Orthognathic (Jaw) Surgery
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Glossary for Narrative Writing
Periodontal Assessment and Treatment Planning Gingival description Color: o pink o erythematous o cyanotic o racial pigmentation o metallic pigmentation o uniformity Contour: o recession o clefts o enlarged papillae o cratered papillae o blunted papillae o highly rolled o bulbous o knife-edged o scalloped o stippled Consistency: o firm o edematous o hyperplastic o fibrotic Band of gingiva: o amount o quality o location o treatability Bleeding tendency: o sulcus base, lining o gingival margins Suppuration Sinus tract formation Pocket depths Pseudopockets Frena Pain Other pathology Dental Description Defective restorations: o overhangs o open contacts o poor contours Fractured cusps 1 ww.links2success.biz [email protected] 914-303-6464 Caries Deposits: o Type . plaque . calculus . stain . matera alba o Location . supragingival . subgingival o Severity . mild . moderate . severe Wear facets Percussion sensitivity Tooth vitality Attrition, erosion, abrasion Occlusal plane level Occlusion findings Furcations Mobility Fremitus Radiographic findings Film dates Crown:root ratio Amount of bone loss o horizontal; vertical o localized; generalized Root length and shape Overhangs Bulbous crowns Fenestrations Dehiscences Tooth resorption Retained root tips Impacted teeth Root proximities Tilted teeth Radiolucencies/opacities Etiologic factors Local: o plaque o calculus o overhangs 2 ww.links2success.biz [email protected] 914-303-6464 o orthodontic apparatus o open margins o open contacts o improper -

WHAT HAPPENED? CDR, a 24-Year-Old Chinese Male
CHILDHOOD DEVELOPMENTAL SCREENING 2020 https://doi.org/10.33591/sfp.46.5.up1 FINDING A MASS WITHIN THE ORAL CAVITY: WHAT ARE THE COMMON CAUSES AND 4-7 GAINING INSIGHT: WHAT ARE THE ISSUES? In Figure 2 below, a list of masses that could arise from each site Figure 3. Most common oral masses What are the common salivary gland pathologies Salivary gland tumours (Figure 7) commonly present as channel referrals to appropriate specialists who are better HOW SHOULD A GP MANAGE THEM? of the oral cavity is given and elaborated briey. Among the that a GP should be aware of? painless growing masses which are usually benign. ey can equipped in centres to accurately diagnose and treat these Mr Tan Tai Joum, Dr Marie Stella P Cruz CDR had a slow-growing mass in the oral cavity over one year more common oral masses are: torus palatinus, torus occur in both major and minor salivary glands but are most patients, which usually involves surgical excision. but sought treatment only when he experienced a sudden acute mandibularis, pyogenic granuloma, mucocele, broma, ere are three pairs of major salivary glands (parotid, commonly found occurring in the parotid glands. e most 3) Salivary gland pathology may be primary or secondary to submandibular and sublingual) as well as hundreds of minor ABSTRACT onset of severe pain and numbness. He was fortunate to have leukoplakia and squamous cell carcinoma – photographs of common type of salivary gland tumour is the pleomorphic systemic causes. ese dierent diseases may present with not sought treatment as it had not caused any pain. -
Mandibular Tori
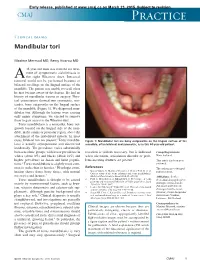
Early release, published at www.cmaj.ca on March 23, 2015. Subject to revision. CMAJ Practice Clinical images Mandibular tori Maxime Mermod MD, Remy Hoarau MD 44-year-old man was referred for treat- ment of symptomatic sialolithiasis in A the right Wharton duct. Intraoral removal could not be performed because of bilateral swellings on the lingual surface of the mandible. The patient was unable to recall when he first became aware of the lesions. He had no history of mandibular trauma or surgery. Phys- ical examination showed two symmetric, non- tender, bony outgrowths on the lingual surface of the mandible (Figure 1). We diagnosed man- dibular tori. Although the lesions were causing only minor symptoms, we elected to remove them to gain access to the Wharton duct. Torus mandibularis is a nontender, bony out- growth located on the lingual side of the man- dible, in the canine or premolar region, above the attachment of the mylohyoid muscle. In most 1 cases, bilateral tori are present. Torus mandibu- Figure 1: Mandibular tori are bony outgrowths on the lingual surface of the laris is usually asymptomatic and discovered mandible, often bilateral and symmetric, as in this 44-year-old patient. incidentally. The prevalence varies substantially between ethnic groups, with lower prevalence in resection is seldom necessary, but is indicated Competing interests: whites (about 8%) and blacks (about 16%) and when ulceration, articulation disorder or prob- None declared. higher prevalence in Asian and Inuit popula- lems inserting dentures are present.3 This article has been peer tions.2 Torus mandibularis is slightly more com- reviewed. -

