch U B w e O S n 1 r y 1 a g Stadium Culloden r L R B Nature Reserve C m e L o m P.S. -

Inverness Active Travel
S e a T h e o ld r n R b d A u n s d h e C R r r d s o o m n d w M S a t e a l o c l l R e R n n d n a n a m C r g Dan Corbett e l P O s n r yvi P s W d d l Gdns o T Maclennan n L e a S r Gdns l e Anderson t Sea ae o l St Ct eld d R L d In ca Citadel Rd L d i o ia a w S m d e t Ja R Clachnacudden r B e K t e S Fire Station n Kilmuir s u Football s s l Ct r o a PUBLIC a i c r Harbour R WHY CHOOSE ACTIVE TRAVEL? k d Harbour Road R u Club ad S d m t M il Roundabout TRANSPORT K t S Cycling is fast and convenient. Pumpgate Lochalsh n Ct Ct o t College H It is often quicker to travel by bike than by bus or Traveline Scotland – s S a r l b o car in the city. Cycle parking is easy and free. www.travelinescotland.com t e n W u r S N w al R o 1 k o r t er a copyright HITRANS – www.scotrail.co.uk d ScotRail e B S Rd H It helps you stay fit and healthy. t Pl a a Shoe Walker rb e d o Ln G r CollegeInverness City Centreu Incorporating exercise into your daily routine helps Stagecoach – www.stagecoachbus.com r R r a Tap n o R mpg Telford t t d you to achieve the recommended 150 minutes of Skinner h t u S – www.decoaches.co.uk t e Visitor information Post oce D and E Coaches Ct P Ave Waterloo S exercise a week which will help keep you mentally n r Upper Kessock St Bridge Longman Citylink – www.citylink.co.ukCa u Museum & art gallery Supermarket and physically healthy. -
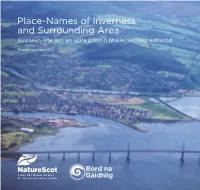
Place-Names of Inverness and Surrounding Area Ainmean-Àite Ann an Sgìre Prìomh Bhaile Na Gàidhealtachd
Place-Names of Inverness and Surrounding Area Ainmean-àite ann an sgìre prìomh bhaile na Gàidhealtachd Roddy Maclean Place-Names of Inverness and Surrounding Area Ainmean-àite ann an sgìre prìomh bhaile na Gàidhealtachd Roddy Maclean Author: Roddy Maclean Photography: all images ©Roddy Maclean except cover photo ©Lorne Gill/NatureScot; p3 & p4 ©Somhairle MacDonald; p21 ©Calum Maclean. Maps: all maps reproduced with the permission of the National Library of Scotland https://maps.nls.uk/ except back cover and inside back cover © Ashworth Maps and Interpretation Ltd 2021. Contains Ordnance Survey data © Crown copyright and database right 2021. Design and Layout: Big Apple Graphics Ltd. Print: J Thomson Colour Printers Ltd. © Roddy Maclean 2021. All rights reserved Gu Aonghas Seumas Moireasdan, le gràdh is gean The place-names highlighted in this book can be viewed on an interactive online map - https://tinyurl.com/ybp6fjco Many thanks to Audrey and Tom Daines for creating it. This book is free but we encourage you to give a donation to the conservation charity Trees for Life towards the development of Gaelic interpretation at their new Dundreggan Rewilding Centre. Please visit the JustGiving page: www.justgiving.com/trees-for-life ISBN 978-1-78391-957-4 Published by NatureScot www.nature.scot Tel: 01738 444177 Cover photograph: The mouth of the River Ness – which [email protected] gives the city its name – as seen from the air. Beyond are www.nature.scot Muirtown Basin, Craig Phadrig and the lands of the Aird. Central Inverness from the air, looking towards the Beauly Firth. Above the Ness Islands, looking south down the Great Glen. -
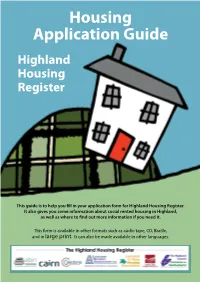
Housing Application Guide Highland Housing Register
Housing Application Guide Highland Housing Register This guide is to help you fill in your application form for Highland Housing Register. It also gives you some information about social rented housing in Highland, as well as where to find out more information if you need it. This form is available in other formats such as audio tape, CD, Braille, and in large print. It can also be made available in other languages. Contents PAGE 1. About Highland Housing Register .........................................................................................................................................1 2. About Highland House Exchange ..........................................................................................................................................2 3. Contacting the Housing Option Team .................................................................................................................................2 4. About other social, affordable and supported housing providers in Highland .......................................................2 5. Important Information about Welfare Reform and your housing application ..............................................3 6. Proof - what and why • Proof of identity ...............................................................................................................................4 • Pregnancy ...........................................................................................................................................5 • Residential access to children -

