Multidimensional Inequality and Covid-19 in Brazil
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Considerations on the Testimony About the Brazilian Civil-Military
ISSN: 2317-2347 – v. 9, n. 2 (2020) Todo o conteúdo da RLR está licenciado sob Creative Commons Atribuição 4.0 Internacional Discursive remains: considerations on the testimony about the Brazilian Civil-Military Dictatorship / Restos discursivos: considerações acerca do testemunho sobre a Ditadura Civil-Militar Brasileira Juliene da Silva Marques * PhD student supported by CAPES and Master by the Postgraduate Program in Language Sciences at the University of the South of Santa Catarina - UNISUL. Professor at the Federal Institute of Education, Science and Technology of Rio Grande do Sul – IFRS. https://orcid.org/0000-0001-5347-8815 Diego Airoso da Motta** PhD in Sociology at the Federal University of Rio Grande do Sul (UFRGS), Porto Alegre, Brazil and Master's Degree in Social Science at the University of Vale do Rio dos Sinos (Unisinos). https://orcid.org/0000-0002-2238-3706 Received: May, 26th, 2020. Approved: June, 05th, 2020. How to cite this article: MARQUES, Juliene da Silva; MOTTA, Diego Airoso da. Discursive remains: considerations on the testimony about the Brazilian Civil-Military Dictatorship. Revista Letras Raras, Campina Grande, v. 9, n. 2, p. 110-, jun. 2020. ABSTRACT Considering the political manifestations over the past years regarding the request for a new military intervention, this article has as its object of investigation testimonies about the Brazilian Civil-Military Dictatorship and comments about them, which show how the senses about this period are resignified in the present time. Based on this materiality and its movements of sense, the objective of this research is to analyze how these testimonies are set in motion today. -

Annual Report and Accounts Year Ended 31 March 2021 British Tourist Authority - Trading As Visitbritain and Visitengland
Annual Report and Accounts Year Ended 31 March 2021 British Tourist Authority - Trading as VisitBritain and VisitEngland HC 476 SG/2021/153 BRITISH TOURIST AUTHORITY TRADING AS VISITBRITAIN & VISITENGLAND ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31 MARCH 2021 Presented to Parliament pursuant to Section 6(4) and Section 6(6) of the Development of Tourism Act 1969. Ordered by the House of Commons to be printed 14 July 2021 HC 476 SG/2021/153 © British Tourist Authority copyright 2021 This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3. Where we have identified any third-party copyright information you will need to obtain permission from the copyright holders concerned. This publication is available at www.gov.uk/official-documents. Any enquiries related to this publication should be sent to us at VisitBritain, 3 Grosvenor Gardens, London SW1W 0BD. ISBN 978-1-5286-2716-0 CCS0621804704 07/21 Printed on paper containing 75% recycled fibre content minimum. Printed in the UK by the APS Group on behalf of the Controller of Her Majesty’s Stationery Office. British Tourist Authority trading as VisitBritain and VisitEngland Annual Report and Financial Statements for the Year Ended 31 March 2021 TABLE OF CONTENTS TABLE OF CONTENTS ..............................................................................................................1 Chairman’s Foreword ....................................................................................................2 -