Abscesses Apicectomy
BChD, Dip Odont. (Mondchir.) MBChB, MChD (Chir. Max.-Fac.-Med.) Univ. of Pretoria Co Reg: 2012/043819/21 Practice.no: 062 000 012 3323 ABSCESSES WHAT IS A TOOTH ABSCESS? A dental/tooth abscess is a localised acute infection at the base of a tooth, which requires immediate attention from your dentist. They are usually associated with acute pain, swelling and sometimes an unpleasant smell or taste in the mouth. More severe infections cause facial swelling as the bacteria spread to the nearby tissues of the face. This is a very serious condition. Once the swelling begins, it can spread rapidly. The pain is often made worse by drinking hot or cold fluids or biting on hard foods and may spread from the tooth to the ear or jaw on the same side. WHAT CAUSES AN ABSCESS? Damage to the tooth, an untreated cavity, or a gum disease can cause an abscessed tooth. If the cavity isn’t treated, the inside of the tooth can become infected. The bacteria can spread from the tooth to the tissue around and beneath it, creating an abscess. Gum disease causes the gums to pull away from the teeth, leaving pockets. If food builds up in one of these pockets, bacteria can grow, and an abscess may form. An abscess can cause the bone around the tooth to dissolve. WHY CAN'T ANTIBIOTIC TREATMENT ALONE BE USED? Antibiotics will usually help the pain and swelling associated with acute dental infections. However, they are not very good at reaching into abscesses and killing all the bacteria that are present. -

Total Temporomandibular Joint Replacement and Simultaneous Orthognathic Surgery Using Computer- Assisted Surgery
Total Temporomandibular Joint Replacement and Simultaneous Orthognathic Surgery Using Computer- Assisted Surgery Natalia Lucia Gomez, Luis Alejandro Boccalatte, Águeda Lopez Ruiz, María Gabriela Nassif, Marcelo Fernando Figari, et al. Journal of Maxillofacial and Oral Surgery ISSN 0972-8279 J. Maxillofac. Oral Surg. DOI 10.1007/s12663-020-01422-y 1 23 Your article is protected by copyright and all rights are held exclusively by The Association of Oral and Maxillofacial Surgeons of India. This e-offprint is for personal use only and shall not be self-archived in electronic repositories. If you wish to self-archive your article, please use the accepted manuscript version for posting on your own website. You may further deposit the accepted manuscript version in any repository, provided it is only made publicly available 12 months after official publication or later and provided acknowledgement is given to the original source of publication and a link is inserted to the published article on Springer's website. The link must be accompanied by the following text: "The final publication is available at link.springer.com”. 1 23 Author's personal copy J. Maxillofac. Oral Surg. https://doi.org/10.1007/s12663-020-01422-y CLINICAL PAPER Total Temporomandibular Joint Replacement and Simultaneous Orthognathic Surgery Using Computer-Assisted Surgery 1 1 2 Natalia Lucia Gomez • Luis Alejandro Boccalatte • A´ gueda Lopez Ruiz • 1 1 3,4 Marı´a Gabriela Nassif • Marcelo Fernando Figari • Lucas Ritacco Received: 6 April 2020 / Accepted: 10 July 2020 Ó The Association of Oral and Maxillofacial Surgeons of India 2020 Abstract Materials and methods We present two cases to illustrate Background Disorders of the temporomandibular joint our protocol and its results. -

