View: the Following Is a List of Programs and Their Functional Areas of Responsibility
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

True North // September 2017
True North // September 2017 cameco in northern saskatchewan Cameco partners with the Red Cross to support Pelican Narrows evacuees (p.2) WINTER Surviving off 2015 Land and Water Fond du Lac Canoe Quest is a Success Far From Home Red Cross and Cameco employees delivered baby strollers to young families from northeastern Saskatchewan while they were evacuated to Prince Albert and Saskatoon during the wildfires earlier this fall. “Once again, Cameco came through to help those Cameco proud to evacuated in northern Saskatchewan,” said Cindy support evacuees Fuchs, Vice-President of the Canadian Red Cross in during fires Saskatchewan. “We are so thankful for Cameco’s support – it makes a world of difference for people forced from their homes.” Wildfires forced more than 2,700 people from the Cree communities of Pelican Narrows and Sandy Bay in late August. The evacuation ban was lifted September 13. During that time evacuees stayed in Prince Albert and Saskatoon with the aid of the Red Cross. Cameco was proud to partner with the organization and provided baby strollers, movie passes and food to make the stay more comfortable. Cameco also contributed $25,000 to the Red Cross’s Red Gala. Proceeds from the gala help support disaster relief. source: Government of Saskatchewan Facebook page page 2 True North // September 2017 Fond du Lac Youth Canoe Quest imparts important traditional skills The participants in the Fond du Lac also visited the basecamp to perform, Toutsaint says the experience made Canoe Quest met with stunning as well as other members who wanted such an impression that the community sunrises for five days at the beginning to cheer the group along. -

La Ronge Integrated Land Use Management Plan Background
La Ronge Integrated Land Use Management Plan Background Document La Ronge Integrated Land Use Management Plan, January 2003 La Ronge Integrated Land Use Management Plan Management Plan La Ronge Integrated Land Use Management Plan, January 2003 BACKGROUND DOCUMENT TABLE OF CONTENTS PAGE# Lists of Tables and Figures................................................................................... ii Chapter 1 - The La Ronge Planning Area........................................................... 1 Chapter 2 - Ecological and Natural Resource Description............................... 4 2.1 Landscape Area Description..................................................... 4 2.1.1 Sisipuk Plain Landscape Area................................... 4 2.1.2 La Ronge Lowland Landscape Area.......................... 4 2.2 Forest Resources..................................................................... 4 2.3 Water Resources..................................................................... 5 2.4 Geology.................................................................................... 5 2.5 Wildlife Resources.................................................................... 6 2.6 Fish Resources......................................................................... 9 Chapter 3 - Existing Resource Uses and Values................................................11 3.1 Timber......................................................................................12 3.2 Non-Timber Forest Products......................................................13 -

Pictographs in Northern Saskatchewan: Vision Quest
PICTOGRAPHS IN NORTHERN SASKATCHEWAN: VISION QUEST AND PAWAKAN A Thesis Submitted to the Faculty of Graduate Studies and Research in Partial Fulfillment of the Requirements for a Degree of Master of Arts in the Department of Anthropology and Archaeology University of Saskatchewan Saskatoon by Katherine A. Lipsett April, 1990 The author claims copyright. Use shall not be made of the material contained herein without proper acknowledgement, as indicated on the following page. The author has agreed that the Library, University of Saskatchewan, may make this thesis freely available for inspection. Moreover, the author has agreed that permission for extensive copying of this thesis for scholarly purposes may be granted by the professor or professors who supervised the thesis work recorded herein or, in their absence, by the Head of the Department or the Dean of the College in which the thesis work was done. It is understood that due recognition will be given to the author of this thesis and to the University of Saskatchewan in any use of the material in this thesis. Copying or publication or any other use of the thesis for financial gain without approval by the University of Saskatchewan and the author's written permission is prohibited. Requests for permission to copy or to make any other use of material in this thesis in whole or part should be addressed to: Head of the Department of Anthropology and Archaeology University of Saskatchewan Saskatoon, Saskatchewan Canada S7N OWO i ABSTRACT Pictographs in northern Saskatchewan have been linked to the vision quest ritual by Rocky Cree informants. -