Ter/Haver-Existential Clauses in Brazilian Portuguese: Variation and Change
DOCUMENT RESUME ED 457 686 FL 026 908 AUTHOR Callou, Dinah TITLE Ter/Haver-Existential Clauses in Brazilian Portuguese: Variation and Change. PUB DATE 2001-00-00 NOTE 10p. PUB TYPE Information Analyses (070) LANGUAGE English, Portuguese EDRS PRICE MF01/PC01 Plus Postage. DESCRIPTORS Diachronic Linguistics; Dialects; English; Foreign Countries; French; *Grammar; Language Variation; *Portuguese; Pronunciation; Second Language Instruction; Second Language Learning; *Sentence Structure; Uncommonly Taught Languages; *Verbs IDENTIFIERS *Brazil; *Portuguese (Brazilian) ABSTRACT This paper discusses the details of existential sentences constructed with the Portuguese verbs "ter" and "haver" in the interpersonal form. The uses of these verbs are discussed and analyzed in detail. The history and evolution of linguistic changes in Brazilian Portuguese are discussed in an attempt to detect historical social and cultural factors responsible for the variation in existential sentences. (Contains 15 references.) (KFT) Reproductions supplied by EDRS are the best that can be made from the original document. U.S. DEPARTMENT OF EDUCATION Office of Educational Research and Improvement PERMISSION TO REPRODUCE AND ED J CATIONAL RESOURCES INFORMATION DISSEMINATE THIS MATERIAL HAS CENTER (ERIC) BEEN GRANTED BY This document has been reproduced as received from the person or organization originating it. 0 Minor changes have been made to amyl. Ccitiour improve reproduction quality. Points of view or opinions stated in this TO THE EDUCATIONAL RESOURCES document do not necessarily represent INFORMATION CENTER (ERIC) official OERI position or policy. 1 Ter/haver-existential clauses in Brazilian Portuguese: variation ad changei Dinah Callon (UFRJ/CNN-Brazil) 1.Introduction Generally, the label "existential sentence" denotes the there is/are constructions and its equivalents in other languages. -
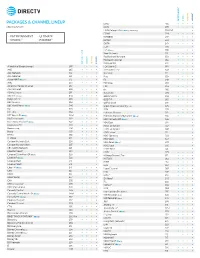
Packages & Channel Lineup
™ ™ ENTERTAINMENT CHOICE ULTIMATE PREMIER PACKAGES & CHANNEL LINEUP ESNE3 456 • • • • Effective 6/17/21 ESPN 206 • • • • ESPN College Extra2 (c only) (Games only) 788-798 • ESPN2 209 • • • • • ENTERTAINMENT • ULTIMATE ESPNEWS 207 • • • • CHOICE™ • PREMIER™ ESPNU 208 • • • EWTN 370 • • • • FLIX® 556 • FM2 (c only) 386 • • Food Network 231 • • • • ™ ™ Fox Business Network 359 • • • • Fox News Channel 360 • • • • ENTERTAINMENT CHOICE ULTIMATE PREMIER FOX Sports 1 219 • • • • A Wealth of Entertainment 387 • • • FOX Sports 2 618 • • A&E 265 • • • • Free Speech TV3 348 • • • • ACC Network 612 • • • Freeform 311 • • • • AccuWeather 361 • • • • Fuse 339 • • • ActionMAX2 (c only) 519 • FX 248 • • • • AMC 254 • • • • FX Movie 258 • • American Heroes Channel 287 • • FXX 259 • • • • Animal Planet 282 • • • • fyi, 266 • • ASPiRE2 (HD only) 381 • • Galavisión 404 • • • • AXS TV2 (HD only) 340 • • • • GEB America3 363 • • • • BabyFirst TV3 293 • • • • GOD TV3 365 • • • • BBC America 264 • • • • Golf Channel 218 • • 2 c BBC World News ( only) 346 • • Great American Country (GAC) 326 • • BET 329 • • • • GSN 233 • • • BET HER 330 • • Hallmark Channel 312 • • • • BET West HD2 (c only) 329-1 2 • • • • Hallmark Movies & Mysteries (c only) 565 • • Big Ten Network 610 2 • • • HBO Comedy HD (c only) 506 • 2 Black News Channel (c only) 342 • • • • HBO East 501 • Bloomberg TV 353 • • • • HBO Family East 507 • Boomerang 298 • • • • HBO Family West 508 • Bravo 237 • • • • HBO Latino3 511 • BYUtv 374 • • • • HBO Signature 503 • C-SPAN2 351 • • • • HBO West 504 • -

