Abbreviations
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Improving the Quality of Life of the Elderly and Disabled
IMPROVING THE QUALITY OF LIFE OF THE ELDERLY AND DISABLED PEOPLE IN HUMAN SETTLEMENTS IMPROVING THE QUALITY OF LIFE OF ELDERLY AND DISABLED PEOPLE IN HUMAN SETTLEMENTS VOLUME I A Resource Book of Policy and Programmes from around the World United Nations Centre for Human Settlements (Habitat) Nairobi, 1993 HS/284/93E ISBN 92-1-131208-6 FOREWORD The world's population is ageing dramatically. The total number of people aged 60 and older grew from 200 million in 1950 to 400 million in 1982. Their number is expected to increase to 600 million in the year 2001 when 70 per cent of them will live in developing countries. This demographic revolution has major consequences on the way human settlements are designed, managed and used. The United Nations and its agencies have undertaken many activities that recognize this reality. The General Assembly adopted the World Programme of Action concerning Disabled Persons and proclaimed 1981 the International Year of Disabled Persons. In 1982, 124 Member States adopted the International Plan of Action on Aging at the World Assembly on Aging. These two landmark events launched a variety of activities and studies during the United Nations Decade of Elderly and Disabled Persons. The United Nations Centre for Human Settlements (Habitat) launched the decade with two important documents. Designing with Care - a Guide to Adaptation of the Built Environment for Disabled Persons was published as the result of cooperation between the United Nations, UNCHS (Habitat) and the Swedish International Development Agency (SIDA). This guide pointed out that implementation of suggested design guidelines and related policies and programmes would have to be undertaken by authorities, taking into consideration the economic, social and climatic conditions of the human settlement concerned. -

How Can We Create Environments Where Hate Cannot Flourish?
How can we create environments where hate cannot flourish? Saturday, February 1 9:30 a.m. – 10:00 a.m. Check-In and Registration Location: Field Museum West Entrance 10:00 a.m. – 10:30 a.m. Introductions and Program Kick-Off JoAnna Wasserman, USHMM Education Initiatives Manager Location: Lecture Hall 1 10:30 a.m. – 11:30 a.m. Watch “The Path to Nazi Genocide” and Reflections JoAnna Wasserman, USHMM Education Initiatives Manager Location: Lecture Hall 1 11:30 a.m. – 11:45 a.m. Break and walk to State of Deception 11:45 a.m. – 12:30 p.m. Visit State of Deception Interpretation by Holocaust Survivor Volunteers from the Illinois Holocaust Museum Location: Upper level 12:30 p.m. – 1:00 p.m. Breakout Session: Reflections on Exhibit Tim Kaiser, USHMM Director, Education Initiatives David Klevan, USHMM Digital Learning Strategist JoAnna Wasserman, USHMM Education Initiatives Manager Location: Lecture Hall 1, Classrooms A and B Saturday, February 2 (continued) 1:00 p.m. – 1:45 p.m. Lunch 1:45 p.m. – 2:45 p.m. A Survivor’s Personal Story Bob Behr, USHMM Survivor Volunteer Interviewed by: Ann Weber, USHMM Program Coordinator Location: Lecture Hall 1 2:45 p.m. – 3:00 p.m. Break 3:00 p.m. – 3:45 p.m. Student Panel: Beyond Indifference Location: Lecture Hall 1 Moderator: Emma Pettit, Sustained Dialogue Campus Network Student/Alumni Panelists: Jazzy Johnson, Northwestern University Mary Giardina, The Ohio State University Nory Kaplan-Kelly, University of Chicago 3:45 p.m. – 4:30 p.m. Breakout Session: Sharing Personal Reflections Tim Kaiser, USHMM Director, Education Initiatives David Klevan, USHMM Digital Learning Strategist JoAnna Wasserman, USHMM Education Initiatives Manager Location: Lecture Hall 1, Classrooms A and B 4:30 p.m. -