The Archaeology of Brabant Lake
THE ARCHAEOLOGY OF BRABANT LAKE A Thesis Submitted to the College of Graduate Studies and Research in Partial Fulfilment of the Requirements for the Degree of Master of Arts in the Department of Anthropology and Archaeology University of Saskatchewan Saskatoon By Sandra Pearl Pentney Fall 2002 © Copyright Sandra Pearl Pentney All rights reserved. PERMISSION TO USE PERMISSION TO USE In presenting this thesis in partial fulfilment of the requirements for a Postgraduate degree from the University of Saskatchewan, I agree that the Libraries of this University may make it freely available for inspection. I further agree that permission for copying of this thesis in any manner, in whole or in part, for scholarly purposes may be granted by the professor or professors who supervised my thesis work or, In their absence, by the Head of the Department or the Dean of the College in which my thesis work was done. It is understood that any copying or publication or use of this thesis or parts thereof for financial gain shall not be allowed without my written permission. It is also understood that due recognition shall be given to me and to the University of Saskatchewan in any scholarly use which may be made of any material in my thesis. Requests for permission to copy or to make other use of material in this thesis in whole or part should be addressed to: Head of the Department of Anthropology and Archaeology University of Saskatchewan Saskatoon, Saskatchewan (S7N 5B 1) ABSTRACT Boreal forest archaeology is costly and difficult because of rugged terrain, the remote nature of much of the boreal areas, and the large expanses of muskeg. -

Politics, Power, and Environmental Governance: a Comparative Case Study of Three Métis Communities in Northwest Saskatchewan
University of Alberta Politics, Power, and Environmental Governance: A Comparative Case Study of Three Métis Communities in Northwest Saskatchewan by Bryn Alan Politylo A thesis submitted to the Faculty of Graduate Studies and Research in partial fulfillment of the requirements for the degree of Master of Science in Rural Sociology Department of Resource Economics and Environmental Sociology ©Bryn Alan Politylo Fall 2011 Edmonton, Alberta Permission is hereby granted to the University of Alberta Libraries to reproduce single copies of this thesis and to lend or sell such copies for private, scholarly or scientific research purposes only. Where the thesis is converted to, or otherwise made available in digital form, the University of Alberta will advise potential users of the thesis of these terms. The author reserves all other publication and other rights in association with the copyright in the thesis and, except as herein before provided, neither the thesis nor any substantial portion thereof may be printed or otherwise reproduced in any material form whatsoever without the author's prior written permission. Abstract Recently northwest Saskatchewan has seen a rapid push towards large-scale development corresponding with a shifting political economy in the province. For the rights- bearing Métis people of northwest Saskatchewan this shift significantly influences provincial environmental governance, which affects the agency of Métis people to participate in natural resource management and decision-making in the region. To examine the agency and power of Métis communities in provincial natural resource management and decision-making, qualitative methods and a comparative case study of three Métis communities were used to analyze and interpret the social spaces that Métis people occupy in provincial environmental governance. -
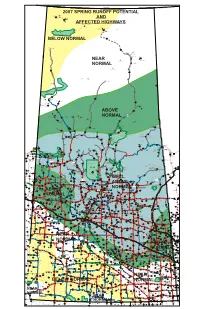
Spring Runoff Highway Map.Pdf
NUNAVUT TERRITORY MANITOBA NORTHWEST TERRITORIES 2007 SPRING RUNOFF POTENTIAL Waterloo Lake (Northernmost Settlement) Camsell Portage .3 999 White Lake Dam AND Uranium City 11 10 962 19 AFFECTEDIR 229 Fond du Lac HIGHWAYS Fond-du-Lac IR 227 Fond du Lac IR 225 IR 228 Fond du Lac Black Lake IR 224 IR 233 Fond du Lac Black Lake Stony Rapids IR 226 Stony Lake Black Lake 905 IR 232 17 IR 231 Fond du Lac Black Lake Fond du Lac ATHABASCA SAND DUNES PROVINCIAL WILDERNESS PARK BELOW NORMAL 905 Cluff Lake Mine 905 Midwest Mine Eagle Point Mine Points North Landing McClean Lake Mine 33 Rabbit Lake Mine IR 220 Hatchet Lake 7 995 3 3 NEAR Wollaston Lake Cigar Lake Mine 52 NORMAL Wollaston Lake Landing 160 McArthur River Mine 955 905 S e m 38 c h u k IR 192G English River Cree Lake Key Lake Mine Descharme Lake 2 Kinoosao T 74 994 r a i l CLEARWATER RIVER PROVINCIAL PARK 85 955 75 IR 222 La Loche 914 La Loche West La Loche Turnor Lake IR 193B 905 10 Birch Narrows 5 Black Point 6 IR 221 33 909 La Loche Southend IR 200 Peter 221 Ballantyne Cree Garson Lake 49 956 4 30 Bear Creek 22 Whitesand Dam IR 193A 102 155 Birch Narrows Brabant Lake IR 223 La Loche ABOVE 60 Landing Michel 20 CANAM IR 192D HIGHWAY Dillon IR 192C IR 194 English River Dipper Lake 110 IR 193 Buffalo English River McLennan Lake 6 Birch Narrows Patuanak NORMAL River Dene Buffalo Narrows Primeau LakeIR 192B St.George's Hill 3 IR 192F English River English River IR 192A English River 11 Elak Dase 102 925 Laonil Lake / Seabee Mine 53 11 33 6 IR 219 Lac la Ronge 92 Missinipe Grandmother’s -

