Brighton and Hove CCG 2020/21 Annual Report
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Update: 15 January
Update: 15 January YOUR HEALTHWATCH Dental services Healthwatch Brighton and Hove asked local people to tell us about their experiences of dental care from September to December 2020, and 56 people responded. You can access our findings here. We are receiving a large number of queries asking how to find an NHS dentist. Dental services remain under pressure and full services have not yet resumed and have once again been impacted by the current lockdown. We are working with NHS England, who commission dental services, to get better information and will share this with you as soon as we get this. In the meantime, please email us with any questions and we will do our best to help [email protected] COVID vaccine A reminder that we have created a dedicated webpage on the Healthwatch Brighton and Hove website which is being regularly updated. Further information on the roll-out is provided later on in this bulletin. We have been answering questions about the vaccine and roll-out and hope that you have found our advice helpful. If you have a question, or would like to share your experience of having the vaccine, please email us at [email protected] HEALTH AND SOCIAL CARE UPDATES (1) NHS and care services across the county The Sussex Health and Care Partnership has issued a statement on their website about NHS and care services across the county. Part of this states: Due to the sharp increase in COVID-19 infection rates across our communities in Sussex in recent weeks, demand for NHS and care services across the county has risen significantly. -

Brighton and Hove COVID-19 Vaccination Stakeholder Briefing 26
COVID-19 Response Stakeholder briefing 26 January 2021 COVID-19 Vaccination update: Brighton and Hove This briefing aims to update you on the roll out of the COVID-19 vaccination programme in Brighton and Hove. Latest position We have been stepping up the vaccination programme in phases over recent weeks and we have now done over 200,000 vaccines across Sussex. Official figures will be given later this week but we are on course to vaccinate the top four priority groups across Sussex by mid- February, in line with the national target. We now have arrangements in place for patients at every GP practice across Sussex, we have a large vaccination service going live from next week, and we have added two more hospital hubs to the six we already had in place. This will significantly increase our ability to vaccinate more people quicker in the coming days and weeks. Due to the relatively large number of people who are over 80 living in Sussex, we recognise it will take us longer than in some other parts of the country to vaccinate this priority group in particular. However, we are on track to vaccinate all care homes for older people by the end of the week, in line with the national target, and we expect to have vaccinated all over 80 year olds by the beginning of February. We are working extremely hard to vaccinate as many people as quickly as possible and we are committed to meeting the target of getting the four priority cohorts vaccinated by 15th February. -

Pre-Invite-Letter-March-2021
Wellsbourne Healthcare CIC March 2021 Your local GP surgery in East Brighton www.wellsbournehealthcare.org.uk To all patients of Wellsbourne Healthcare Dear Patient You will soon be invited for your Covid-19 vaccine. Here is how it will work: 1. You will receive a text message to your mobile phone. Please follow the instructions in the text message to book your appointment at the Brighton Racecourse Vaccination Facility. This is the easiest and quickest way to get your appointment. 2. If you cannot respond to the text, you will receive a phone call inviting you to book your appointment 3. The texts and calls will come from our partners who are organising the appointments. They may be called ‘NHSNoReply’ or ‘HERE’ or ‘IAS’. You can trust them. We are asking everyone to make their own way to Brighton Racecourse. There is free parking. Please travel by car, bus or taxi, or ask your family or friends to help. If you cannot make your own way to the Racecourse, you will be offered a free taxi service. This will be confirmed at the time you are making your appointment over the phone. Please make use of this free service if you need it. It is there for everyone. If you cannot travel at all, even with assistance, you will receive a home visit from a District Nurse. Thank you for your understanding. It is wonderful news that vaccinations are under way and we will reach everyone as quickly as possible. There is more information overleaf, including how to let us know if you cannot get to the Racecourse at all. -
Pankhurst and Craven Vale
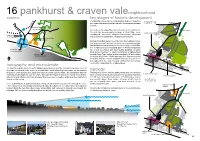
16 pankhurst & craven valeneighbourhood context key stages of historic development Pankhurst & Craven Vale is a strip of urban and inner suburban development that runs from the top of the Downs down towards 1897-9 workhouse the sea. London Road 15 minutes on foot Its location at the edge of the city has meant that, through history, racecourse the area has accommodated a range of urban fringe uses, Kemp Town station Brighton station including the racecourse, Brighton’s workhouse, allotments 11 minutes by bus and a variety of sanatoriums, hospitals and asylums. Pankhurst & Craven Vale neighbourhood Eastern Road has always been the main thoroughfare, below the neighbourhood, and was the local centre providing shops, allotments facilities and the transport hub to the surrounding communities. The neighbourhood surrounding Eastern Road and Edward city centre Street was developed with poor quality buildings including 14 minutes by bus back to back housing. The southern part of the neighbourhood Marina around Kemp Town railway station was badly hit by bombing 19 minutes by bus during the World War II. Bomb damage, slum clearance during N the 1950s and 60s, and the available allotment land led to the development of the large housing estates that now occupy topography and microclimate much of the land within the neighbourhood. The land rises up steeply to the north affording panoramic views of the sea and Kemp Town. Current development situated on the incline is orientated due south within large open space ideally situated typology Eastern Road for passive solar gain but also exposed to south west and easterly winds. -

