Weekly Chemotherapy with Cisplatin and Paclitaxel in Inoperable Non-Small Cell Lung Cancer: an Extended Phase II Study*
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

PI3K Inhibitors in Cancer: Clinical Implications and Adverse Effects
International Journal of Molecular Sciences Review PI3K Inhibitors in Cancer: Clinical Implications and Adverse Effects Rosalin Mishra , Hima Patel, Samar Alanazi , Mary Kate Kilroy and Joan T. Garrett * Department of Pharmaceutical Sciences, College of Pharmacy, University of Cincinnati, Cincinnati, OH 45267-0514, USA; [email protected] (R.M.); [email protected] (H.P.); [email protected] (S.A.); [email protected] (M.K.K.) * Correspondence: [email protected]; Tel.: +1-513-558-0741; Fax: +1-513-558-4372 Abstract: The phospatidylinositol-3 kinase (PI3K) pathway is a crucial intracellular signaling pathway which is mutated or amplified in a wide variety of cancers including breast, gastric, ovarian, colorectal, prostate, glioblastoma and endometrial cancers. PI3K signaling plays an important role in cancer cell survival, angiogenesis and metastasis, making it a promising therapeutic target. There are several ongoing and completed clinical trials involving PI3K inhibitors (pan, isoform-specific and dual PI3K/mTOR) with the goal to find efficient PI3K inhibitors that could overcome resistance to current therapies. This review focuses on the current landscape of various PI3K inhibitors either as monotherapy or in combination therapies and the treatment outcomes involved in various phases of clinical trials in different cancer types. There is a discussion of the drug-related toxicities, challenges associated with these PI3K inhibitors and the adverse events leading to treatment failure. In addition, novel PI3K drugs that have potential to be translated in the clinic are highlighted. Keywords: cancer; PIK3CA; resistance; PI3K inhibitors Citation: Mishra, R.; Patel, H.; Alanazi, S.; Kilroy, M.K.; Garrett, J.T. -

Induction with Mitomycin C, Doxorubicin, Cisplatin And
British Journal of Cancer (1999) 80(12), 1962–1967 © 1999 Cancer Research Campaign Article no. bjoc.1999.0627 Induction with mitomycin C, doxorubicin, cisplatin and maintenance with weekly 5-fluorouracil, leucovorin for treatment of metastatic nasopharyngeal carcinoma: a phase II study RL Hong1, TS Sheen2, JY Ko2, MM Hsu2, CC Wang1 and LL Ting3 Departments of 1Oncology, 2Otolaryngology and 3Radiation Therapy, National Taiwan University Hospital, National Taiwan University, No. 7, Chung-Shan South Road, Taipei 10016, Taiwan Summary The combination of cisplatin and 5-fluorouracil (5-FU) (PF) is the most popular regimen for treating metastatic nasopharyngeal carcinoma (NPC) but it is limited by severe stomatitis and chronic cisplatin-related toxicity. A novel approach including induction with mitomycin C, doxorubicin and cisplatin (MAP) and subsequent maintenance with weekly 5-FU and leucovorin (FL) were designed with an aim to reduce acute and chronic toxicity of PF. Thirty-two patients of NPC with measurable metastatic lesions in the liver or lung were entered into this phase II trial. Mitomycin C 8 mg m–2, doxorubicin 40 mg m–2 and cisplatin 60 mg m–2 were given on day 1 every 3 weeks as initial induction. After either four courses or remission was achieved, patients received weekly dose of 5-FU 450 mg m–2 and leucovorin 30 mg m–2 for maintenance until disease progression. With 105 courses of MAP given, 5% were accompanied by grade 3 and 0% were accompanied by grade 4 stomatitis. The dose-limiting toxicity of MAP was myelosuppression. Forty per cent of courses had grade 3 and 13% of courses had grade 4 leukopenia. -

