The Pulmonary Microbiome, Mechanical Ventilation, and Trauma
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Bacteriophages: Ecology and Applications Ramin Mazaheri Nezhad Fard 1,2*
Iranian Journal of Virology 2018;12(2): 41-56 ©2018, Iranian Society of Virology Review Article Bacteriophages: Ecology and Applications Ramin Mazaheri Nezhad Fard 1,2* 1. Department of Pathobiology, School of Public Health, Tehran University of Medical Sciences, Tehran, Iran 2. Food Microbiology Research Center, Tehran University of Medical Sciences, Tehran, Iran Table of Contents Bacteriophages: Ecology and Applications………………………………………………....1 Abstract ...................................................................................................................................... 1 Introduction ................................................................................................................................ 2 Background ............................................................................................................................ 2 Ecology .................................................................................................................................. 2 Genomics ............................................................................................................................... 6 Collection ............................................................................................................................... 7 Applications ........................................................................................................................... 8 Conclusions ............................................................................................................................. -

Evaluation of Methods for the Concentration and Extraction of Viruses from Sewage in the Context of Metagenomic Sequencing
RESEARCH ARTICLE Evaluation of Methods for the Concentration and Extraction of Viruses from Sewage in the Context of Metagenomic Sequencing Mathis Hjort Hjelmsø1☯*, Maria HellmeÂr2☯, Xavier Fernandez-Cassi3, Natàlia Timoneda3,4, Oksana Lukjancenko1, Michael Seidel5, Dennis ElsaÈsser5, Frank M. Aarestrup1, Charlotta LoÈfstroÈ m2¤, SõÂlvia Bofill-Mas3, Josep F. Abril3,4, Rosina Girones3, Anna Charlotte Schultz2 a1111111111 1 Research Group for Genomic Epidemiology, The National Food Institute, Technical University of Denmark, Kongens Lyngby, Denmark, 2 Division of Microbiology and Production, The National Food Institute, a1111111111 Technical University of Denmark, Søborg, Denmark, 3 Laboratory of Virus Contaminants of Water and Food, a1111111111 Department of Genetics, Microbiology, and Statistics, University of Barcelona, Barcelona, Catalonia, Spain, a1111111111 4 Institute of Biomedicine of the University of Barcelona, University of Barcelona, Barcelona, Catalonia, a1111111111 Spain, 5 Institute of Hydrochemistry, Chair of Analytical Chemistry, Technical University of Munich, Munich, Germany ☯ These authors contributed equally to this work. ¤ Current address: Food and Bioscience, SP Technical Research Institute of Sweden, Lund, Sweden * [email protected] OPEN ACCESS Citation: Hjelmsø MH, HellmeÂr M, Fernandez-Cassi X, Timoneda N, Lukjancenko O, Seidel M, et al. Abstract (2017) Evaluation of Methods for the Concentration and Extraction of Viruses from Viral sewage metagenomics is a novel field of study used for surveillance, epidemiological Sewage in the Context of Metagenomic Sequencing. PLoS ONE 12(1): e0170199. studies, and evaluation of waste water treatment efficiency. In raw sewage human waste doi:10.1371/journal.pone.0170199 is mixed with household, industrial and drainage water, and virus particles are, therefore, Editor: Patrick Tang, Sidra Medical and Research only found in low concentrations. -