How to Bring About Forest-Smart Mining: Strategic Entry Points for Institutional Donors
How to bring about forest-smart mining: strategic entry points for institutional donors November 2020 How to bring about forest-smart mining: strategic entry points for institutional donors November 2020 About this report: The World Bank’s PROFOR Trust Fund developed the concept of Forest-Smart Mining in 2017 to raise awareness of different economic sectors’ impacts upon forest health and forest values, such as biodiversity, ecosystem services, human development, supporting and regulating services and cultural values. From 2017 to 2019, Levin Sources, Fauna and Flora International, Swedish Geological AB, and Fairfields Consulting were commissioned by the World Bank/PROFOR Trust fund to investigate good and bad practices of all scales of mining in forest landscapes, and the contextual conditions that support ‘forest-smart’ mining. Three reports and an Executive Summary were published in May 2019, further to a series of events and launches in New York, Geneva, and London which have led to related publications. This report was commissioned by a philanthropic foundation to provide an analysis of the key initiatives and stakeholders working to address the negative impacts of mining on forests. The purpose of the report is to provide a menu of recommendations to inform the development of a new program to bring about forest-smart mining. In the interest of raising awareness and stimulating appetite and action by other institutional donors to step into this space, the client has permitted Levin Sources and Fauna & Flora International to further develop and publish the report. We would like to thank the client for the opportunity to do so. -

U.S.-Brazil Connect Summit
8:30 am Ernesto Torres Cantú, CEO, Citigroup Latin America, and Chair, Brazil-U.S. Business Council Cassia Carvalho, Executive Director, Brazil-U.S. Business Council, U.S. Chamber of Commerce 8:35 am 8:45 am Strengthening U.S.-Brazil Cooperation in Times of Pandemic Secretary Michael R. Pompeo, United States Secretary of State Minister Ernesto Araújo, Ministry of Foreign Relations of the Federative Republic of Brazil Introduced by: Marc Allen, Chief Strategy Officer and Senior Vice President, Strategy and Corporate Development, The Boeing Company, and Vice Chair, Brazil- U.S. Business Council Moderated by: Myron Brilliant, Executive Vice President and Head of International Affairs, U.S. Chamber of Commerce 9:05 am Introduced by: Myron Brilliant, Executive Vice President and Head of International Affairs, U.S. Chamber of Commerce 9:15 am Introduced/Moderated by: Ernesto Torres Cantú, CEO, Citigroup Latin America, and Chair, Brazil-U.S. Business Council 9:45 am How to Build a Sustainable and Inclusive Economy in Brazil: What are the Priorities? Roberto Fendt, Deputy-Minister for Foreign Trade and International Affairs, Ministry of Economy of the Federative Republic of Brazil Otaviano Canuto, Senior Fellow, Policy Center for the New South Moderated by: Cassia Carvalho, Executive Director, Brazil-U.S. Business Council, U.S. Chamber of Commerce 10:10 am Vitor Menezes, Secretary of Telecommunications, Ministry of Communications Artur Coimbra, Director of the Department of Broadband, Ministry of Communications Whit Richardson, President, WarnerMedia Entertainment Networks, Latin America Moderated by: Karim Lesina, Senior Vice President, International External and Regulatory Affairs, AT&T and Vice Chair, Brazil-U.S. -

Brazil the Timeline of the Federal Government's
BRAZIL THE TIMELINE OF THE FEDERAL GOVERNMENT’S STRATEGY TO SPREAD COVID-19 São Paulo, 28th May 2021. Study prepared within the scope of research project ““RIGHTS IN THE PANDEMIC - Mapping the impact of Covid-19 on human rights in Brazil” of the Centre for Studies and Research on Health Law (CEPEDISA) of the School of Public Health (FSP) of the University of São Paulo (USP)”, updated at the request of the parliamentary committee of inquiry created by Federal Senate Requests 1371 and 1372, of 2021, by means of Official Letter 57/2021- CPIPANDEMIA. EXECUTIVE SUMMARY 1. This study is part of research project ““RIGHTS IN THE PANDEMIC - Mapping the impact of Covid-19 on human rights in Brazil” of the Centre for Studies and Research on Health Law (CEPEDISA) of the School of Public Health (FSP) of the University of São Paulo (USP)”, carried out in partnership with Non-Governmental Organization “Conectas Direitos Humanos” until January 2021 and, since then, with the National Council of Health Secretaries (CONASS), with the aim of collecting federal and state regulations relating to Covid-19 and assessing their impact on human rights in Brazil. The partnership entered into with CONASS refers to the mapping and analysis of rules drawn up by the State and Federal District Health Offices and is restricted to the scope of health policies during the Covid-19 pandemic. The timeline of the federal government’s strategy to spread Covid-19 was first published in January 2021, and has now been updated at the request of the Federal Senate's Parliamentary Committee of Inquiry on Covid-19. -