THE STRUCTURED STORAGE of ONCOLOGICAL CHEMOTERAPEUTIC REGIMENS Contribution to Standardization of Therapeutic Procedures in Current Oncology
THE STRUCTURED STORAGE OF ONCOLOGICAL CHEMOTERAPEUTIC REGIMENS Contribution to Standardization of Therapeutic Procedures in Current Oncology D. Klimes1, L. Dusek1, M. Kubasek1, J. Novotny2, J. Finek3 and R. Vyzula4 1 Institute of Biostatistics and Analyzes, Masaryk University, Kamenice 126/3, Brno, Czech Republik 2 Department of Oncology, General Teaching Hospital, Prague, Czech Republic 3 Charles University Prague, Medical Faculty Pilsen, Pilsen, Czech Republic 4 Masaryk Memorial Cancer Institute, Brno, Czech Republic Keywords: Cancer Chemotherapy Protocols, Antineoplastic Combined Chemotherapy Regimens, XML, Clinical Database. Abstract: The aim of the chemotherapeutic regimens (CHR) digitalization project is the proposal of a universal structure and creation of a publicly accessible database of contemporary CHR as a universal utility for the communication and evaluation of contemporary and newly defined clinical schedules in anti-tumor chemotherapy. After analysis of contemporary anti tumor CHR a standard XML structure was proposed, which enables the recording of simple CHR from the field of chemotherapy in solid adult tumors, and also has the potential of recording the complex treatment protocols in the field of paediatric oncology. The resulting XML documents were saved on a web server. A publicly accessible CHR database was constructed. There were a total of 130 XML documents with definitions of individual CHR in the first phase. Linked to this data store, three examples of web applications were added to demonstrate the potential uses of this newly created database. 1 INTRODUCTION clinical studies and are published in the oncological journals (Goldberg et al., 2004) (Henderson et al., Chemotherapy, along with surgery and radiotherapy 2003) (Citron et al., 2003) and subsequently in is an irreplaceable part of the clinical treatment of national or international guidelines (NCCN, 2006) oncological illnesses across nearly all diagnoses. -

Arsenic Trioxide Is Highly Cytotoxic to Small Cell Lung Carcinoma Cells
160 Arsenic trioxide is highly cytotoxic to small cell lung carcinoma cells 1 1 Helen M. Pettersson, Alexander Pietras, effect of As2O3 on SCLC growth, as suggested by an Matilda Munksgaard Persson,1 Jenny Karlsson,1 increase in neuroendocrine markers in cultured cells. [Mol Leif Johansson,2 Maria C. Shoshan,3 Cancer Ther 2009;8(1):160–70] and Sven Pa˚hlman1 1Center for Molecular Pathology, CREATE Health and 2Division of Introduction Pathology, Department of Laboratory Medicine, Lund University, 3 Lung cancer is the most frequent cause of cancer deaths University Hospital MAS, Malmo¨, Sweden; and Department of f Oncology-Pathology, Cancer Center Karolinska, Karolinska worldwide and results in 1 million deaths each year (1). Institute and Hospital, Stockholm, Sweden Despite novel treatment strategies, the 5-year survival rate of lung cancer patients is only f15%. Small cell lung carcinoma (SCLC) accounts for 15% to 20% of all lung Abstract cancers diagnosed and is a very aggressive malignancy Small cell lung carcinoma (SCLC) is an extremely with early metastatic spread (2). Despite an initially high aggressive form of cancer and current treatment protocols rate of response to chemotherapy, which currently com- are insufficient. SCLC have neuroendocrine characteristics bines a platinum-based drug with another cytotoxic drug and show phenotypical similarities to the childhood tumor (3, 4), relapses occur in the absolute majority of SCLC neuroblastoma. As multidrug-resistant neuroblastoma patients. At relapse, the efficacy of further chemotherapy is cells are highly sensitive to arsenic trioxide (As2O3) poor and the need for alternative treatments is obvious. in vitro and in vivo, we here studied the cytotoxic effects Arsenic-containing compounds have been used in tradi- of As2O3 on SCLC cells. -

A Phase II Trial of the Src-Kinase Inhibitor AZD0530 in Patients with Advanced Castration-Resistant Prostate Cancer: a California Cancer Consortium Study Primo N
Clinical report 179 A phase II trial of the Src-kinase inhibitor AZD0530 in patients with advanced castration-resistant prostate cancer: a California Cancer Consortium study Primo N. Lara Jra,b, Jeff Longmatec, Christopher P. Evansa, David I. Quinnd, Przemyslaw Twardowskic, Gurkamal Chattae, Edwin Posadasf, Walter Stadlerf and David R. Gandaraa Prostate cancer cells undergo neuroendocrine AZD0530, a potent oral Src kinase inhibitor, is feasible differentiation during androgen deprivation and secrete and tolerable in this pretreated patient population neuropeptides, hence activating androgen receptor- but possessed little clinical efficacy as monotherapy. regulated genes. Src-family protein kinases are involved in Strong preclinical evidence warrants further neuropeptide-induced prostate cancer growth and investigation of AZD0530 in earlier-stage prostate migration. A phase II trial of AZD0530, an oral Src-family cancer or as combination therapy. Anti-Cancer Drugs kinase inhibitor, in patients with advanced castration 20:179–184 c 2009 Wolters Kluwer Health | Lippincott resistant prostate cancer was conducted. The primary Williams & Wilkins. endpoint was prostate cancer-specific antigen (PSA) response rate, defined as a 30% or greater decrease. Anti-Cancer Drugs 2009, 20:179–184 A two-stage Simon design was used. Eligibility criteria Keywords: castration-resistant, prostate cancer, Src inhibitor included documentation of castration resistance (including antiandrogen withdrawal), adequate end-organ aUniversity of California Davis Cancer Center, Sacramento, bVeterans’ function, and performance status, and not more than one Administration of Northern California, Mather, cCity of Hope Comprehensive Cancer Center, Duarte, dUniversity of Southern California Norris Cancer Center, prior taxane-based chemotherapy regimen. AZD0530 was Los Angeles, California, eUniversity of Pittsburgh Cancer Center, Pittsburgh, given at 175 mg orally once daily continuously. -