Reticulate Evolution Everywhere
Reticulate Evolution Everywhere Nathalie Gontier Abstract Reticulation is a recurring evolutionary pattern found in phylogenetic reconstructions of life. The pattern results from how species interact and evolve by mechanisms and processes including symbiosis; symbiogenesis; lateral gene transfer (that occurs via bacterial conjugation, transformation, transduction, Gene Transfer Agents, or the movements of transposons, retrotransposons, and other mobile genetic elements); hybridization or divergence with gene flow; and infec- tious heredity (induced either directly by bacteria, bacteriophages, viruses, pri- ons, protozoa and fungi, or via vectors that transmit these pathogens). Research on reticulate evolution today takes on inter- and transdisciplinary proportions and is able to unite distinct research fields ranging from microbiology and molecular genetics to evolutionary biology and the biomedical sciences. This chapter sum- marizes the main principles of the diverse reticulate evolutionary mechanisms and situates them into the chapters that make up this volume. Keywords Reticulate evolution · Symbiosis · Symbiogenesis · Lateral Gene Transfer · Infectious agents · Microbiome · Viriome · Virolution · Hybridization · Divergence with gene flow · Evolutionary patterns · Extended Synthesis 1 Reticulate Evolution: Patterns, Processes, Mechanisms According to the Online Etymology Dictionary (http://www.etymonline.com), the word reticulate is an adjective that stems from the Latin words “re¯ticulātus” (having a net-like pattern) and re¯ticulum (little net). When scholars identify the evolution of life as being “reticulated,” they first and foremost refer to a recurring evolutionary pattern. N. Gontier (*) AppEEL—Applied Evolutionary Epistemology Lab, University of Lisbon, Lisbon, Portugal e-mail: [email protected] © Springer International Publishing Switzerland 2015 1 N. Gontier (ed.), Reticulate Evolution, Interdisciplinary Evolution Research 3, DOI 10.1007/978-3-319-16345-1_1 2 N. -

PRIMER Fall 2008 Volume 5 Issue 2
the PRIMER Fall 2008 Volume 5 Issue 2 also in this issue Guts ’R Us?: CSP 2009 JGI News . 2 Genome of Simplest Animal Reveals Ancient User Community Faces: Lineage . 10 Selections Announced Alexandra Worden . 3 Using Metagenomics Super Bacteria for on Lake Washington Q: What do boat-boring the information that we gener- Super Alfalfa . 4 Microbes. 12 bivalves and stinkbirds have ate from these selections CSP2009 Project at in common? JGI Announcements . 16 promise to take us faster and Contaminated A: Their guts are just two of 44 further down the path toward Hanford Site . 6 new CSP 2009 targets. clean, renewable transporta- In the continuing effort to tion fuels while affording us a tap the vast, unexplored reaches more comprehensive under- Director Rubin of the Earth’s microbial and standing of the global carbon plant domains for bioenergy cycle,” says Eddy Rubin, DOE Reviews and environmental applications, JGI Director. “The range of the DOE JGI has announced its projects spans important ter- Genomics of latest portfolio of DNA sequenc- restrial contributors to bio- ing projects for the coming year. mass production in the Loblolly Biofuels in The 44 projects, culled from pine—the cornerstone of the Nature nearly 150 proposals received U.S. forest products industry— through the Community to phytoplankton, barely visible Genomics is accelerating Sequencing Program (CSP), will to the naked eye, but no less improvements for converting collectively generate more than important to the massive gen- plant biomass into biofuel, thus 60 billion nucleotides of data. eration of fixed carbon in our bringing closer to reality wide- “The scientific and techno- marine ecosystems.” spread use of an alternative to logical advances enabled by With new cont. -