Vaccine Update: 14 January
Vaccine update: 14 January Key updates about the vaccine This information is in addition to that shown on the Healthwatch Brighton and Hove website which includes details of the priority list, and vaccination centres. Please click here to access the website which is being updated regularly. For additional information: The Sussex Health and Care Partnership have produced the following webpages to help you understand what will happen next: • For answers to Frequently Asked Questions about the vaccination programme please click here. o We have attached the questions which are included below so that you can see what information is available. We have not included the answers as these are being routinely updated in line with amended guidance, and as we learn more. • When will I get my jab? • For details of Brighton and Hove vaccination services • Health and care workforce vaccinations Vaccinations GP sites • It has been announced that Brighton Racecourse will go live this week for patients at: Park Crescent Health Centre, St Peter’s Medical Centre, Wellsbourne Healthcare CIC, Albion Street Surgery, Arch healthcare, Ardingly Court Surgery, Broadway Surgery, Pavilion Surgery, Regency Surgery, Saltdean and Rottingdean Medical Practice, School House Surgery, Ship Street Surgery, St Luke’s Surgery, The Avenue Surgery, Woodingdean Medical Centre. Other GP-led sites are already operating. County Oak Medical Centre: For patients at Brighton Station Health Centre, Carden Surgery, Montpelier Surgery, Seven Dials Medical Centre and University of Sussex Health Centre. Portslade Health Centre: For patients at Brighton Health and Wellbeing Centre, Benfield Valley Healthcare Hub, Charter Medical Group, Hove Medical Centre, Links Road Surgery, Mile Oak Medical Centre, Portslade Health Centre, Trinity Medical Centre, and Wish Park Surgery. -

Wellsbourne Healthcare, Aged 80 and Over
Wellsbourne Wednesday 13th January 2021 Healthcare CIC Your local GP surgery in East Brighton www.wellsbournehealthcare.org.uk To all patients of Wellsbourne Healthcare, aged 80 and over Dear Patient You will soon be invited for your Covid-19 vaccine. Here is how it will work: 1. You will receive a text message to your mobile phone. Please follow the instructions in the text message to book your appointment at the Brighton Racecourse Vaccination Facility. This is the easiest and quickest way to get your appointment. 2. If you cannot respond to the text, you will receive a phone call inviting you to book your appointment 3. The texts and calls will come from our partners who are organising the appointments. They may be called ‘NHSNoReply’ or ‘HERE’ or ‘IAS’. You can trust them. We are asking everyone to make their own way to Brighton Racecourse. There is free parking. Please travel by car, bus or taxi, or ask your family or friends to help. We are arranging transport for those who cannot get there by any other means. If you cannot travel at all, even with assistance, we are arranging home visits. At this time, however, we cannot say exactly when these options will be available. Thank you for your understanding. It is wonderful news that vaccinations are under way and we will reach everyone as quickly as possible. There is more information overleaf, including how to let us know if you need travel assistance or cannot get to the Racecourse at all. Yours sincerely Sarah Webb, Practice Manager Wellsbourne Healthcare CIC Wellsbourne Healthcare CIC, 179 Whitehawk Road, Brighton BN2 5FL Community Interest Company Number: 10974442 Vaccinations for Wellsbourne Healthcare CIC Patients at Brighton Racecourse We are writing to you to let you know that the way you will be invited for this vaccine is different to how we normally invite you for vaccinations. -