Northern Saskatchewan Administration District (NSAD)
Northern Saskatchewan Administration District (NSAD) Camsell Uranium ´ Portage City Stony Lake Athasbasca Rapids Athabasca Sand Dunes Provincial Park Cluff Lake Points Wollaston North Eagle Point Lake Airport McLean Uranium Mine Lake Cigar Lake Uranium Rabbit Lake Wollaston Mine Uranium Mine Lake McArthur River 955 Cree Lake Key Lake Uranium Reindeer Descharme Mine Lake Lake 905 Clearwater River Provincial Park Turnor 914 La Loche Lake Garson Black Lake Point Bear Creek Southend Michel Village St. Brabant George's Buffalo Hill Patuanak Narrows 102 Seabee 155 Gold Mine Santoy Missinipe Lake Gold Sandy Ile-a-la-crosse Pinehouse Bay Stanley Mission Wadin Little Bay Pelican Amyot Lac La Ronge Jans Bay La Plonge Provincial Park Narrows Cole Bay 165 La Ronge Beauval Air Napatak Keeley Ronge Tyrrell Lake Jan Lake Lake 55 Sturgeon-Weir Creighton Michel 2 Callinan Point 165 Dore Denare Lake Tower Meadow Lake Provincial Park Beach Beach 106 969 916 Ramsey Green Bay Weyakwin East 55 Sled Trout Lake Lake 924 Lake Little 2 Bear Lake 55 Prince Albert Timber National Park Bay Prince Albert Whelan Cumberland Little Bay Narrow Hills " Peck Fishing G X Delaronde National Park Provincial Park House NortLahke rLnak eTowns Northern Hamlets ...Northern Settlements 123 Creighton Black Point Descharme Lake 120 Noble's La Ronge Cole Bay Garson Lake 2 Point Dore Lake Missinipe # Jans Bay Sled Lake Ravendale Northern Villages ! Peat Bog Michel Village Southend ...Resort Subdivisions 55 Air Ronge Patuanak Stanley Mission Michel Point Beaval St. George's Hill Uranium -
Diabetes Directory
Saskatchewan Diabetes Directory February 2015 A Directory of Diabetes Services and Contacts in Saskatchewan This Directory will help health care providers and the general public find diabetes contacts in each health region as well as in First Nations communities. The information in the Directory will be of value to new or long-term Saskatchewan residents who need to find out about diabetes services and resources, or health care providers looking for contact information for a client or for themselves. If you find information in the directory that needs to be corrected or edited, contact: Primary Health Services Branch Phone: (306) 787-0889 Fax : (306) 787-0890 E-mail: [email protected] Acknowledgement The Saskatchewan Ministry of Health acknowledges the efforts/work/contribution of the Saskatoon Health Region staff in compiling the Saskatchewan Diabetes Directory. www.saskatchewan.ca/live/health-and-healthy-living/health-topics-awareness-and- prevention/diseases-and-disorders/diabetes Table of Contents TABLE OF CONTENTS ........................................................................... - 1 - SASKATCHEWAN HEALTH REGIONS MAP ............................................. - 3 - WHAT HEALTH REGION IS YOUR COMMUNITY IN? ................................................................................... - 3 - ATHABASCA HEALTH AUTHORITY ....................................................... - 4 - MAP ............................................................................................................................................... -

