Cochrane Living Systematic Review Guidance
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Cochrane Collaboration Establishes Representation in Colombia Why and for What Purpose?
EDITORIAL • The Cochrane CollaborationE DITORIin ColombiaAL The Cochrane Collaboration establishes representation in Colombia Why and for what purpose? María XiMena rojas-reyes • Bogotá, D.C. (ColoMBia) DOI: https://doi.org/10.36104/amc.2020.1382 Colombia is, among Latin American countries, the one with the longest track record in the effort to introduce evidence-based medicine to patient care and, subsequently, base health policy decisions on the evidence obtained from research. Several universities have contributed to this process, beginning with the creation of the first master’s program in clinical epidemiology in April 1997 at the Pontificia Universidad Javeriana School of Medicine, followed by an interdepartmental master´s program in clinical epidemiology at the Universidad Nacional approved in 2004, and a clinical epidemiology program affiliated with the Universidad de Antioquia School of Medicine begun in 2005, and continuing to where we are today, with more than six specialization and master’s programs in clinical epidemiology offered at various universities throughout the country. Clinical epidemiology is a discipline in which scientific observations of intact human beings can be carried out and interpreted through the application of epidemiological meth- ods and principles to clinical practice problems. It provides clinicians with information regarding basic research methods which allows them to not only understand and assimilate the information from studies published in the literature, but also to organize their own observations to extract them from the anecdotal level and constitute them as scientifically solid, methodologically valid and clinically relevant assertions. Thus, the clinical epidemiology training programs have contributed to a growing number of clinicians nationwide having the ability to evaluate the validity of information in the medical literature (based on which patient care decisions are made) and produce a synthesis of valid and relevant information to guide the approach to and management of clinical problems. -

The Cochrane Afraid to Challenge the Diagnostic Acu- Men Ofhis Ancestors Or Peers
place or at the wrong time. He was not The Cochrane afraid to challenge the diagnostic acu- men ofhis ancestors or peers. He Collaboration believed that clinical questions often were answered on the basis oftests, Lessons for Public Health rather than on common sense. Practice and Evaluation? Obstetrics offered Cochrane an example ofthe practices ofthe day. Like many other fields ofmedicine, MIRUAM ORLEANS, PHD obstetrics adhered to treatments that perhaps were oftraditional or emo- tional value but which had little basis Archie Cochrane undoubtedly in science. The therapeutic use ofiron wanted to reach providers of and vitamins, the basis for extended health care with his ideas, but he lengths ofstay in hospitals following probably never thought that he would childbirth, and the basis for deciding father a revolution in the evaluation of how many maternity beds were needed medical practices. in Britain were all questioned by In his book ofonly 92 pages, Cochrane, who believed that these "Effectiveness and Efficiency: Random matters could and should be investi- Reflections on Health Services," pub- gated in trials. lished by the Nuffield Provincial Hos- Although Cochrane was by no pitals Trust in 1972, he cast a critical means the first clinician-epidemiologist eye on health care delivery, on many to suggest that randomized controlled A. L Cochrane well-respected and broadly applied trials were an appropriate means of interventions, and on whole fields of deciding questions regarding the effi- were appropriate for laboratory studies medicine and their underlying belief ciency and benefit oftreatment, I can and probably some animal and behav- systems (1). -

Adaptive Clinical Trials: an Introduction
Adaptive clinical trials: an introduction What are the advantages and disadvantages of adaptive clinical trial designs? How and why were Introduction adaptive clinical Adaptive clinical trial design is trials developed? becoming a hot topic in healthcare research, with some researchers In 2004, the FDA published a report arguing that adaptive trials have the on the problems faced by the potential to get new drugs to market scientific community in developing quicker. In this article, we explain new medical treatments.2 The what adaptive trials are and why they report highlighted that the pace of were developed, and we explore both innovation in biomedical science is the advantages of adaptive designs outstripping the rate of advances and the concerns being raised by in the available technologies and some in the healthcare community. tools for evaluating new treatments. Outdated tools are being used to assess new treatments and there What are adaptive is a critical need to improve the effectiveness and efficiency of clinical trials? clinical trials.2 The current process for developing Adaptive clinical trials enable new treatments is expensive, takes researchers to change an aspect a long time and in some cases, the of a trial design at an interim development process has to be assessment, while controlling stopped after significant amounts the rate of type 1 errors.1 Interim of time and resources have been assessments can help to determine invested.2 In 2006, the FDA published whether a trial design is the most a “Critical Path Opportunities -