Responding to Nature
Responding to nature. Hannah Redfern Hughes 1 Health benefits of nature: Mind advocates for the use of Eco therapy. This specific type of therapy, which includes doing activities outdoors in nature, is found to help with mild to moderate depression and anxiety. I will always personally attest to the benefits of nature, specifically when I go for a walk with the aim of finding a green space or just to listen to the sea. I find it a very relaxing experience and helps to relieve any everyday stress. Own image. 20/07/20. 18.28 PM. Darren y gesail. 2 "Nature And Mental Health". Mind.Org.Uk, 2018. Bonnie Kemske Sarah purvey ‘Cast Hugs’ is an interesting way to get the viewer to interact with an object. I think that exploring the forms and texture I use could be a way to encourage interaction with my vessels. I wanted to include Purvey’s work because I was interested in her mark making and how she can convey the energy of the landscape through it. Fig 1.Kemske, Bonnie. Cast Hugs. RCA, London, 2007. Fig.2, ‘Grazed’. Part of Purvey’s Landscape series. 3 Helen Carnac Richard Long The translation of drawing to vessel is what interested me about Carnac’s work. Fig.3. Richard Long. Walk of Seven Cairns. 1992 I’ve referenced one of Long’s text-works because he is known for using walks at the centre of his work. I was interested to see how he used different mediums to document them. Fig,3. Helen Carnac. Each other. -

Brighton and Hove COVID-19 Vaccination Stakeholder Briefing
COVID-19 Response Stakeholder briefing 02 February 2021 COVID-19 Vaccination update: Brighton and Hove Welcome to your regular briefing from the Sussex Health and Care Partnership on the roll- out of the COVID-19 vaccination programme in Brighton and Hove. Introduction The COVID-19 vaccination programme continues to be rolled out across our communities. The top line brief from this week is: We are on course to have offered the COVID-19 vaccination to the top four priority groups by mid-February, in line with the national target; Residents living in all care homes for older people in Brighton and Hove have been offered the COVID-19 vaccine. A small remainder of homes in Sussex have had visits deferred for safety reasons, following a risk assessment, during a local outbreak; All registered patients who are eligible for a vaccine has access to a GP-led vaccination service; Following the successful launch of a large vaccination centre at the Brighton Centre last week, two further vaccination centres have opened this week in Eastbourne and Crawley; Seven hospital hubs are currently focussing on vaccinating health and care staff; Home visits have started via a roving service to take the vaccine into people’s own homes if they are housebound and cannot attend a vaccination site. Latest position In the latest data published today, up to 25 January 2021 in Sussex: 202,509 doses of the COVID-19 vaccination have been delivered; 81,614 people aged 80 and over have been vaccinated; Sussex is 7th highest in the country for the number of people age 80 and over that have received their vaccination and has the third highest population of people aged 80 and over. -
Brighton Clr Cdd with Bus Stops Map (Web)
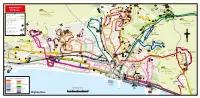
CO 25 to Horsham R.S.P.C.A. LDEAN LA. 84# 77 to Devil’s Dyke 17 Old Boat 79‡ to Ditchling Beacon 5B# * -PASS 50.50U HOVE BY Corner NORTHFIELD 270 to East Grinstead IGHTON & 78‡ BR Braeside STANMER PARK CRESCENT 271.272.273 to Crawley Glenfalls Avenue Church R D Northfield Crescent E 5B#.50 E Thornhill Avenue F V L East O E I L’ N Avenue U E Park Village C 50U.84# S D V E N A T O 5B# 5A N O N Sanyhils E Crowhurst E Brighton Area 5 U Crowhurst R EN V D D Avenue A Road 24 Y Craignair E R Road 5B#.23 Y R SID A Bramber House K AE West Avenue C Stanmer R E O BR Eskbank North A 25.25X B D D Avenue Saunders Hill R . 17 IG University 50.50U.84# R H H C T Village O 270 Patcham Mackie Avenue O O Bus Routes A N A Barrhill Asda L D W D B & Science Park Road 28 to Ringmer 271 5.5A 5B.26 E of Sussex North A Avenue K A H R 5B.24.26 H N O South 272 V 29B to Uckfield R 46 U 5B# 5A UE E 78‡ 25 H VEN Thornhill Avenue Road Falmer Village 5 A R 273 E * 52.55# L B I KI A C 52. #55 S Y toTunbridge Wells L A 29.29X# M Bowling N - Sussex House T P L 24 A 84# Haig Avenue E S Green S 52 Carden Cuckmere W A S S P Ladies Sport Centre A A V KEY P Portfield Hill O R #29X T Way - . -