FY 2013 Trans-NIH AIDS Research By-Pass Budget Estimate and Trans
FY 2013 National Institutes of Health TRANS-NIH AIDS RESEARCH BY-PASS BUDGET ESTIMATE and TRANS-NIH PLAN FOR HIV-RELATED RESEARCH Prepared by the Office of AIDS Research Jack Whitescarver, Ph.D. NIH Associate Director for AIDS Research and Director, Office of AIDS Research The cover photo shows a 3-D model of HIV, depicted as orange threads, attacking and fusing with an immune cell, depicted as the gray surface. Constructed by a Russian team of scientists, the image won first place for illustrations in the 2010 International Science and Engineering Visualization Challenge sponsored by the journal Science and the National Science Foundation. ©Visual Science Company www.visualsciencecompany.com F Y 2013 National Institutes of Health TRANS-NIH AIDS RESEARCH BY-PASS BUDGET ESTIMATE and TRANS-NIH PLAN FOR HIV-RELATED RESEARCH Dr. Edward Handelsman at the Liquid Camp for HIV-positive teens, where he served each summer as the camp’s Medical Director. Dedicated to the memory and legacy of DR. EDWARD LOUIS HANDELSMAN Chief of the International Maternal, Adolescent, and Pediatric Branch Division of AIDS National Institute of Allergy and Infectious Diseases National Institutes of Health His intelligence, passion, commitment, and heart made him a champion for maternal, pediatric, and adolescent AIDS research, prevention, and care. FY 2013 Trans-NIH AIDS Research By-Pass Research AIDS Trans-NIH FY 2013 FY 2013 Trans-NIH AIDS Research By-Pass Budget Estimate CONTENTS 1 Legislative Mandate 3 Introduction 7 HIV/AIDS Pandemic 11 NIH AIDS Research Program -
25.9 Metagenomics NV Q&A MH IF
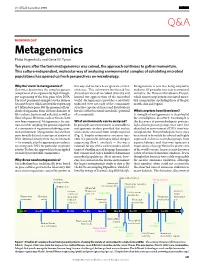
Vol 455|25 September 2008 Q&A MICROBIOLOGY Metagenomics Philip Hugenholtz and Gene W. Tyson Ten years after the term metagenomics was coined, the approach continues to gather momentum. This culture-independent, molecular way of analysing environmental samples of cohabiting microbial populations has opened up fresh perspectives on microbiology. Why the ‘meta’ in metagenomics? this way and we have been ignorant of their Meta genomics is now also being adopted in Genomics determines the complete genetic existence. This cultivation bottleneck has medicine. Of particular note is an international complement of an organism by high-through- skewed our view of microbial diversity and initiative, the Human Microbiome Project, put sequencing of the base pairs of its DNA. limited our appreciation of the microbial which aims to map human-associated micro- The most prominent example was the Human world. Meta genomics provides a relatively bial communities (including those of the gut, Genome Project, which involved the sequencing unbiased view not only of the community mouth, skin and vagina). of 3 billion base pairs. But the genomes of hun- structure (species richness and distribution) dreds of organisms from all three domains of but also of the functional (metabolic) potential What surprises have there been? life (archaea, bacteria and eukarya), as well as of a community. A strength of metagenomics is its potential those of quasi-life forms such as viruses, have for serendipitous discovery. An example is now been sequenced. Metagenomics, by con- What environments can be analysed? the discovery of proteorhodopsin proteins, trast, involves sampling the genome sequences In principle, any environment is amenable to light-driven proton pumps that were first of a community of organisms inhabiting a com- metagenomic analysis provided that nucleic identified in environmental DNA from bac- mon environment. -

The Bi-Directional Relationship Between Gut Microbiota and Autoimmunity Trevor O
Eastern Washington University EWU Digital Commons EWU Masters Thesis Collection Student Research and Creative Works Spring 2018 The bi-directional relationship between gut microbiota and autoimmunity Trevor O. Kirby Eastern Washington University Follow this and additional works at: http://dc.ewu.edu/theses Part of the Microbial Physiology Commons, and the Organismal Biological Physiology Commons Recommended Citation Kirby, Trevor O., "The bi-directional relationship between gut microbiota and autoimmunity" (2018). EWU Masters Thesis Collection. 507. http://dc.ewu.edu/theses/507 This Thesis is brought to you for free and open access by the Student Research and Creative Works at EWU Digital Commons. It has been accepted for inclusion in EWU Masters Thesis Collection by an authorized administrator of EWU Digital Commons. For more information, please contact [email protected]. The Bi-directional Relationship Between Gut Microbiota and Autoimmunity ________________________________________________________________________ A Thesis Presented To Eastern Washington University Cheney, Washington In Partial Fulfillment of the Requirements For the Degree Masters of Science in Biology ________________________________________________________________________ By Trevor O. Kirby Spring 2018 THESIS OF TREVOR O. KIRBY APPROVED BY ______________________________________________________DATE____________ DR. JAVIER OCHOA-REPÁRAZ, CHAIR, GRADUATE STUDY COMMITTEE ______________________________________________________DATE____________ DR. ANDREA CASTILLO, GRADUATE STUDY -

