HDAC Agenda 27 November 2018
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
STUDENT LIFE HANDBOOK Your Reference Guide As a New Student at IPU New Zealand
STUDENT LIFE HANDBOOK Your reference guide as a new student at IPU New Zealand IPU EMERGENCY CONTACT NUMBER (STUDENT SUPPORT/SECURITY) 0800 355 050 UPDATED JANUARY 2019 WELCOME TO haere mai! CONTENTS INTRODUCTION Campus Map 2 Academic Calendar 2018 4 President’s Welcome 5 Palmerston North and the Manawatu Area 6 Reception & Student Services 8 Academic Learning Support Centre 9 IT Support 10 CAMPUS FACILITIES Dining Hall 12 Junior Common Room 13 Health Clinic – D Block and Medical Facilities 14 Healthy Lifestyle Habits 16 The Importance of Health Insurance 17 Community Support Services 18 Recreation Centre + KAN (Performing Arts Centre) 20 Library 21 Study Centre, Prayer Room, Computer Lab and Bus Stop 22 Security 24 Hall Life 26 Recycling on Campus 29 IMPORTANT POLICY Enrolment 30 Refund Policy 32 Overdue Accounts & Fee Payment Policy 33 English Language Requirements 35 Student Visa 36 Assessment 37 Campus Rules and Regulations 41 Regulations for Driving & Vehicles 43 RULES, ADVICE & GUIDELINES Personal Safety 44 Health & Safety 46 Harassment & Bullying 47 New Zealand Law – What international students need to know 48 IPU Complaints Process 55 NZQA - International Students - How to make a complaint 56 Emergency and Contact Details 62 IPU NEW ZEALAND CAMPUS MAP CAMPUS MAP HALL 6 ADMINISTRATION VISITOR PARKING AREAS HALL 5 STUDENT SUPPORT CAR PARK SP HEALTH CLINIC GATE 5 DISABLED CAR PARK HALL 3 SC STUDY CENTRE HALL 4 SP STUDENT CAR PARK S SECURITY OFFICE LIBRARY B BUS STOP HALL 7 HALL 9 SMOKING AREA BICYCLE PARK Senior HALL 2 Common Room -

Manawatu -Wanganui
Venue No Venue Name Venue Physical Address 98 FOXTON RETURNED SERVICES ASSOCIATION 1 EASTON STREET,FOXTON, MANAWATU 4814,NEW ZEALAND 136 TAUMARUNUI COSMOPOLITAN CLUB CORNER KATARINA AND MIRIAMA STREETS,TAUMARUNUI CENTRAL, TAUMARUNUI 3920,NEW ZEALAND 192 CASTLECLIFF CLUB INC 4 TENNYSON STREET,CASTLECLIFF, WANGANUI DISTRICT 4501,NEW ZEALAND 222 THE OFFICE 514-516 MAIN STREET EAST, PALMERSTON NORTH CENTRAL, PALMERSTON NORTH 5301 223 WILLOW PARK TAVERN 820 TREMAINE AVENUE, PALMERSTON NORTH CENTRAL, PALMERSTON NORTH 5301 225 THE COBB 522-532 MAIN STREET EAST, PALMERSTON NORTH CENTRAL, PALMERSTON NORTH 5301 261 TAUMARUNUI RSA CLUB 10 MARAE STREET,TAUMARUNUI CENTRAL, TAUMARUNUI 3946,NEW ZEALAND 272 DANNEVIRKE SERVICES AND CITIZENS CLUB 1 PRINCESS STREET, DANNEVIRKE, MANAWATU 5491 293 Ohakune Tavern 66-72 CLYDE STREET,OHAKUNE, MANAWATU 4625,NEW ZEALAND 308 THE EMPIRE HOTEL 8 STAFFORD STREET, FEILDING, MANAWATU 5600 347 WANGANUI EAST CLUB 101 WAKEFIELD STREET, WANGANUI, WANGANUI DISTRICT 4540 356 TARARUA CLUB 15 TARARUA STREET, PAHIATUA, MANAWATU 5470 365 OHAKUNE CLUB 71 GOLDFINCH STREET, OHAKUNE, MANAWATU 5461 389 ALBERT SPORTS BAR 692-700 MAIN STREET EAST, PALMERSTON NORTH CENTRAL, PALMERSTON NORTH 5301 394 STELLAR BAR 2 VICTORIA STREET, WANGANUI, WANGANUI DISTRICT 4540 395 FATBOYZ BAR COBB AND CO CORNER DURHAM AND OXFORD STREETS, LEVIN, MANAWATU 5500 410 ASHHURST MEMORIAL RSA 74 CAMBRIDGE AVENUE,ASHHURST, MANAWATU 4847,NEW ZEALAND 431 ST JOHN'S CLUB 158 GLASGOW STREET,WANGANUI, WANGANUI DISTRICT 4500,NEW ZEALAND 439 LEVIN COSMOPOLITAN CLUB 47-51 -
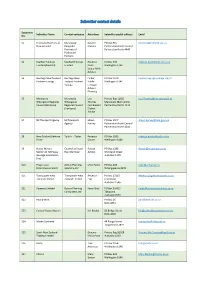
Submitter Contact Details
Submitter contact details Submitter Submitter Name Contact company Attention: Submitter postal address Email No. S1 Federated Farmers of Manawatu- Coralee PO Box 945 [email protected] New Zealand Rangitikei Matena Palmerston North Central Province of Palmerston North 4440 Federated Farmers S2 KiwiRail Holdings KiwiRail Holdings Rebecca PO Box 593 [email protected] Limited (KiwiRail) Limited Beals Wellington 6140 Senior RMA Advisor S3 Heritage New Zealand Heritage New Finbar PO Box 2629 [email protected] Pouhere Taonga Zealand Pouhere Kiddle Wellington 6140 Taonga Heritage Adviser- Planning S5 Manawatu- Manawatu- Lisa Private Bag 11025 [email protected] Whanganui Regional Whanganui Thomas Manawatu Mail Centre Council (Horizons) Regional Council Coordinator Palmerston North 4442 (Horizons) District Advice S7 NZ Transport Agency NZ Transport Shaun PO Box 1947 [email protected] Agency Harvey Palmerston North Central Palmerston North 4440 S8 New Zealand Defence Tonkin + Taylor Rebecca PO Box 2083 [email protected] Force Davies Wellington 6140 S9 House Movers Counsel at Stuart Rowan PO Box 1296 [email protected] Section of NZ Heavy Ryan Barrister Ashton Shortland Street Haulage Association Auckland 1140 (Inc) S10 Progressive Zomac Planning Mike Foster PO Box 103 [email protected] Enterprises Limited Solutions Ltd Whangaparoa 0943 S11 Transpower New Transpower New Rebecca PO Box 17215 [email protected] Zealand Limited Zealand Limited Eng Greenlane Auckland 1546 S21 Powerco -