2019 Urban Series Event Details
2019 Urban Series Event Details Event 1: Lochardil – Friday 6th Sept 2019 Event 2: Kinmylies – Friday 13th Sept 2019 Event 3: Dalneigh – Friday 20th Sept 2019 Starts: 5.30pm TO 6.15pm. Courses close 7.15pm **Please note the course closing time for Dalneigh has been brought forward to 7.15pm** Please check http://invoc.org.uk/ before setting off in case of poor weather conditions and other last-minute information that may affect the event. The Urban Series: Consists of three low key urban races set to test your route choice and quick decision making. All within Inverness. The events are suitable for newcomers to the sport, as navigation is more straightforward than in the forest. The challenge for the experienced orienteer is making quick and correct route choice decisions. The organisation will be low-key using minimal volunteer manpower. Relax and enjoy yourself on these late summer evenings. Urban league and results: Results will be combined into a league. Winner gets 100pts, 2nd place 99pts,etc. Total score over the three events. One league for each course (short and long leagues). Event results and updated leagues will be published on the website as soon as practical after the event www.invoc.org.uk. Courses: There are 2 courses at each event. Long and Short. Winning times are expected to be in the region of 20 to 25 mins, though will vary by event. Juniors: The events are on public roads and the courses have been risked assessed as follows: • Long is suitable for 16 year olds and over only • Short is suitable for 14 year olds and over (other older juniors can run it as well) 13 years and younger can only take part if they are closely accompanied by an adult at all times; this adult must take responsibility for road crossing decisions. -

Demand for Inverness City (Based on First Choice) Carse Central/Crown
Demand for Inverness City (based on first choice) Carse Central/Crown/Raigmore Dalneigh/Springfield Hilton Kinmylies/Muirtown Merkinch Housing Transfer Housing Transfer Housing Transfer Housing Transfer Housing Transfer Housing Transfer List List List List List List List List List List List List 1 bed 67 14 394 101 155 45 109 44 142 35 51 23 2 bed 6 7 91 27 24 24 46 22 41 23 9 7 3 bed 3 2 42 21 17 27 22 6 28 22 11 11 4+ bed 3 25 6 4 11 12 7 6 4 3 4 Total 79 23 552 155 200 107 189 79 217 84 74 45 Demand for Inverness City (based on first choice) Milton of South Kessock Wester Inshes Culcabock Housing Transfer Housing Transfer Housing Transfer Total List List List List List List 1 bed 27 5 21 3 79 10 1325 2 bed 9 4 6 2 41 9 398 3 bed 9 3 2 24 9 259 4+ bed 2 1 1 1 3 2 95 Total 47 13 28 8 147 30 2077 Demand for Inverness City (using all choices) Carse Central/Crown/Raigmore Dalneigh/Springfield Hilton Kinmylies/Muirtown Merkinch Housing Transfer Housing Transfer Housing Transfer Housing Transfer Housing Transfer Housing Transfer List List List List List List List List List List List List 1 bed 423 87 1149 246 877 189 721 138 886 205 482 88 2 bed 85 41 284 94 223 99 219 64 245 98 108 39 3 bed 52 27 146 78 110 83 97 42 132 89 52 43 4+ bed 21 11 55 37 42 36 45 28 41 34 29 12 Total 581 166 1634 455 1252 407 1082 272 1304 426 671 182 Demand for Inverness City (using all choices) Milton of South Kessock Wester Inshes Culcabock Housing Transfer Housing Transfer Housing Transfer Total List List List List List List 1 bed 605 120 351 49 714 149 7479 -