The Effective Health Care Research Consortium (EHCRC) Publication
Consortium Publication Policy, 20 February 2013 The Effective Health Care Research Consortium (EHCRC) Publication policy The Effective Health Care Research Consortium (the Consortium) has extensive experience in medical publishing, research ethics, and principles of research integrity. Using this experience, and helped by a specialist in the field, we have drawn up this policy document to help promote capacity development in research integrity. 1 This policy applies to all supported Consortium activities. In addition, we encourage partners to use this to prompt their own departments and institutions to develop similar explicit policies. 1. Scope This policy relates to academic publications in peer-reviewed journals including systematic reviews published on The Cochrane Library. This includes authors working with the Cochrane Infectious Diseases Group (CIDG), all Consortium supported Cochrane authors, and all Consortium supported research publications. The policy applies to all outputs from the programme and associated grants (for example, self-published material, reports, newsletters, and blogs). 2. General principles Work supported by the Consortium will be published in a timely and responsible manner. All reports and publications will endeavour to present findings in a responsible, objective and accurate manner and without undue delays. Those who have made a significant contribution to the research will be recognised appropriately by authorship or acknowledgement. 3. Registration of systematic reviews and clinical trials All systematic reviews initiated by the consortium that are not registered as Cochrane Reviews will be prospectively registered on a suitable register (such as PROSPERO). We expect anyone receiving Consortium funds as support to their work (as money, or in kind, such as payment of travel) will, should they be involved in a clinical trial, ensure this trial is registered prospectively (i.e. -

The Cochrane Collaboration: an Introduction P
toolbox research are unlikely to have a high ticular research questions. This is why become dated and irrelevant. Because of number of clinically based trials direct the evidence-based supplement will also this we will seek to both review our core ed towards them. Equally journals endeavour to include these when appro list regularly and also look beyond this which publish qualitative research are priate and well conducted. list. If any reader feels any particular disadvantaged in a table based on ran It is equally important that only well article is important and should be domised-controlled trials or systematic conducted and reported randomised included please feel free to contact the review. However rating journals on the controlled trials or systematic reviews editorial office with the reference. We basis of their number of citations is are included. If we were to look in detail will then include it in our review equally open to challenge as noted at both the randomised-controlled tri process. Provided it passes the quality above. als and systematic reviews identified by filters it will appear in the supplement. Well-conducted randomised -con- the search strategy above many would trolled trials and systematic reviews not meet our quality criteria (see page Acknowledgements based on them have great potential for 32). This supplement will endeavour to To Christine Allot, Librarian, at the Berkshire Health Authority who conducted the answering questions about whether a include only good quality articles relat medline searches. treatment does more harm than good ing to treatment, diagnostic testing, particularly in the clinical situation. -

Cochrane Collaboration Conversation with Givewell
Meeting between Cochrane Collaboration representatives and GiveWell at the U.S. Cochrane Center, May 8, 2012. From the Cochrane Collaboration: Kay Dickersin Director of the U.S. Cochrane Center and the Eyes and Vision Review Group, U.S. Satellite Lorne Becker Director of the Cochrane Collaboration Trading Company and Cochrane Innovations Jeremy Grimshaw Co-Chair, Cochrane Steering Group, Director of the Canadian Cochrane Center, and Coordinating Editor of the Cochrane Effective Practice and Organization of Care Roger Soll Coordinating Editor of the Neonatal Review Group and Member of the Executive Board of the Review Group Coordinating Editors Lisa Bero Director, U.S. Cochrane Center (San Francisco Branch) and Cochrane World Health Organization delegate George Rutherford Coordinating Editor, HIV/AIDS Review Group From GiveWell: Holden Karnofsky and Stephanie Wykstra These notes reflect answers that Cochrane representatives gave during our conversation. Cochrane Collaboration’s aims: • Cochrane Collaboration’s primary aim is to produce high quality systematic reviews of existing health-related research. The organization also trains researchers to do systematic reviews, develops better methods for analyzing and comparing studies in its systematic reviews and educates researchers in the use of these methods, and advocates for evidence-based decision- making within the World Health Organization (WHO), governments, professional associations, consumers and other groups. Structure of the organization: • The Cochrane Collaboration uses a multilevel level organizational and governance structure, comprising a group of “entities” that are organized around functions related to conducting and disseminating systematic reviews of the evidence. Each Cochrane organization (or “entity”) provides its own governance structure and is responsible for raising its own funding. -