Sky Launches More Than 70 Channels for Its Subscribers
PRESS RELEASE Sky launches more than 70 channels for its subscribers In support of the recommendation asking the general public to stay home in order to be able to contain the spread of the new Coronavirus, the operator has given access to its programming on various channels and at no additional cost. São Paulo, March 15, 2020 - With the evolution of the new Corona virus (Covid-19), SKY, the country's largest satellite television operator, announces that starting today, it will open the signal to channels of different genres for all its clients and at no additional cost. The initiative aims to bring content, information and entertainment to those who will be at home in the cities of all municipalities in the country. All the channels will have an open linear TV-signal among them and in some channels the users will also be able to watch live-TV via streaming transmitted on SKY Play, the company's on demand platform video service. See below all the channels that will be available. Thereafter, new channels may be added as well. SKY also points out that depending on the available workforce some occasional problems might arise for on-site or for customer services. The company is monitoring and prioritizing the well-being of its employees and partners. Open Signals - On TV • A&E, AMC, Animal Planet, Arte 1, AXN, Band News, Band Sports, BBC, Bis, Boomerang, Canal Brasil, Cartoon Network, Cinemax, Climatempo, CNN, CNN Brasil, Comedy Central, Discovery, Discovery H&H, Discovery ID , Discovery Science, Discovery World, Discovery Kids, Discovery Theater, Discovery Turbo, E!, Fashion TV, Fish TV, Food Network, GloboNews, Gloob, Gloobinho, GNT, Golf, H2, HGTV, History, Lifetime, More Globosat, Megapix , MTV, Multishow, Nick Jr, Nickelodeon, OFF, Paramount, PlayTV, Prime Box Brazil, Sony Channel, Space, SPORTV, SPORTV 2, SPORTV 3, Studio Universal, Sundance, SyFy, TBS, TCM, Telecine Premium, Telecine Action, Telecine Fun, Telecine Touch, Telecine Popcorn, Telecine Cult, TLC, TNT, TNT Series, ToonCast, Tru TV, Universal Channel, Viva, Warner Channel, Woohoo, ZooMoo. -

Arab Geopolitics 2020: the Perspectives in a Dynamic Middle East, What Kind of Neighborhood Future?
POLICY CENTER FOR THE NEW SOUTH ACTIVITY REPORT 2020 POLICY CENTER FOR THE NEW SOUTH ACTIVITY REPORT 2020 TABLE OF CONTENTS Introduction .....................................................................................06 In Sum ................................................................................................08 COVID-19 Program ...................................................................... 10 A Few Key Figures ..........................................................................12 Annual Events .................................................................................14 Think .................................................... 19 Our Publications & Opinions ................................................20 Economy ......................................................................................24 International Relations ..........................................................30 Media Focus ...............................................................................34 Stimulate ...............................................37 Atlantic Dialogues Emerging leaders .............................38 Internship Program ................................................................43 Bridge .................................................. 45 International Events ..............................................................48 National Events .......................................................................53 Events in Partnership ............................................................56 -