Blockage of Neddylation Modification Stimulates Tumor Sphere Formation
Blockage of neddylation modification stimulates tumor PNAS PLUS sphere formation in vitro and stem cell differentiation and wound healing in vivo Xiaochen Zhoua,b,1, Mingjia Tanb,1, Mukesh K. Nyatib, Yongchao Zhaoc,d, Gongxian Wanga,2, and Yi Sunb,c,e,2 aDepartment of Urology, The First Affiliated Hospital of Nanchang University, Nanchang, Jiangxi 330006, China; bDivision of Radiation and Cancer Biology, Department of Radiation Oncology, University of Michigan, Ann Arbor, MI 48109; cInstitute of Translational Medicine, Zhejiang University School of Medicine, Hangzhou, Zhejiang 310029, China; dKey Laboratory of Combined Multi-Organ Transplantation, Ministry of Public Health, First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou 310058, China; and eCollaborative Innovation Center for Diagnosis and Treatment of Infectious Diseases, Zhejiang University, Hangzhou 310058, China Edited by Vishva M. Dixit, Genentech, San Francisco, CA, and approved March 10, 2016 (received for review November 13, 2015) MLN4924, also known as pevonedistat, is the first-in-class inhibitor acting alone or in combination with current chemotherapy of NEDD8-activating enzyme, which blocks the entire neddylation and/or radiation (6, 11). One of the seven clinical trials of MLN4924 modification of proteins. Previous preclinical studies and current (NCT00911066) was published recently, concluding a modest effect clinical trials have been exclusively focused on its anticancer property. of MLN4924 against acute myeloid leukemia (AML) (12). Unexpectedly, we show here, to our knowledge for the first time, To further elucidate the role of blocking neddylation in cancer that MLN4924, when applied at nanomolar concentrations, signif- treatment, we thought to study the effect of MLN4924 on cancer icantly stimulates in vitro tumor sphere formation and in vivo stem cells (CSCs) or tumor-initiating cells (TICs), a small group tumorigenesis and differentiation of human cancer cells and mouse of tumor cells with stem cell properties that have been claimed to embryonic stem cells. -
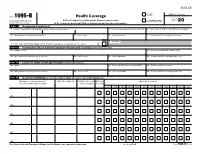
Form 1095-B Health Coverage Department of the Treasury ▶ Do Not Attach to Your Tax Return
560118 VOID OMB No. 1545-2252 Form 1095-B Health Coverage Department of the Treasury ▶ Do not attach to your tax return. Keep for your records. CORRECTED 2020 Internal Revenue Service ▶ Go to www.irs.gov/Form1095B for instructions and the latest information. Part I Responsible Individual 1 Name of responsible individual–First name, middle name, last name 2 Social security number (SSN) or other TIN 3 Date of birth (if SSN or other TIN is not available) 4 Street address (including apartment no.) 5 City or town 6 State or province 7 Country and ZIP or foreign postal code 9 Reserved 8 Enter letter identifying Origin of the Health Coverage (see instructions for codes): . ▶ Part II Information About Certain Employer-Sponsored Coverage (see instructions) 10 Employer name 11 Employer identification number (EIN) 12 Street address (including room or suite no.) 13 City or town 14 State or province 15 Country and ZIP or foreign postal code Part III Issuer or Other Coverage Provider (see instructions) 16 Name 17 Employer identification number (EIN) 18 Contact telephone number 19 Street address (including room or suite no.) 20 City or town 21 State or province 22 Country and ZIP or foreign postal code Part IV Covered Individuals (Enter the information for each covered individual.) (a) Name of covered individual(s) (b) SSN or other TIN (c) DOB (if SSN or other (d) Covered (e) Months of coverage First name, middle initial, last name TIN is not available) all 12 months Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec 23 24 25 26 27 28 For Privacy Act and Paperwork Reduction Act Notice, see separate instructions. -