Is Combined Chemotherapy with Cisplatin, Etoposide and Irinotecan the New Standard Treatment for Patients with Sensitive Relapsed Small Cell Lung Cancer?
Editorial Is combined chemotherapy with cisplatin, etoposide and irinotecan the new standard treatment for patients with sensitive relapsed small cell lung cancer? Alessandro Morabito Oncologia Medica Toraco-Polmonare, IRCCS Istituto Nazionale dei Tumori, Fondazione Pascale, Napoli, Italy Correspondence to: Alessandro Morabito, MD. Director of Thoracic Medical Oncology, National Cancer Institute, Via Mariano Semola, 80131 Naples, Italy. Email: [email protected]; [email protected]. Comment on: Goto K, Ohe Y, Shibata T, et al. Combined chemotherapy with cisplatin, etoposide, and irinotecan versus topotecan alone as second-line treatment for patients with sensitive relapsed small-cell lung cancer (JCOG0605): a multicentre, open-label, randomised phase 3 trial. Lancet Oncol 2016;17:1147-57. Submitted Nov 20, 2016. Accepted for publication Dec 01, 2016. doi: 10.21037/tcr.2016.12.37 View this article at: http://dx.doi.org/10.21037/tcr.2016.12.37 Treatment of small cell lung cancer (SCLC) remains a best supportive care (BSC), combined chemotherapy with significant challenge for the oncologists. Attempts to cyclophosphamide, doxorubicin and vincristine (CAV), improve the results of first- and second-line treatment oral topotecan and amrubicin: topotecan improved OS have all failed so far and no real progress has been made and quality of life compared with BSC, while CAV and in last years, emphasizing the need for novel strategies amrubicin did not show any survival benefit compared with of treatment. Patients with relapsed SCLC are usually topotecan (6-9). Although the efficacy of topotecan was low, classified into different categories, according to the time with response rates from 7% to 24% and OS from 5.8 to elapsed from the end of previous treatment: sensitive, if 9.9 months, no regimen showed superiority over topotecan tumor progression is documented at least 3 months after that continues to be considered as the standard second-line the completion of initial treatment, or resistant if tumor chemotherapy for patients with relapsed SCLC. -

Combination of Oxoplatin with Other FDA-Approved Oncology Drugs
International Journal of Molecular Sciences Article Theoretical Prediction of Dual-Potency Anti-Tumor Agents: Combination of Oxoplatin with Other FDA-Approved Oncology Drugs José Pedro Cerón-Carrasco Reconocimiento y Encapsulación Molecular, Universidad Católica San Antonio de Murcia Campus los Jerónimos, 30107 Murcia, Spain; [email protected] Received: 16 April 2020; Accepted: 2 July 2020; Published: 3 July 2020 Abstract: Although Pt(II)-based drugs are widely used to treat cancer, very few molecules have been approved for routine use in chemotherapy due to their side-effects on healthy tissues. A new approach to reducing the toxicity of these drugs is generating a prodrug by increasing the oxidation state of the metallic center to Pt(IV), a less reactive form that is only activated once it enters a cell. We used theoretical tools to combine the parent Pt(IV) prodrug, oxoplatin, with the most recent FDA-approved anti-cancer drug set published by the National Institute of Health (NIH). The only prerequisite imposed for the latter was the presence of one carboxylic group in the structure, a chemical feature that ensures a link to the coordination sphere via a simple esterification procedure. Our calculations led to a series of bifunctional prodrugs ranked according to their relative stabilities and activation profiles. Of all the designed molecules, the combination of oxoplatin with aminolevulinic acid as the bioactive ligand emerged as the most promising strategy by which to design enhanced dual-potency oncology drugs. Keywords: cancer; drug design; organometallics; platinum-based drugs; bifunctional compounds; theoretical tools 1. Introduction The unexpected discovery of the bioactivity of Pt salts by Rosenberg about 60 years ago opened the door to a new type of cancer treatment: chemotherapy with transition metals [1]. -