Community Investment in the Pandemic: Trends and Opportunities
Community investment in the pandemic: trends and opportunities Jonathan Huntington, Vice President Sustainability and Stakeholder Relations, Cameco January 6, 2021 A Cameco Safety Moment Recommended for the beginning of any meeting Community investment in the pandemic: trends and opportunities (January 6, 2021) 2 Community investment in the pandemic: Trends • Demand - increase in requests • $1 million Cameco COVID Relief Fund: 581 applications, $17.5 million in requests • Immense competition for funding dollars • We supported 67 community projects across 40 different communities in SK Community investment in the pandemic: trends and opportunities (January 6, 2021) 3 Successful applicants for Cameco COVID Relief Fund Organization Community Organization Community Children North Family Resource Center La Ronge The Generation Love Project Saskatoon Prince Albert Child Care Co-operative Association Prince Albert Lakeview Extended School Day Program Inc. Saskatoon Central Urban Metis Federation Inc. Saskatoon Delisle Elementary School -Hampers Delisle TLC Daycare Inc. Birch Hills English River First Nation English River Beauval Group Home (Shirley's Place) Beauval NorthSask Special Needs La Ronge Nipawin Daycare Cooperative Nipawin Leask Community School Leask Battlefords Interval House North Battleford Metis Central Western Region II Prince Albert Beauval Emergency Operations - Incident Command Beauval Global Gathering Place Saskatoon Northern Hamlet of Patuanak Patuanak Saskatoon YMCA Saskatoon Northern Settlement of Uranium City Uranium City -

Bylaw No. 3 – 08
BYLAW NO. 3 – 08 A bylaw of The Urban Municipal Administrators’ Association of Saskatchewan to amend Bylaw No. 1-00 which provides authority for the operation of the Association under the authority of The Urban Municipal Administrators Act. The Association in open meeting at its Annual Convention enacts as follows: 1) Article V. Divisions Section 22 is amended to read as follows: Subsection (a) DIVISION ONE(1) Cities: Estevan, Moose Jaw, Regina and Weyburn Towns: Alameda, Arcola, Assiniboia, Balgonie, Bengough, Bienfait, Broadview, Carlyle, Carnduff, Coronach, Fleming, Francis, Grenfell, Indian Head, Kipling, Lampman, Midale, Milestone, Moosomin, Ogema, Oxbow, Pilot Butte, Qu’Appelle, Radville, Redvers, Rocanville, Rockglen, Rouleau, Sintaluta, Stoughton, Wapella, Wawota, White City, Whitewood, Willow Bunch, Wolseley, Yellow Grass. Villages: Alida, Antler, Avonlea, Belle Plaine, Briercrest, Carievale, Ceylon, Creelman, Drinkwater, Fairlight, Fillmore, Forget, Frobisher, Gainsborough, Gladmar, Glenavon, Glen Ewen, Goodwater, Grand Coulee, Halbrite, Heward, Kendal, Kennedy, Kenosee Lake, Kisbey, Lake Alma, Lang, McLean, McTaggart, Macoun, Manor, Maryfield, Minton, Montmarte, North Portal, Odessa, Osage, Pangman, Pense, Roch Percee, Sedley, South Lake, Storthoaks, Sun Valley, Torquay, Tribune, Vibank, Welwyn, Wilcox, Windthorst. DIVISION TWO(2) Cities: Swift Current Towns: Burstall, Cabri, Eastend, Gravelbourg, Gull Lake, Herbert, Kyle, Lafleche, Leader, Maple Creek, Morse, Mossbank, Ponteix, Shaunavon. Villages: Abbey, Aneroid, Bracken, -