FY 2015 Trans-NIH Plan for HIV-Related Research
FY 2015 National Institutes of Health TRANS-NIH PLAN FOR HIV-RELATED RESEARCH Prepared by the Office of AIDS Research Jack Whitescarver, Ph.D. NIH Associate Director for AIDS Research and Director, Office of AIDS Research Dedicated to the Memory of SPENCER COX 1968–2012 An AIDS pioneer, treatment activist, research advocate, and friend. Spencer brought a unique energy and commitment to help us build an AIDS research program that is responsive to the epidemic, based on the most promising science, and inclusive of the voices of the community. He advocated for the highest possible scientific standards for clinical trials to provide clear and useful information for the trial participants and for HIV-infected individuals who may benefit from the research in the future. His voice will be missed. FY 2015 Trans-NIH Plan for HIV-Related Research CONTENTS 1 Legislative Mandate INTRODUCTION 3 Overview 4 HIV/AIDS Pandemic 5 NIH AIDS Research Program 10 NIH Office of AIDS Research 11 Trans-NIH Strategic Plan 12 OAR Budget Development Process 13 Extraordinary Opportunities for FY 2015 19 Conclusion PRIORITY: Expanding Basic Discovery Research 21 Etiology and Pathogenesis PRIORITY: Reducing New Infections 30 Vaccines 45 Microbicides 52 Behavioral and Social Science 64 Treatment as Prevention PRIORITY: Improving Disease Outcomes for HIV-Infected Individuals 70 Drug Discovery, Development, and Treatment 87 Research Toward a Cure PRIORITY: Reducing HIV-Related Disparities 97 Racial and Ethnic Populations 105 Women and Girls 113 Research in International -

Editorial: Tissue Remodeling in Health and Disease Caused by Bacteria, Parasites, Fungi, and Viruses
EDITORIAL published: 02 February 2021 doi: 10.3389/fcimb.2021.642311 Editorial: Tissue Remodeling in Health and Disease Caused by Bacteria, Parasites, Fungi, and Viruses Sigrun Lange 1* and Marcel I. Ramirez 2,3 1 Tissue Architecture and Regeneration Research Group, School of Life Sciences, University of Westminster, London, United Kingdom, 2 Instituto Oswaldo Cruz, Rio de Janeiro, Brazil, 3 Departamento de Bioqu´ımica e Biologia Molecular, Universidade Federal do Parana´ , Curitiba, Brazil Keywords: tissue remodeling, host manipulation, parasites, bacteria, fungi, viruses, zoonosis, host- pathogen interaction Editorial on the Research Topic Tissue Remodeling in Health and Disease Caused by Bacteria, Parasites, Fungi, and Viruses INTRODUCTION Tissues undergo constant remodeling to maintain architecture during growth, in normal physiology and in response to disease. Interactions of the host with both commensals and pathogens, which Edited and reviewed by: include bacteria, viruses, fungi, and parasites, may affect not only immune responses due to Jeroen P. J. Saeij, recognition of pathogen associated molecular patterns (PAMPS), but also tissue remodeling University of California, Davis, including for example through the generation of neo-epitopes and damage-associated molecular United States patterns (DAMPS). Roles for the microbiome, viriome, fungi, as well as pathogenic bacteria and *Correspondence: parasites, in both homeostasis and in host-pathogen interactions, is a topic of considerable interest Sigrun Lange regarding effects relating -

The Potential Benefit and Challenges of Phage Therapy for the Livestock
antibiotics Review Phages for Africa: The Potential Benefit and Challenges of Phage Therapy for the Livestock Sector in Sub-Saharan Africa Angela Makumi * , Amos Lucky Mhone, Josiah Odaba, Linda Guantai and Nicholas Svitek * Department of Animal and Human Health, International Livestock Research Institute (ILRI), P.O. Box 30709, Nairobi 00100, Kenya; [email protected] (A.L.M.); [email protected] (J.O.); [email protected] (L.G.) * Correspondence: [email protected] (A.M.); [email protected] (N.S.) Abstract: One of the world’s fastest-growing human populations is in Sub-Saharan Africa (SSA), accounting for more than 950 million people, which is approximately 13% of the global population. Livestock farming is vital to SSA as a source of food supply, employment, and income. With this population increase, meeting this demand and the choice for a greater income and dietary options come at a cost and lead to the spread of zoonotic diseases to humans. To control these diseases, farmers have opted to rely heavily on antibiotics more often to prevent disease than for treatment. The constant use of antibiotics causes a selective pressure to build resistant bacteria resulting in the emergence and spread of multi-drug resistant (MDR) organisms in the environment. This necessitates the use of alternatives such as bacteriophages in curbing zoonotic pathogens. This review covers the underlying problems of antibiotic use and resistance associated with livestock farming in SSA, bacteriophages as a suitable alternative, what attributes contribute to making bacteriophages potentially valuable for SSA and recent research on bacteriophages in Africa. -