State of New Physics in B->S Transitions
New physics in b ! s transitions after LHC run 1 Wolfgang Altmannshofera and David M. Straubb a Perimeter Institute for Theoretical Physics, 31 Caroline St. N, Waterloo, Ontario, Canada N2L 2Y5 b Excellence Cluster Universe, TUM, Boltzmannstr. 2, 85748 Garching, Germany E-mail: [email protected], [email protected] We present results of global fits of all relevant experimental data on rare b s decays. We observe significant tensions between the Standard Model predictions! and the data. After critically reviewing the possible sources of theoretical uncer- tainties, we find that within the Standard Model, the tensions could be explained if there are unaccounted hadronic effects much larger than our estimates. Assuming hadronic uncertainties are estimated in a sufficiently conservative way, we discuss the implications of the experimental results on new physics, both model indepen- dently as well as in the context of the minimal supersymmetric standard model and models with flavour-changing Z0 bosons. We discuss in detail the violation of lepton flavour universality as hinted by the current data and make predictions for additional lepton flavour universality tests that can be performed in the future. We find that the ratio of the forward-backward asymmetries in B K∗µ+µ− and B K∗e+e− at low dilepton invariant mass is a particularly sensitive! probe of lepton! flavour universality and allows to distinguish between different new physics scenarios that give the best description of the current data. Contents 1. Introduction2 2. Observables and uncertainties3 2.1. Effective Hamiltonian . .4 2.2. B Kµ+µ− .....................................4 2.3. B ! K∗µ+µ− and B K∗γ ............................6 ! + − ! 2.4. -

Folkloristic Understandings of Nation-Building in Pakistan
Folkloristic Understandings of Nation-Building in Pakistan Ideas, Issues and Questions of Nation-Building in Pakistan Research Cooperation between the Hanns Seidel Foundation Pakistan and the Quaid-i-Azam University Islamabad Islamabad, 2020 Folkloristic Understandings of Nation-Building in Pakistan Edited by Sarah Holz Ideas, Issues and Questions of Nation-Building in Pakistan Research Cooperation between Hanns Seidel Foundation, Islamabad Office and Quaid-i-Azam University Islamabad, Pakistan Acknowledgements Thank you to Hanns Seidel Foundation, Islamabad Office for the generous and continued support for empirical research in Pakistan, in particular: Kristóf Duwaerts, Omer Ali, Sumaira Ihsan, Aisha Farzana and Ahsen Masood. This volume would not have been possible without the hard work and dedication of a large number of people. Sara Gurchani, who worked as the research assistant of the collaboration in 2018 and 2019, provided invaluable administrative, organisational and editorial support for this endeavour. A big thank you the HSF grant holders of 2018 who were not only doing their own work but who were also actively engaged in the organisation of the international workshop and the lecture series: Ibrahim Ahmed, Fateh Ali, Babar Rahman and in particular Adil Pasha and Mohsinullah. Thank you to all the support staff who were working behind the scenes to ensure a smooth functioning of all events. A special thanks goes to Shafaq Shafique and Muhammad Latif sahib who handled most of the coordination. Thank you, Usman Shah for the copy editing. The research collaboration would not be possible without the work of the QAU faculty members in the year 2018, Dr. Saadia Abid, Dr. -