Incidence and Bacteriology of Bacteremia Associated with Various Oral and Maxillofacial Surgical Procedures
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Kanazawa University Repository for Academic Resources Incidence and bacteriology of bacteremia associate with various oral and maxillofacial surgical procedures 著者 Takai Sumie, Kuriyama Tomoari, Yanagisawa Maki, Nakagawa Kiyomasa, Karasawa Tadahiro journal or Oral Surgery, Oral Medicine, Oral Pathology, publication title Oral Radiology, and Endodontology volume 99 number 3 page range 292-298 year 2005-03-01 URL http://hdl.handle.net/2297/2456 Incidence and bacteriology of bacteremia associated with various oral and maxillofacial surgical procedures Sumie Takai, DDS a, Tomoari Kuriyama, DDS, PhD b, Maki Yanagisawa, DDS c, Kiyomasa Nakagawa, DDS, PhD d and Tadahiro Karasawa MD, PhD e Department of Oral and Maxillofacial Surgery, Kanazawa University Graduate School of Medical Science, KANAZAWA, JAPAN a PhD Student, Department of Oral and Maxillofacial Surgery, Kanazawa University Graduate School of Medical Science b Clinical Instructor, Department of Oral and Maxillofacial Surgery, Kanazawa University Hospital c PhD Student, Department of Oral and Maxillofacial Surgery, Kanazawa University Graduate School of Medical Science d Associate Professor, Department of Oral and Maxillofacial Surgery, Kanazawa University Graduate School of Medical Science e Professor, Department of Laboratory Sciences, School of Health Sciences, Kanazawa University Corresponding author: Dr. Tomoari Kuriyama Post: Department of Oral and Maxillofacial Surgery, Kanazawa University Hospital 13-1 Takara-machi, Kanazawa 920-8640, Ishikawa, Japan Tel.: +81 (0) 76 265 2444 Fax.: +81 (0)76 234 4202 E-mail: [email protected] 1 1 Abstract 2 Objective. The aim of this study was to determine the incidence and bacteriology of 3 bacteremia associated with various oral and maxillofacial surgical procedures. -

Temporomandibular Joint Regeneration: Proposal of a Novel Treatment for Condylar Resorption After Orthognathic Surgery Using
de Souza Tesch et al. Stem Cell Research & Therapy (2018) 9:94 https://doi.org/10.1186/s13287-018-0806-4 RESEARCH Open Access Temporomandibular joint regeneration: proposal of a novel treatment for condylar resorption after orthognathic surgery using transplantation of autologous nasal septum chondrocytes, and the first human case report Ricardo de Souza Tesch1*, Esther Rieko Takamori1, Karla Menezes1, Rosana Bizon Vieira Carias1, Cláudio Leonardo Milione Dutra1, Marcelo de Freitas Aguiar2, Tânia Salgado de Sousa Torraca3, Alexandra Cristina Senegaglia4, Cármen Lúcia Kuniyoshi Rebelatto4, Debora Regina Daga4, Paulo Roberto Slud Brofman4 and Radovan Borojevic1 Abstract Background: Upon orthognathic mandibular advancement surgery the adjacent soft tissues can displace the distal bone segment and increase the load on the temporomandibular joint causing loss of its integrity. Remodeling of the condyle and temporal fossa with destruction of condylar cartilage and subchondral bone leads to postsurgical condylar resorption, with arthralgia and functional limitations. Patients with severe lesions are refractory to conservative treatments, leading to more invasive therapies that range from simple arthrocentesis to open surgery and prosthesis. Although aggressive and with a high risk for the patient, surgical invasive treatments are not always efficient in managing the degenerative lesions. Methods: We propose a regenerative medicine approach using in-vitro expanded autologous cells from nasal septum applied to the first proof-of-concept patient. After the required quality controls, the cells were injected into each joint by arthrocentesis. Results were monitored by functional assays and image analysis using computed tomography. Results: The cell injection fully reverted the condylar resorption, leading to functional and structural regeneration after 6 months. -