Learning Reimagined: RADICAL THINKING for EQUITABLE FUTURES LEARNING REIMAGINED | AUGUST 2020
Learning Reimagined: RADICAL THINKING FOR EQUITABLE FUTURES LEARNING REIMAGINED | AUGUST 2020 BIG PICTURE 2 Our known systems, everyday Given the enormity of changes, we purposely pulled out of our routines and relationships typical areas of focus to better understand even broader possible implications for children, families, educators and more. have been radically disrupted. While reports can feel like a sealed chamber, we’ve designed this as This report, which came out of a partnership between Imaginable an open invitation for dialogue. Which of these scenarios do we Futures and IDEO, sets out to capture the global disruption of our strive to avoid, and how? Which are an inspiring call to action? In education systems and to offer an evidence-based vision of the articulating broad opportunity areas, we hope to hear from global future, that takes into account both the constraints and the communities with diverse perspectives about how they would opportunities of this historic moment. It references a moment in adapt these ideas. Our hope is that we might collectively imagine a time, amidst a rapidly changing world; as our ecosystems continue better future and begin thinking about what it will take to get to evolve at unprecedented rates, so will the insights in this report. there. To arrive at these insights, we have leveraged the tools of design We also acknowledge that we are standing on the shoulders of fiction and futuring: analyzing the drivers of change (a global giants. This report would not exist without those who have long pandemic and economic fallout, and movements towards racial invested in building and improving our education systems: justice), citing early signals of hope (the heroic response of teachers, school leaders and caregivers alike. -
CHANGES in the GLOBAL and BRAZILIAN AUDIOVISUAL MARKET Competitive Dynamics, Impact on Consumer Welfare, and Implications for Public Policy and Competition Model
CHANGES IN THE GLOBAL AND BRAZILIAN AUDIOVISUAL MARKET Competitive dynamics, impact on consumer welfare, and implications for public policy and competition model October 2019 1 Author § Raul Katz (Ph.D., Management Science and Political Science, Massachusetts Institute of Technology) is currently Director of Business Strategy Research at the Columbia Institute for Tele-Information, and President of Telecom Advisory Services, LLC (URL: www.teleadvs.com). Before founding Telecom Advisory Services, he worked for twenty years at Booz Allen Hamilton, where he was the Head of the Telecommunications Practice in North and Latin America and member of its Leadership Team. Telecom Advisory Services LLC (TAS) is an international consulting firm specialized in the development of business strategies and public policies for digital and telecommunications companies, governments, and international organizations. Its clients include leading companies in the digital and telecommunications sectors, as well as international organizations such as the International Telecommunications Union, the World Bank, the Inter-American Development Bank, the World Economic Forum, the UN Economic Commission for Latin America and the Caribbean, the GSMA Association, the CTIA, the NCTA, Cable Europe, and the FTTH Council (Europe). In addition, TAS has conducted projects for the governments of Argentina, Brazil, Colombia, Costa Rica, Ecuador, Mexico, and Peru. This study was funded by AT&T. All of the study’s content, including its conclusions, are the independent outcome of the analysis conducted solely by the author and Telecom Advisory Services 2 TABLE OF CONTENTS EXECUTIVE SUMMARY I. INTRODUCTION II. INDUSTRY DYNAMICS IN THE GLOBAL AUDIOVISUAL INDUSTRY II.1. The historical evolution of the audiovisual value chain II.1.1. -

DIRECTV GO Arrives in Brazil
DIRECTV GO arrives in Brazil Brazilians now have access to the best of TV and streaming together, without the need for a contract or service installation. Content partners include Grupo Globo, HBO, Disney, Turner, Viacom, Discovery Networks, Record, SBT and Band Consumers who join the new service in the first month of the launch will receive 5-year access to HBO channels São Paulo, December 1, 2020 – Vrio Corp.,a leading digital entertainment services company in Latin America, announced the launch of DIRECTV GO in Brazil starting today. A pioneer and unique service in the Brazilian market, the platform combines the best of the live national and international programming with streaming content. The offer satisfies the needs of today's multiscreen consumers, who are looking for convenience and freedom to access a wide variety of content in one place. Users will be able to sign up at www.DIRECTVGO.com.br without a physical or printed contract or service installation; simply requires an internet connection1. DIRECTV GO offers more than 90 channels, including live Brazilian television programming from Rede Globo de Televisão, RECORD TV, SBT, Band and Rede TV!. In addition, it includes sports and live championship content (SporTV, FOX Sports, ESPN BR, SporTV 2, SporTV 3, ESPN, FOX Sports 2, BandSports e ESPN 2), channels dedicated to film with thousands of movies and series (Megapix, TNT, Space, Cinemax, Studio Universal, Paramount Channel, AXN, Universal Channel e Warner Channel), and children’s channels (Cartoon Network, Discovery Kids, Gloob, Nickelodeon, Nick Jr., Boomerang, Disney Channel, Nat Geo Kids). News (GloboNews, CNN Brasil and BandNews) and channels focused in music, science, documentaries and entertainment are also available.