Medicare 2019 Part C & D Star Ratings Cut Point Trends
Trends in Part C & D Star Rating Measure Cut Points Updated – 12/19/2018 (Last Updated 12/19/2018) Page 1 Document Change Log Previous Revision Version Description of Change Date - Final release of the 2019 Star Ratings Cut Point Trend document 12/19/2018 (Last Updated 12/19/2018) Page i Table of Contents DOCUMENT CHANGE LOG .............................................................................................................................. I TABLE OF CONTENTS .................................................................................................................................... II INTRODUCTION ............................................................................................................................................... 1 PART C MEASURES ........................................................................................................................................ 2 Measure: C01 - Breast Cancer Screening ........................................................................................................................ 2 Measure: C02 - Colorectal Cancer Screening .................................................................................................................. 3 Measure: C03 - Annual Flu Vaccine .................................................................................................................................. 4 Measure: C04 - Improving or Maintaining Physical Health ........................................................................................... -
Persian Language
v course reference persian language r e f e r e n c e زبان فارسی The Persian Language 1 PERSIAN OR FARSI? In the U.S., the official language of Iran is language courses in “Farsi,” universities and sometimes called “Farsi,” but sometimes it is scholars prefer the historically correct term called “Persian.” Whereas U.S. government “Persian.” The term “Farsi” is better reserved organizations have traditionally developed for the dialect of Persian used in Iran. 2 course reference AN INDO-EUROPEAN LANGUAGE Persian is a member of the Indo-European Persian has three major dialects: Farsi, language family, which is the largest in the the official language of Iran, spoken by 50 world. percent of the population; Dari, spoken mostly in Afghanistan, and Tajiki, spoken Persian falls under the Indo-Iranian branch, in Tajikistan. Other languages in Iran are comprising languages spoken primarily Arabic, New Aramaic, Armenian, Georgian in Afghanistan, Iran, Pakistan, India, and Turkic dialects such as Azerbaidjani, Bangladesh, areas of Turkey and Iraq, and Khalaj, Turkemenian and Qashqa”i. some of the former Soviet Union. INDO-EUROPEAN LANGUAGES GERMANIC INDO-IRANIAN HELLENIC CELTIC ITALIC BALTO-SLAVIC Polish Russin Indic Greek Serbo-Crotin North Germnic Ltin Irnin Mnx Irish Welsh Old Norse Swedish Scottish Avestn Old Persin Icelndic Norwegin French Spnish Portuguese Itlin Middle Persin West Germnic Snskrit Rumnin Ctln Frsi Kurdish Bengli Urdu Gujrti Hindi Old High Germn Old Dutch Anglo-Frisin Middle High Germn Middle Dutch Old Frisin Old English Germn Flemish Dutch Afrikns Frisin Middle English Yiddish Modern English vi v Persian Language 3 ALPHABET: FROM PAHLAVI TO ARABIC History tells us that Iranians used the Pahlavi Unlike English, Persian is written from right writing system prior to the 7th Century. -

Considerations About Semitic Etyma in De Vaan's Latin Etymological Dictionary
applyparastyle “fig//caption/p[1]” parastyle “FigCapt” Philology, vol. 4/2018/2019, pp. 35–156 © 2019 Ephraim Nissan - DOI https://doi.org/10.3726/PHIL042019.2 2019 Considerations about Semitic Etyma in de Vaan’s Latin Etymological Dictionary: Terms for Plants, 4 Domestic Animals, Tools or Vessels Ephraim Nissan 00 35 Abstract In this long study, our point of departure is particular entries in Michiel de Vaan’s Latin Etymological Dictionary (2008). We are interested in possibly Semitic etyma. Among 156 the other things, we consider controversies not just concerning individual etymologies, but also concerning approaches. We provide a detailed discussion of names for plants, but we also consider names for domestic animals. 2018/2019 Keywords Latin etymologies, Historical linguistics, Semitic loanwords in antiquity, Botany, Zoonyms, Controversies. Contents Considerations about Semitic Etyma in de Vaan’s 1. Introduction Latin Etymological Dictionary: Terms for Plants, Domestic Animals, Tools or Vessels 35 In his article “Il problema dei semitismi antichi nel latino”, Paolo Martino Ephraim Nissan 35 (1993) at the very beginning lamented the neglect of Semitic etymolo- gies for Archaic and Classical Latin; as opposed to survivals from a sub- strate and to terms of Etruscan, Italic, Greek, Celtic origin, when it comes to loanwords of certain direct Semitic origin in Latin, Martino remarked, such loanwords have been only admitted in a surprisingly exiguous num- ber of cases, when they were not met with outright rejection, as though they merely were fanciful constructs:1 In seguito alle recenti acquisizioni archeologiche ed epigrafiche che hanno documen- tato una densità finora insospettata di contatti tra Semiti (soprattutto Fenici, Aramei e 1 If one thinks what one could come across in the 1890s (see below), fanciful constructs were not a rarity. -