Temporomandibular Joint (TMJ) Disorder Surgery, Because Such Treatment Is Considered Dental in Nature And, Therefore, Not Covered Under the Medical Benefit
Cigna Medical Coverage Policy Effective Date ............................ 9/15/2014 Subject Temporomandibular Joint Next Review Date ...................... 9/15/2015 Coverage Policy Number ................. 0156 (TMJ) Disorder Surgery Table of Contents Hyperlink to Related Coverage Policies Coverage Policy .................................................. 1 Acupuncture General Background ........................................... 2 Continuous Passive Motion (CPM) Devices Coding/Billing Information ................................... 9 Orthognathic Surgery References ........................................................ 10 Stretch Devices for Joint Stiffness and Contracture INSTRUCTIONS FOR USE The following Coverage Policy applies to health benefit plans administered by Cigna companies. Coverage Policies are intended to provide guidance in interpreting certain standard Cigna benefit plans. Please note, the terms of a customer’s particular benefit plan document [Group Service Agreement, Evidence of Coverage, Certificate of Coverage, Summary Plan Description (SPD) or similar plan document] may differ significantly from the standard benefit plans upon which these Coverage Policies are based. For example, a customer’s benefit plan document may contain a specific exclusion related to a topic addressed in a Coverage Policy. In the event of a conflict, a customer’s benefit plan document always supersedes the information in the Coverage Policies. In the absence of a controlling federal or state coverage mandate, benefits are ultimately determined -
Technique Guide Orthognathic Surgery
Technique Guide Orthognathic Surgery Editor: Myron R. Tucker, DDS 1 Table of contents Table Table of contents Section I: Sagittal Ramus Osteotomy (BSSO or BSRO) for Advancement 3-12 Sagittal Ramus Osteotomy Multiple Modifications 3 Incision/Exposure 3 Superior/Medial, Osteotomy Cuts & Lateral/Vertical 4-5 Thin Ramus 5 Fixation 7-9 Technical Modifications for BSSO for Mandibular Setback 10-12 Section II: Transoral Vertical Ramus Osteotomy 13-15 Advantages/Considerations 13 Ramus Osteotomy Vertical Transoral Incision/Exposure 13-14 Osteotomies 14 Fixation 15 Recontouring proximal segment 15 Section III: Genioplasty 16-18 General Considerations 16 Incision/Exposure 16 Osteotomy 17 Fixation 18 Closure 18 Genioplasty Section IV: LeFort I Maxillary Osteotomy 19-27 Incision/Exposure 19 Osteotomies 19-24 Recontouring 22 Grafting 24 LeFort I Osteotomy Fixation 25-26 Closure 27 Technique guide: Orthognathic Surgery Table of contents 2 NL-SP-HSC-002NL-SP-HSC-002 - Sagittal - Sagittal Ramus, Ramus, Osteotomy, Osteotomy, Transoral Transoral Vertical Vertical Ramus Ramus Osteotomy, Osteotomy, Genioplasty, Genioplasty, and LeFortand LeFort I Osteotomy I Osteotomy Protocol Protocol SAGITTALSAGITTAL RAMUS RAMUS OSTEOTOMY OSTEOTOMY (BSSO (BSSO OR OR BSRO) BSRO) FOR FOR ADVANCEMENT ADVANCEMENT of contents Table NL-SP-HSC-002NL-SP-HSC-002Section - Sagittal - Sagittal I: Ramus, Ramus, Osteotomy, Osteotomy, Transoral Transoral Vertical Vertical Ramus Ramus Osteotomy, Osteotomy, Genioplasty, Genioplasty, and LeFortand LeFort I Osteotomy I Osteotomy Protocol -