Viral and Bacterial Interactions in the Upper Respiratory Tract
Review Viral and Bacterial Interactions in the Upper Respiratory Tract Astrid A. T. M. Bosch, Giske Biesbroek, Krzysztof Trzcinski, Elisabeth A. M. Sanders, Debby Bogaert* Department of Pediatric Immunology and Infectious Diseases, University Medical Center-Wilhelmina Children’s Hospital, Utrecht, The Netherlands complex microbial interplay. In a balanced state, this ecosystem as Abstract: Respiratory infectious diseases are mainly a part of the complete human microbiome is assumed to play a caused by viruses or bacteria that often interact with major beneficial role for the human host [5]. However, imbalances one another. Although their presence is a prerequisite for in this respiratory microbial community can contribute to subsequent infections, viruses and bacteria may be acquisition of a new bacterial or viral pathogen, carriage of present in the nasopharynx without causing any respira- multiple potential pathogenic bacteria, or a viral co-infection [6]. tory symptoms. The upper respiratory tract hosts a vast Subsequently, imbalances in the ecosystem may result in range of commensals and potential pathogenic bacteria, overgrowth and invasion by bacterial pathogens, causing respira- which form a complex microbial community. This tory or invasive diseases, especially in children with an immature community is assumed to be constantly subject to synergistic and competitive interspecies interactions. immune system. Disturbances in the equilibrium, for instance due to the The focus of this review is to describe current knowledge on acquisition of new bacteria or viruses, may lead to microbial interactions between commonly detected bacterial and overgrowth and invasion. A better understanding of the viral pathogens in the upper respiratory tract, with a focus on the dynamics between commensals and pathogens in the mechanisms by which these interactions are potentially mediated. -

Metagenomics Philip Hugenholtz and Gene W
Vol 455|25 September 2008 Q&A MICROBIOLOGY Metagenomics Philip Hugenholtz and Gene W. Tyson Ten years after the term metagenomics was coined, the approach continues to gather momentum. This culture-independent, molecular way of analysing environmental samples of cohabiting microbial populations has opened up fresh perspectives on microbiology. Why the ‘meta’ in metagenomics? this way and we have been ignorant of their Meta genomics is now also being adopted in Genomics determines the complete genetic existence. This cultivation bottleneck has medicine. Of particular note is an international complement of an organism by high-through- skewed our view of microbial diversity and initiative, the Human Microbiome Project, put sequencing of the base pairs of its DNA. limited our appreciation of the microbial which aims to map human-associated micro- The most prominent example was the Human world. Meta genomics provides a relatively bial communities (including those of the gut, Genome Project, which involved the sequencing unbiased view not only of the community mouth, skin and vagina). of 3 billion base pairs. But the genomes of hun- structure (species richness and distribution) dreds of organisms from all three domains of but also of the functional (metabolic) potential What surprises have there been? life (archaea, bacteria and eukarya), as well as of a community. A strength of metagenomics is its potential those of quasi-life forms such as viruses, have for serendipitous discovery. An example is now been sequenced. Metagenomics, by con- What environments can be analysed? the discovery of proteorhodopsin proteins, trast, involves sampling the genome sequences In principle, any environment is amenable to light-driven proton pumps that were first of a community of organisms inhabiting a com- metagenomic analysis provided that nucleic identified in environmental DNA from bac- mon environment.