Grading System the Grades of A, B, C, D and P Are Passing Grades
Grading System The grades of A, B, C, D and P are passing grades. Grades of F and U are failing grades. R and I are interim grades. Grades of W and X are final grades carrying no credit. Individual instructors determine criteria for letter grade assignments described in individual course syllabi. Explanation of Grades The quality of performance in any academic course is reported by a letter grade, assigned by the instructor. These grades denote the character of study and are assigned quality points as follows: A Excellent 4 grade points per credit B Good 3 grade points per credit C Average 2 grade points per credit D Poor 1 grade point per credit F Failure 0 grade points per credit I Incomplete No credit, used for verifiable, unavoidable reasons. Requirements for satisfactory completion are established through student/faculty consultation. Courses for which the grade of I (incomplete) is awarded must be completed by the end of the subsequent semester or another grade (A, B, C, D, F, W, P, R, S and U) is awarded by the instructor based upon completed course work. In the case of I grades earned at the end of the spring semester, students have through the end of the following fall semester to complete the requirements. In exceptional cases, extensions of time needed to complete course work for I grades may be granted beyond the subsequent semester, with the written approval of the vice president of learning. An I grade can change to a W grade only under documented mitigating circumstances. The vice president of learning must approve the grade change. -

Hepatitis A, B, and C: Learn the Differences
Hepatitis A, B, and C: Learn the Differences Hepatitis A Hepatitis B Hepatitis C caused by the hepatitis A virus (HAV) caused by the hepatitis B virus (HBV) caused by the hepatitis C virus (HCV) HAV is found in the feces (poop) of people with hepa- HBV is found in blood and certain body fluids. The virus is spread HCV is found in blood and certain body fluids. The titis A and is usually spread by close personal contact when blood or body fluid from an infected person enters the body virus is spread when blood or body fluid from an HCV- (including sex or living in the same household). It of a person who is not immune. HBV is spread through having infected person enters another person’s body. HCV can also be spread by eating food or drinking water unprotected sex with an infected person, sharing needles or is spread through sharing needles or “works” when contaminated with HAV. “works” when shooting drugs, exposure to needlesticks or sharps shooting drugs, through exposure to needlesticks on the job, or from an infected mother to her baby during birth. or sharps on the job, or sometimes from an infected How is it spread? Exposure to infected blood in ANY situation can be a risk for mother to her baby during birth. It is possible to trans- transmission. mit HCV during sex, but it is not common. • People who wish to be protected from HAV infection • All infants, children, and teens ages 0 through 18 years There is no vaccine to prevent HCV. -

DOCUMENT RESUME Essential Skills for the Care Team. A
DOCUMENT RESUME ED 419 937 CE 076 574 TITLE Essential Skills for the Care Team. A Program for New Employees in Residential and Home Care. INSTITUTION State Univ. of New York, Albany. Rockefeller Coll.; Eddy/Northeast Health, Troy, NY. SPONS AGENCY Office of Vocational and Adult Education (ED), Washington, DC. National Workplace Literacy Program. PUB DATE 1998-00-00 NOTE 456p.; For a related document, see CE 076 575. CONTRACT V198A40098-96 PUB TYPE GuideS Classroom Teacher (052) EDRS PRICE MF01/PC19 Plus Postage. DESCRIPTORS Adult Basic Education; Allied Health Occupations Education; Classroom Techniques; Competence; Competency Based Education; *Home Health Aides; *Nurses Aides; *On the Job Training; Postsecondary Education; Teaching Methods; Units of Study; *Workplace Literacy ABSTRACT This document contains modules for two types of training. It provides 20 hours of training to newly hired Nursing Assistant Trainees (NATs) in residential care settings preparing to become state Certified Nursing Assistants (CNAs), using eight stand-alone modules supported by training process guides. It also includes 7 hours of training for newly hired NATs in the home care settings preparing to become state certified Home Health Aides (HHAs), using five stand-alone modules with training process guides. The materials are suitable for workplace literacy programs for adults with low levels of English literacy skills. A learning strategies module serves as an introduction to both programs. The CNA program contains the following modules: understanding your