Quasi-Experimental Studies in the Fields of Infection Control and Antibiotic Resistance, Ten Years Later: a Systematic Review
HHS Public Access Author manuscript Author ManuscriptAuthor Manuscript Author Infect Control Manuscript Author Hosp Epidemiol Manuscript Author . Author manuscript; available in PMC 2019 November 12. Published in final edited form as: Infect Control Hosp Epidemiol. 2018 February ; 39(2): 170–176. doi:10.1017/ice.2017.296. Quasi-experimental Studies in the Fields of Infection Control and Antibiotic Resistance, Ten Years Later: A Systematic Review Rotana Alsaggaf, MS, Lyndsay M. O’Hara, PhD, MPH, Kristen A. Stafford, PhD, MPH, Surbhi Leekha, MBBS, MPH, Anthony D. Harris, MD, MPH, CDC Prevention Epicenters Program Department of Epidemiology and Public Health, University of Maryland School of Medicine, Baltimore, Maryland. Abstract OBJECTIVE.—A systematic review of quasi-experimental studies in the field of infectious diseases was published in 2005. The aim of this study was to assess improvements in the design and reporting of quasi-experiments 10 years after the initial review. We also aimed to report the statistical methods used to analyze quasi-experimental data. DESIGN.—Systematic review of articles published from January 1, 2013, to December 31, 2014, in 4 major infectious disease journals. METHODS.—Quasi-experimental studies focused on infection control and antibiotic resistance were identified and classified based on 4 criteria: (1) type of quasi-experimental design used, (2) justification of the use of the design, (3) use of correct nomenclature to describe the design, and (4) statistical methods used. RESULTS.—Of 2,600 articles, 173 (7%) featured a quasi-experimental design, compared to 73 of 2,320 articles (3%) in the previous review (P<.01). Moreover, 21 articles (12%) utilized a study design with a control group; 6 (3.5%) justified the use of a quasi-experimental design; and 68 (39%) identified their design using the correct nomenclature. -

SURE Guides for Preparing and Using Evidence-Based Policy Briefs 1
SURE Guides for Preparing and Using Evidence-Based Policy Briefs 1. Getting started Version 2.1 – Updated November 2011 The SURE Collaboration Suggested citation The SURE Collaboration. SURE Guides for Preparing and Using Evidence-Based Policy Briefs: 1. Getting started. Version 2.1 [updated November 2011]. The SURE Collaboration, 2011. Available from www.evipnet.org/sure Copyright You are free to use, distribute and reproduce this work provided the source is properly cited. You may not use this work for commercial purposes without the permission of the SURE Collaboration. SURE is a collaborative project that builds on and supports the Evidence-Informed Policy Network (EVIPNet) in Africa and the Regional East African Community Health (REACH) Policy Initiative. The project involves teams of researchers and policymakers in seven African countries and is supported by research teams in three European countries and Canada. SURE is funded by the European Commission’s 7th Framework Programme (Grant agreement no 222881). Web address: www.evipnet.org/sure Email address: [email protected] 1 1. Getting started 2 Summary In this guide we describe what an ‘evidence-based policy brief’ is, what should be included in such a document, the ways in which it can be used, and the first steps required when preparing one. • What is a policy brief? • What should be included in a policy brief? • How can policy briefs be used? • First steps This guide also includes additional resources for developing a plan to build the capacity needed to prepare and support the use of policy briefs. Resources are also provided for the preparation of rapid responses for policymakers in circumstances in which they may need research evidence but there is insufficient time to prepare a policy brief, or in instances when there is no need to prepare one. -

A Guide to Systematic Review and Meta-Analysis of Prediction Model Performance
RESEARCH METHODS AND REPORTING A guide to systematic review and meta-analysis of prediction model performance Thomas P A Debray,1,2 Johanna A A G Damen,1,2 Kym I E Snell,3 Joie Ensor,3 Lotty Hooft,1,2 Johannes B Reitsma,1,2 Richard D Riley,3 Karel G M Moons1,2 1Cochrane Netherlands, Validation of prediction models is diagnostic test accuracy studies. Compared to therapeu- University Medical Center tic intervention and diagnostic test accuracy studies, Utrecht, PO Box 85500 Str highly recommended and increasingly there is limited guidance on the conduct of systematic 6.131, 3508 GA Utrecht, Netherlands common in the literature. A systematic reviews and meta-analysis of primary prognosis studies. 2Julius Center for Health review of validation studies is therefore A common aim of primary prognostic studies con- Sciences and Primary Care, cerns the development of so-called prognostic predic- University Medical Center helpful, with meta-analysis needed to tion models or indices. These models estimate the Utrecht, PO Box 85500 Str 6.131, 3508 GA Utrecht, summarise the predictive performance individualised probability or risk that a certain condi- Netherlands of the model being validated across tion will occur in the future by combining information 3Research Institute for Primary from multiple prognostic factors from an individual. Care and Health Sciences, Keele different settings and populations. This Unfortunately, there is often conflicting evidence about University, Staffordshire, UK article provides guidance for the predictive performance of developed prognostic Correspondence to: T P A Debray [email protected] researchers systematically reviewing prediction models. For this reason, there is a growing Additional material is published demand for evidence synthesis of (external validation) online only. -