Surgical Considerations of the TMJ
Surgical Considerations of the TMJ Peter B. Franco DMD, FACS Diplomate, American Board of Oral and Maxillofacial Surgery Fellow, American College of Surgeons Carolinas Center for Oral and Facial Surgery Surgical Options of the TMJ • Arthroscopy • Open Arthroplasty – Disk preservation – Diskectomy Surgical Options of TMJ • General Indications – Significant TMJ pain or dysfunction – Non-surgical therapy has failed – Radiographic evidence of disease Failure to manage associated myofascial pain and dysfunction lowers the rate of surgical success. Arthroscopic Arthroplasty • Biopsy of suspected lesions or disease • Confirmation of other diagnostic findings that may warrant surgical treatment • Unexplained persistent joint pain that is non-responsive to medical treatment Arthroscopic Arthroplasty Indications • Closed, locked articular disc • Painful popping joint • Adhesions • Perforated disc • Hypermobile joints • Inflammatory joint disease • Hypermobility • Degenerative Joint Disease • Traumatic Injuries • Suspected Infection Arthroscopic Arthroplasty Equipment • Video/monitoring equipment • Arthroscopic cannula, scissors, forceps, probes, shavers • Laser Arthroscopic Arthroplasty Equipment • Scope • Arthroscopic cannula, scissors, forceps, probes, shavers • Laser Arthroscopic Arthroplasty Equipment • Scope • Video/monitoring equipment • Laser Arthroscopic Arthroplasty Equipment • Scope • Video/monitoring equipment • Arthroscopic cannula, scissors, forceps, probes, shavers Arthroscopic Arthroplasty Equipment Arthroscopic Arthroplasty Arthroscopic -

Oral Pathology Final Exam Review Table Tuanh Le & Enoch Ng, DDS
Oral Pathology Final Exam Review Table TuAnh Le & Enoch Ng, DDS 2014 Bump under tongue: cementoblastoma (50% 1st molar) Ranula (remove lesion and feeding gland) dermoid cyst (neoplasm from 3 germ layers) (surgical removal) cystic teratoma, cyst of blandin nuhn (surgical removal down to muscle, recurrence likely) Multilocular radiolucency: mucoepidermoid carcinoma cherubism ameloblastoma Bump anterior of palate: KOT minor salivary gland tumor odontogenic myxoma nasopalatine duct cyst (surgical removal, rare recurrence) torus palatinus Mixed radiolucencies: 4 P’s (excise for biopsy; curette vigorously!) calcifying odontogenic (Gorlin) cyst o Pyogenic granuloma (vascular; granulation tissue) periapical cemento-osseous dysplasia (nothing) o Peripheral giant cell granuloma (purple-blue lesions) florid cemento-osseous dysplasia (nothing) o Peripheral ossifying fibroma (bone, cartilage/ ossifying material) focal cemento-osseous dysplasia (biopsy then do nothing) o Peripheral fibroma (fibrous ct) Kertocystic Odontogenic Tumor (KOT): unique histology of cyst lining! (see histo notes below); 3 important things: (1) high Multiple bumps on skin: recurrence rate (2) highly aggressive (3) related to Gorlin syndrome Nevoid basal cell carcinoma (Gorlin syndrome) Hyperparathyroidism: excess PTH found via lab test Neurofibromatosis (see notes below) (refer to derm MD, tell family members) mucoepidermoid carcinoma (mixture of mucus-producing and squamous epidermoid cells; most common minor salivary Nevus gland tumor) (get it out!) -

Oral Health and Disease
Downloaded from bmj.com on 19 August 2005 ABC of oral health: Oral health and disease Ruth Holt, Graham Roberts and Crispian Scully BMJ 2000;320;1652-1655 doi:10.1136/bmj.320.7250.1652 Updated information and services can be found at: http://bmj.com/cgi/content/full/320/7250/1652 These include: Rapid responses One rapid response has been posted to this article, which you can access for free at: http://bmj.com/cgi/content/full/320/7250/1652#responses You can respond to this article at: http://bmj.com/cgi/eletter-submit/320/7250/1652 Email alerting Receive free email alerts when new articles cite this article - sign up in the box at service the top right corner of the article Topic collections Articles on similar topics can be found in the following collections Dentistry and Oral Medicine (79 articles) Notes To order reprints of this article go to: http://www.bmjjournals.com/cgi/reprintform To subscribe to BMJ go to: http://bmj.bmjjournals.com/subscriptions/subscribe.shtml Clinical review Downloaded from bmj.com on 19 August 2005 ABC of oral health Oral health and disease Ruth Holt, Graham Roberts, Crispian Scully A healthy dentition and mouth is important to both quality of life and nutrition, and oral disease may affect systemic health, as Enamel covering crown Gingival crevice discussed in later articles in this series. (gingival sulcus) Dentine Development of the dentition Gingiva Pulp chamber Teeth form mainly from neuroectoderm and comprise a crown of insensitive enamel surrounding sensitive dentine and a root Periodontal ligament that has no enamel covering.