Taxotere (Docetaxel) Label
Patient Information Leaflet Detach and give to Patient Rev.May 2004 Patient Information Leaflet Questions and Answers About Taxotere® Injection Concentrate (generic name = docetaxel) (pronounced as TAX-O-TEER) What is Taxotere? Taxotere is a medication to treat breast cancer, non-small cell lung cancer and prostate cancer. It has severe side effects in some patients. This leaflet is designed to help you understand how to use Taxotere and avoid its side effects to the fullest extent possible. The more you understand your treatment, the better you will be able to participate in your care. If you have questions or concerns, be sure to ask your doctor or nurse. They are always your best source of information about your condition and treatment. What is the most important information about Taxotere? • Since this drug, like many other cancer drugs, affects your blood cells, your doctor will ask for routine blood tests. These will include regular checks of your white blood cell counts. People with low blood counts can develop life-threatening infections. The earliest sign of infection may be fever, so if you experience a fever, tell your doctor right away. • Occasionally, serious allergic reactions have occurred with this medicine. If you have any allergies, tell your doctor before receiving this medicine. • A small number of people who take Taxotere have severe fluid retention, which can be life- threatening. To help avoid this problem, you must take another medication such as dexamethasone (DECKS-A-METH-A-SONE) prior to each Taxotere treatment. You must follow the schedule and take the exact dose of dexamethasone prescribed (see schedule at end of brochure). -
Small Cell Lung Cancer (SCLC) Algorithm
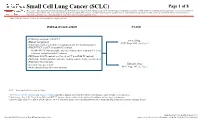
Small Cell Lung Cancer (SCLC) Page 1 of 8 Disclaimer: This algorithm has been developed for MD Anderson using a multidisciplinary approach considering circumstances particular to MD Anderson’s specific patient population, services and structure, and clinical information. This is not intended to replace the independent medical or professional judgment of physicians or other health care providers in the context of individual clinical circumstances to determine a patient's care. This algorithm should not be used to treat pregnant women. Note: Consider Clinical Trials as treatment options for eligible patients. INITIAL EVALUATION STAGE ● Pathology consistent with SCLC Limited Stage ● History and physical AJCC Stage I-III2, see Page 2 ● Laboratory studies to include hematological and full chemistry panels ● FDG PET/CT and CT chest with IV contrast ○ If FDG PET/CT not available: nuclear medicine bone scan and CT chest, abdomen, and pelvis with IV contrast ● MRI brain with IV contrast (preferred) or CT head with IV contrast ● MRI spine, lumbar puncture and bone marrow aspirate/biopsy as indicated ● Pulmonary function tests 1 Extensive Stage ● Lifestyle risk assessment AJCC Stage IV3, see Page 3 ● Molecular profiling (for never smokers) AJCC = American Joint Committee on Cancer 1 See Physical Activity, Nutrition, and Tobacco Cessation algorithms; ongoing reassessment of lifestyle risks should be a part of routine clinical practice 2 Limited stage: Stage I-III (T any, N any, M0) per AJCC 8th edition or disease confined to the ipsilateral hemithorax -

Cisplatin and Etoposide (Lung)
Cisplatin and Etoposide (lung) _____________________________________________________________________________________________ Indication First line chemotherapy for patients with small cell lung cancer (SCLC), who have a good performance status (WHO PS 0-2). Concomitant radiotherapy may start with cycle 2. ICD-10 codes Codes pre-fixed with C34 Regimen details Day Drug Dose Route 1 Cisplatin 75-80mg/m² IV infusion 1 Etoposide 100mg/m² IV infusion 2 and 3 or Etoposide 100mg/m² IV infusion 2 and 3 Etoposide 200mg/m2 PO Cycle frequency 21 days Number of cycles 4 - 6 cycles (usually 4) Administration Cisplatin is administered in 500mL sodium chloride 0.9% over 60 minutes following the pre and post hydration protocol below. Infusion Fluid & Additives Volume Infusion Time Sodium Chloride 0.9% 1000mL 1 hour Mannitol 20% 200mL 30 minutes OR Mannitol 10% 400mL 30 minutes Ensure urine output > 100mL / hour prior to giving cisplatin. Give a single dose of furosemide 20mg iv if necessary. Cisplatin 500mL 1 hour Sodium Chloride 0.9% + 2g MgSO4 + 1000mL 2 hours 20mmol KCl TOTAL 2700mL or 2900mL 4 hours 30 minutes Note: Patients with magnesium or potassium below the normal range should have 2g MgSO4 and 20mmol KCl added to the pre-hydration bag and the duration of the infusion increased to 2 hours. All patients must be advised to drink at least 2 litres of fluid over the following 24 hours. IV etoposide is administered in 1000mL sodium chloride 0.9% and infused over a minimum of 1 hour. Version 1 Review date June 2018 Page 1 of 4 Oral etoposide is available as 50mg and 100mg capsules. -