Dalneigh Primary School Handbook
Dalneigh Primary School Handbook 2012/13 Head Teacher – Shona Mackinnon St Ninian Drive Inverness IV3 5AU 01463 232636 [email protected] Dear Parents May I take this opportunity to welcome you as the parent of a new child, to Dalneigh Primary School. Starting school will be both exciting and challenging for your child. Please do not hesitate to contact us to discuss any issues that you may have. I would genuinely encourage all parents to come to school regularly in order that you may share in your child’s education and successes. This handbook explains most aspects of school life for your information. Please keep it for future reference. I look forward to getting to know you and your children over the coming months. Yours sincerely Shona Mackinnon Head Teacher School Aims Our School Aims are: - Provide a broad and balanced programme of work, through which each child should achieve his/her full potential. Further raise levels of attainment by providing more effective stimulating learning and teaching environment to ensure pupils realise their full potential academically and socially. Continue to build on our positive ethos of wider achievement by regular monitoring of progress, and then in turn celebrating our successes. Develop an awareness of citizenship and active health promotion by motivating a responsibility in children and staff alike. Meet the needs of all staff in order to maintain professional standards through continued professional development and staff development and review. Provide equal opportunities for all staff and pupils taking account of cultural, social and religious backgrounds. Nurture a close working partnership with parents and the wider community as well as external agencies for the benefit of all pupils. -

Item 18. Inverness High School Associated School Group Overview
The Highland Council Agenda 18 Item City of Inverness Area Committee Report CIA/16/15 5 March 2015 No Inverness High School Associated School Group Overview Report by Director of Care and Learning Summary This report provides an update of key information in relation to the schools within the Inverness High School Associated School Group (ASG), and provides useful updated links to further information in relation to these schools. 1.0 ASG PROFILE The primary schools in this area serve over 980 pupils, with the secondary school serving 416 young people. ASG roll projections can be found at: School roll forecasts 2014-15 All schools receive support through the Area Office and the Quality Improvement team. Currently, the post of Head Teacher at Dalneigh Primary School is being covered on an acting basis. 1.1 Attainment and Achievement 1.1.1 INVERNESS HIGH SCHOOL Attainment – Performance Summary As a consequence of STACs data no longer being produced, no performance data can be provided at this stage. A separate report using the new “Insight” data will be provided to Members after it becomes available in February 2015. This report will cover all the City of Inverness Area ASGs in a single report, and will enable Members to assess performance across schools and also with comparator schools. 1.1.2 Wider Achievement & Notable Successes Date of Latest School Link to Education Scotland Pages Published Report Bishop Eden’s Primary School May-07 (Follow Up) Bishop Eden’s Primary Inspection Central Primary School Oct-12 Central Primary Inspection Dalneigh Primary School Apr-13 (Follow Up) Dalneigh Primary Inspection Inverness High School Mar-11 Inverness High Inspection Merkinch Primary School Feb-11 Merkinch Primary Inspection St. -

1 Minutes of the Cradlehall PPC Hearing Friday
Minutes of the Cradlehall PPC Hearing Friday 21st June, 2019 PANEL MEMBERS Alasdair Christie Chairman Gaener Roger Lay Member Ian Gibson Lay Member Caroline Morgan Contractor Pharmacist John Mitchell Contractor Pharmacist Jennifer Lumsden Non-contractor Pharmacist BOARD MEMBERS IN ATTENDANCE Alison MacRobbie Macmillan Palliative & Community Care Pharmacist - NHS Highland Fiona Riddell Community Pharmacy Business Manager OBSERVERS Nicola McGibbon Administrative Assistant, NHSH Lynn Matheson CD Inspector, NHSH INTERESTED PARTIES Mr. M. Ameen Applicant Mr. Fraser Culloden & Westhill Community Council Mrs. K. Fraser Ms. Fiona MacFarlane Boots Ms. Gayle Macdonald Mr. Mark Grehan Rowlands Mrs.Mhairi Mann Ms. Shona Scott Tesco Mr. Christopher Boyle Mr. Calum Murray APC Representative 1 1. Chairman’s Address 1.1 The Chairman welcomed everyone to the Hearing and thanked everyone for coming along. He introduced the panel to those present and proceeded to ask the Interested Parties and Applicant, including Observers and Board staff to introduce themself and informed the group that the meeting was being recorded. 1.2 Prior to commencing, the Chairman requested confirmation of everyone being in receipt of all the information and documentation required for the Hearing. Everyone confirmed this to be the case. He informed those present that two Health Board staff were in attendance as Observers for training purposes and ensured there were no objections. Also that over the consultation period some people will have been in contact with Fiona and Alison. He asked if all parties were happy that correct procedures had been followed and confirmed this has been satisfactory. This was confirmed to be the case. He asked for any declarations of perceived conflict of interest to which no-one responded. -