Evaluation of NIHR Investment in Cochrane Report
Evaluation of NIHR investment in Cochrane infrastructure and systematic reviews Committee members: Professor Jos Kleijnen (Chair), Dr Phil Alderson, Dr Jane Aubin, Professor John Cairns, Ms Sally Crowe, and Professor Paul Garner Report writer: Kate Misso 10 February 2017 1 TABLE OF CONTENTS LIST OF TABLES ............................................................................................................................ 5 LIST OF FIGURES ........................................................................................................................... 6 LIST OF ABBREVIATIONS ............................................................................................................... 7 EXECUTIVE SUMMARY ............................................................................................................... 10 1. The global landscape of systematic reviews ............................................................................. 10 2. The performance of NIHR funded Cochrane Review Groups (CRGs) ....................................... 11 3. Cochrane’s impact on key clinical and policy issues in the NHS ............................................... 13 4. The economic impact of systematic reviews ............................................................................ 14 5. Current and planned developments in Cochrane and stakeholders’ views ............................. 14 Conclusions ...................................................................................................................................... -

Experiences of Using Cochrane Systematic Reviews by Local HTA Units
http://ijhpm.com Int J Health Policy Manag 2020, x(x), 1–6 doi 10.34172/ijhpm.2020.133 Short Communication Experiences of Using Cochrane Systematic Reviews by Local HTA Units Thomas G. Poder1,2* ID , Marc Rhainds3 ID , Christian A. Bellemare4 ID , Simon Deblois5 ID , Imane Hammana5 ID , Catherine Safianyk6 ID , Sylvie St-Jacques6 ID , Pierre Dagenais7,8 ID Abstract Article History: This study evaluated the use of Cochrane systematic reviews (CSRs) by Quebec’s local health technology assessment (HTA) Received: 21 November 2019 units to promote efficiency in hospital decision-making. An online survey was conducted to examine: Characteristics of Accepted: 13 July 2020 the HTA units; Knowledge about works and services from the Cochrane Collaboration; Level of satisfaction about the ePublished: 1 August 2020 use of CSRs; Facilitating factors and barriers to the implementation of CSRs evidence in a local context; Suggestions to improve the use of CSRs. Data accuracy was checked by 2 independent evaluators. Ten HTA units participated. From their implementation a total of 321 HTA reports were published (49.8% included a SR). Works and services provided by the Cochrane collaboration were very well-known and HTA units were highly satisfied with CSRs (80%-100%). As regards to applicability in HTA and use of CSRs, major strengths were as follow: Useful as resource for search terms and background material; May reduce the workload (eg, brief review instead of full SR); Use to update a current review. Major weaknesses were: Limited use since no CSRs were available for many HTA projects; Difficulty to apply findings to local context; Focused only on efficacy and innocuity; Cannot be used as a substitute to a full HTA report. -
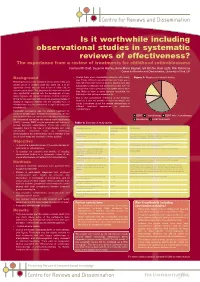
Is It Worthwhile Including Observational Studies in Systematic Reviews of Effectiveness?
CRD_mcdaid05_Poster.qxd 13/6/05 5:12 pm Page 1 Is it worthwhile including observational studies in systematic reviews of effectiveness? The experience from a review of treatments for childhood retinoblastoma Catriona Mc Daid, Suzanne Hartley, Anne-Marie Bagnall, Gill Ritchie, Kate Light, Rob Riemsma Centre for Reviews and Dissemination, University of York, UK Background • Overall there were considerable problems with quality Figure 1: Mapping of included studies (see Table). Without randomised allocation there was a Retinoblastoma is a rare malignant tumour of the retina and high risk of selection bias in all studies. Studies were also usually occurs in children under two years old. It is an susceptible to detection and performance bias, with the aggressive tumour that can lead to loss of vision and, in retrospective studies particularly susceptible as they were extreme cases, death. The prognoses for vision and survival less likely to have a study protocol specifying the have significantly improved with the development of more intervention and outcome assessments. timely diagnosis and improved treatment methods. Important • Due to the considerable limitations of the evidence clinical factors associated with prognosis are age and stage of identified, it was not possible to make meaningful and disease at diagnosis. Patients with the hereditary form of robust conclusions about the relative effectiveness of retinoblastoma may be predisposed to significant long-term different treatment approaches for childhood complications. retinoblastoma. Historically, enucleation was the standard treatment for unilateral retinoblastoma. In bilateral retinoblastoma, the eye ■ ■ ■ with the most advanced tumour was commonly removed and EBRT Chemotherapy EBRT with Chemotherapy the contralateral eye treated with external beam radiotherapy ■ Enucleation ■ Local Treatments (EBRT).