Advances in Cancer Research Hariharan U*
Editorial iMedPub Journals Archives in Cancer Research 2021 www.imedpub.com Vol.9 ISSN No.S2:e003 Advances in Cancer Research Hariharan U* Anesthesiology & Intensive Care, Dr Ram Manohar Lohia Hospital & ABVIMS-PGIMER, GGSIP University, New Delhi, India *Corresponding author: Uma Hariharan, Anesthesiology & Intensive Care, Dr Ram Manohar Lohia Hospital & PGIMER, New Delhi, India Tel: +91- 9811271093, E-mail: [email protected] Citation: Hariharan U, (2021) Advances in Cancer research. Arch Cancer Res.Vol.9 No.S2: e003. Copyright: © 2021 Hariharan U. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Introduction therapy for cancer in that they are introduced into the blood stream and are therefore in principle able to address cancer at Chemotherapy (often abbreviated to chemo and sometimes any anatomic location in the body. Systemic therapy is often CTX or CTx) is a type of cancer treatment that uses one or more used in conjunction with other modalities that constitute local anti-cancer drugs (chemotherapeutic agents) as part of a therapy (i.e. treatments whose efficacy is confined to the standardized chemotherapy regimen. Chemotherapy may be anatomic area where they are applied) for cancer such as given with a curative intent (which almost always involves radiation therapy, surgery or hyperthermia therapy. combinations of drugs), or it may aim to prolong life or to Traditional chemotherapeutic agents are cytotoxic by means reduce symptoms (palliative chemotherapy). Chemotherapy is of interfering with cell division (mitosis) but cancer cells vary one of the major categories of the medical discipline specifically widely in their susceptibility to these agents. -

Combination Chemotherapy with Estramustine Phosphate, Ifosfamide and Cisplatin for Hormone-Refractory Prostate Cancer
Acta Med. Okayama, 2006 Vol. 60, No. 1, pp. 43ン49 CopyrightⒸ 2006 by Okayama University Medical School. Original Article http ://www.lib.okayama-u.ac.jp/www/acta/ Combination Chemotherapy with Estramustine Phosphate, Ifosfamide and Cisplatin for Hormone-refractory Prostate Cancer Haruki Kakua, Takashi Saikaa*, Tomoyasu Tsushimab, Atsushi Nagaia, Teruhiko Yokoyamaa, Fernando Abarzuaa, Shin Ebaraa, Daisuke Manabea, Yasutomo Nasua, and Hiromi Kumona aDepartment of Urology, Okayama University Graduate School of Medicine, Dentistry and Pharmaceutical Sciences, Okayama 700ン8558, Japan, and bDepartment of Urology, Medival center of Okayama, Okayama 701-1192, Japan We evaluated the effi ciency and toxicity of estramustine phosphate (ECT), ifosfamide (IFM) and cis- platin (CDDP) combination chemotherapy in twenty-one patients with hormone-refractory prostate cancer (HRPC), for which there is currently no eff ective treatment. Patients received a daily dose of 560 mg ECT in combination with 1.2 g/m2 IFM on days 1 to 5 and 70 mg/m2 CDDP on day 1. This combination therapy was given every 3 to 4 weeks. An objective response of more than 50オ reduc- tion in prostate-specifi c antigen was observed in 9 of 18 patients (50オ), and a more than 50オ reduc- tion in bi-dimensionally measurable soft-tissue lesions was observed in 2 of 7 patients (29オ). The median duration of response among the cases showing partial response was 40 weeks, while the median duration of response of overall partial-response plus stable cases was 30 weeks. The median survival duration of all cases was 47 weeks. Toxicity was modest and acceptable. In conclusion, the ECT, IFM and CDDP combination chemotherapy regimen is a viable treatment option for HRPC.