Sue Berry, 'A Resort Town Transformed: Brighton C.1815–1840'
Sue Berry, ‘A resort town transformed: Brighton c.1815–1840’, The Georgian Group Journal, Vol. XXIII, 2015, pp. 213–230 TEXT © THE AUTHORS 2015 A RESORT TOWN TRANSFORMED: BRIGHTON c. ‒ SUE BERRY Most of the elegant terraces, squares and crescents in Brighton, Dale accepted the common view that it modern Brighton and Hove were begun between about was a mere fishing village before the Prince of Wales and . The majority were built along the arrived in . More recent research has emphasised sweeping bay on which this resort stands. The first aim that Brighton was not a village but a town, albeit a of this article is to summarise recent research which small and poor one, which was regenerated by expands and revises major parts of Anthony Dale’s seaside tourism from the s. By the time the Fashionable Brighton ‒ ( ). This Prince arrived it was already a popular, rapidly pioneering work formed part of a campaign to save growing resort, aided by good access to London and Adelaide Crescent and Brunswick Town from starting to expand onto agricultural land. demolition and to raise the profile of other coastal Dale thought that the development of the town developments to help protect them. The second aim is to before about had little influence on the location draw attention to the importance of other extensive, and scale of the projects that he described. But deeds and expensive, improvements which were essential to and other sources have since revealed that the the success of a high-quality resort town during this practices used to buy blocks of strips in the period, but which Dale did not discuss. -
Housing and Mixed Use Site Allocations Topic Paper
Housing and Mixed Use Site Allocations Topic Paper June 2018 Site Allocations Topic Paper Contents Introduction 2 Background 2 Overarching Approach in City Plan Part Two 3 Housing and Mixed Use Site Allocations (Policy H1) 4 Urban Fringe Site Allocations (Policy H2) 7 Purpose Built Student Accommodation Site Allocations 9 (Policy H3) Strategic Site Allocations (Policies SSA1 – SSA4) 12 Appendices Appendix 1 – Housing and Mixed Use Sites 14 Appendix 2 – Urban Fringe Sites 30 Appendix 3 – Housing and Mixed use Site Proformas 35 Appendix 4 – Urban Fringe Site Proformas 173 Maps in this document are based on Ordnance Survey data. © Crown Copyright. All rights reserved. Licence: 100020999, Brighton & Hove City Council. 2018. 1. Introduction 1.1 The purpose of this Topic Paper is to outline the Council’s approach to the proposed housing, mixed use and purpose built student accommodation (PBSA) site allocations set out in Policies H1, H2, H3 and SSA1 to SSA4 of the draft City Plan Part Two (CPP2). 2. Background 2.1 In City Plan Part One (CPP1) strategic policies set the overall amounts of new development to be delivered across the city to 2030 and the broad locations where significant new housing development will take place. Part Two of the City Plan builds on this strategic framework, by identifying and allocating additional sites particularly for new housing development to enable the delivery of sufficient new housing to meet the adopted strategic housing target. 2.2 CPP1 Policy CP1 (Housing Delivery) sets out how the Council will make provision for at least 13,200 new homes to be built over the plan period 2010 – 2030, equating to an annual average rate of provision of 660 dwellings. -
Vebraalto.Com
2A The Broadway, Brighton, BN2 5NF £335,000 Leasehold AN AMAZING FIND... EASY REACH RSCH and BRIGHTON MARINA is this 3 bedroom MAISONETTE which boasts it's own GARAGE and GARDEN. Recently REFURBISHED throughout. Bathroom and wet room. EPC E54. Front Door To Hallway Wood flooring, radiator, stairs to first floor with glass panel and feature lighting. Bedroom Radiator, built-in vanity unit, range of built-in cupboards, double glazed window to the front. Bathroom Range of bathroom fitments comprising bath with mixer taps, mains fed shower attachment and glass shower panel. Low level close coupled WC, vanity unit with inset sink and mixer taps and mirror above. Tilled floor, part-tiled walls, range of built-in cupboards. Cupboard housing boiler. Double glazed window to the front with frosted glass, ladder style heated towel rail. Kitchen Range of kitchen fitments comprising inset 'Lamona' oven and 4 ring gas hob with extractor fan over. Inset fridge, freezer, dishwasher, washing machine. Stainless steel single drainer sink unit with mixer taps. Part tiled walls, cupboard housing electric and gas meters. Dining Room Location: Radiator, Double glazed bay window to the front. The Broadway is located at the lower end of Whitehawk with a variety of local shops close by and good bus links to the Lounge Double glazed window to the rear, radiator, engineered oak City Centre. You will also find the Royal Sussex County flooring. Hospital close by as is Brighton Marina with a larger variety of shops, the Asda superstore, restaurants and cinema. It Stairs to First Floor won’t take too long to stroll or drive to the seafront or nearby bustling Kemptown.