Cameco COVID-19 Relief Fund Supports 67 Community Projects
TSX: CCO website: cameco.com NYSE: CCJ currency: Cdn (unless noted) 2121 – 11th Street West, Saskatoon, Saskatchewan, S7M 1J3 Canada Tel: 306-956-6200 Fax: 306-956-6201 Cameco COVID-19 Relief Fund Supports 67 Community Projects Saskatoon, Saskatchewan, Canada, April 30, 2020 . Cameco (TSX: CCO; NYSE: CCJ) is pleased to announce that the company is supporting 67 community projects in Saskatoon and northern Saskatchewan through its $1 million Cameco COVID-19 Relief Fund. “There are so many communities and charitable groups hit hard by this pandemic, yet their services are needed now more than ever,” said Cameco president and CEO Tim Gitzel. “We are extremely happy to be able to help 67 of these organizations continue to do the vital work they do every day to keep people safe and supported through this unprecedented time.” Approved projects come from 40 Saskatchewan communities from Saskatoon to the province’s far north. A full listing can be found at the end of this release. Included in the support Cameco is providing are significant numbers of personal protective equipment (PPE) for northern Saskatchewan communities and First Nations – 10,000 masks, 7,000 pairs of gloves and 7,000 litres of hand sanitizer. Donations of supplies and money from nearly 100 Cameco employees augmented the company’s initial $1 million contribution. Cameco will move quickly to begin delivering this support to the successful applicants. “I’m proud of Cameco’s employees for stepping up yet again to support the communities where they live,” Gitzel said. “It happens every time we put out a call for help, a call for volunteers, a call to assist with any of our giving campaigns, and I can’t say enough about their generosity.” Announced on April 15, the Cameco COVID-19 Relief Fund was open to applications from charities, not-for-profit organizations, town offices and First Nation band offices in Saskatoon and northern Saskatchewan that have been impacted by the pandemic. -

Download Trip Notes
Canadian Wilderness Trip Notes TRIP OVERVIEW Explore the Canadian wilderness along the Churchill River System in Canada’s Saskatchewan province. You will be taken to unspoilt remote wilderness locations where beautiful clear and relatively warm freshwater swims, some in moving water and others across open lakes, will both challenge and enthral you. Eagles, osprey, beavers, otters, pelicans and even the occasional bear are not an unusual sight. We take you to a place in time when the river was essential to the survival of the local indigenous peoples. Experience the beauty of the boreal forest, visit white sand beaches, mighty river rapids and canoe portages that have been created by hundreds of years of travel. Enjoy breath-taking views of your swims from the air on a scenic transfer flight in the ‘workhorse of the north’ -a float plane -and listen to a talk about how survival in the north is just a way of life. The meals are delicious, the people are amazing, and of course all the swims are incredible. Evenings are spent at the idyllic Thompson’s Resort with optional evening activities such as canoeing, kayaking, hiking, fishing or even take a scenic flight. WHO IS THIS TRIP FOR? This trip is for swimmers who want to experience off-grid adventures in remote, unspoilt locations. This is the perfect place to just switch off and focus on enjoying stunning swims in a gorgeous wilderness setting. While your days will be spent enjoying being out in nature, evenings at Thompson’s Resort will be your opportunity to enjoy all the comforts of home, including online connectivity.