Stagecoach North Scotland Inverness City Guide from 19 August 2019
Stagecoach North Scotland Inverness City Guide from 19 August 2019 This booklet contains all the timetable and route information you’ll need for travelling around Inverness City, including maps of our routes on the centre pages. Easy Access It’s easy getting around Inverness with Stagecoach. All of our local routes are operated by low floor, easy access buses, ideal for wheelchair users, buggies or even just when you’re loaded with shopping bags! Real-Time Tracking We provide real-time bus information on all our routes, enabling our passengers to check exactly when their bus will arrive. You can plan your journey on www.stagecoachbus.com or using our app. Timetable Variations A normal service will operate on Good Friday and Easter Monday. A Saturday service will be in operation on May Day. No services will operate on Christmas Day and New Years Day. Adjusted services will operate during the festive period, please see separate publications issued for this period. School Holidays Highland school holidays for 2019 are: 14-25 October 2019, 23 December 2019- 03 January 2021 On School in service days [19 August 2019, 16,17 September 2019] Services 104, 141, 142, 143, 144 will not operate. All other services will operate a normal schoolday timetable. City Centre l Culduthel Farm l Lochardil l Milton of Leys 1 1A 1B 1C 1U MONDAY TO FRIDAY Service No. 1B 1 1 1B 1 1A 1 1B 1 1A 1 1U 1 1A 1 1B 1 1A 1 NSch Union Street 0517 0535 0605 0627 0635 0645 0705 0710 0730 0745 0800 0815 0830 0845 0900 0915 30 45 00 Old Hilton Tomatin Road 0525 0544 0614 0635 -

HIGHLAND COUNCIL Committee: City of Inverness Area Committee
Agenda 5 Item Report CIA/25/20 No HIGHLAND COUNCIL Committee: City of Inverness Area Committee Date: 19 November 2020 Inner Moray Firth Local Development Plan 2 - Main Issues Report Title: Report Report By: Executive Chief Officer - Infrastructure and Environment 1. PURPOSE/EXECUTIVE SUMMARY 1.1 This report seeks approval for the Main Issues Report for the second Inner Moray Firth Local Development Plan to be published for public consultation. The Main Issues Report enclosed at Appendix 1 has been shaped by a series of appraisals, engagements and discussions outlined in Section 4 of this report. Approval of this consultation document by Committee will allow the Council to seek views on the options for addressing the main issues affecting the future of the area, and also where to direct future development, in the Inner Moray Firth area. 2. RECOMMENDATIONS 2.1 Members are asked to: i. approve the Main Issues Report (as applicable to this committee area) to be published for public consultation, accepting that a number of minor presentational and typographical changes will be made prior to publication; ii. agree the approach to consultation outlined in paragraph 6.1 of this report; and iii. note the important role that the plan will play in addressing the Climate & Ecological Emergency, economic recovery, and in taking forward the Council’s agreed Indicative Regional Spatial Strategy recently submitted to Scottish Government. 3. IMPLICATIONS 3.1 Resource: Resources to complete the statutory processes are allowed for within the Service budget. 3.2 Legal and Risk: the Plan can be challenged in the courts but only on matters of process not planning judgement emphasising the need for the Council to continue to adhere to all statutory procedures throughout the Plan’s progress so that the Council will have a defensible position in the event of any challenge. -

INVERNESS CITY VISION: Building a Better Inverness
INVERNESS CITY VISION: building a better Inverness ‘can ‐do INverness’: where individuals and communities are enabled to fulfil ambitions that benefit them, their city and the wider area; where passion is matched to potential, and every action generates the best possible outcome Table of contents 01. Laying foundations 02. Building structures 03. Making it happen Introduction [our desires] and what we can do [collective Layout of the vision document action and responsibility] The future of Inverness is about people and This visioning document is laid out in three sections: their relationship with the natural and built The visioning process • Section 1: Laying Foundations environment. The city is a remarkable place The vision builds on the successful City Vision • Section 2: Building Structures with a fantastic setting and amazing assets; it of 2003. The starting point for the work was a thorough understanding of the city, what it is, • Section 3: Making it happen is remote but well connected; it is a place its history and identity, how it works. The where people want to be and choose to move broad visioning process is summarised as to. To guide the future we need to agree a follows: vision of what we collectively want to happen. The Vision must be about the needs and aspirations of the many different generations who make up Inverness; this must be a vision for the people, for the creation of their place. In this context, there are four fundamental questions underpinning this vision: 1. Who is the city for? 2. Why would you want to be there? 3.