Historic Places in Palmerston North
Historic Places In Palmerston North An inventory of places listed on the Register of the New Zealand Historic Places Trust Pouhere Taonga Historic Places Manawatu-Horowhenua Incorporated 2013 Historic Places in Palmerston North A project of Historic Places Manawatu-Horowhenua Inc. ISSN: 2357-1861 Prepared by: Rosemary Harris Margaret Tate Pat Scrivens First published in Palmerston North 2007; revised 2013. Design: Ess’Dee Associates Ltd. Copyright: Historic Places Manawatu-Horowhenua Inc. You are free to copy this material for non-commercial use. For all other purposes permission is required from Historic Places Manawatu-Horowhenua Inc., PO Box 732, Palmerston North. Historic Places Manawatu-Horowhenua Inc. revised 2013 1 Contents Introduction ........................................................................................................................................................3 Palmerston North Central Business District Regent Theatre .......................................................................................................................................................5 All Saints' Church (Anglican) ...................................................................................................................................7 Cathedral of the Holy Spirit (Catholic) ....................................................................................................................9 Grand Hotel Building (Former)..............................................................................................................................11 -

3. Palmerston North's Housing Market
1 Contents 1. Overview .................................................................................................................................. 3 2. Annual trends .......................................................................................................................... 3 3. Palmerston North’s housing market ...................................................................................... 4 New residential building consents ........................................................................................... 4 Census housing data ................................................................................................................ 8 Other housing market indicators ........................................................................................... 10 4. Business Activity .................................................................................................................... 14 Non-residential building consents ......................................................................................... 14 5. Outlook for major construction projects in Palmerston North and the wider region ....... 16 6. Retail trends .......................................................................................................................... 16 7. Gross domestic product (GDP) .............................................................................................. 18 8. Employment trends .............................................................................................................. -

Palmerston North
International Safe Community APPLICATION PALMERSTON NORTH FORM A CONTENTS ENDORSEMENT LETTER program have been undertaken and/or supported by the regional government? 46 Mayor of Palmerston North 6 B.4 Describe the strategic program concerning the safety promotion and injury prevention work, which ENDORSEMENT LETTER has been formulated 49 B.5 Who is responsible for the management of the SP/IP Chairperson of the Palmerston program and where are they based in the local political North Safety Advisory Board 7 and administrative organization? 50 B.6 Which is the lead unit for the SP/IP program? 50 SECTION A Community Overview B.7 Is the Safe Communities initiative a sustained program or a project? 50 A.1 Briefly describe the community and its historical development. 9 B.8 Are the objectives decided by the local politicians A.2 Describe the strategy, ambitions, objectives and work in the covering the whole community? Which are they? 52 community in regard to safety. It must be a higher level of safety B.9 Who have adopted these objectives? 53 than average for a community in the country or region. 13 B.10 How are the Safe Community objectives A.3 How is the mayor (or similar function of the community) and the evaluated and executive committee involved? Who is chairing the cross-sector to whom are the results reported? 53 group? 16 B.11 Are economic incentives in order to increase safety A.4 Describe the injury risk-panorama in the community. 17 used? If yes, how are they used? 54 B.12 Are there local regulations for improved safety? SECTION B Structure of the Community If so, describe them 55 B.1 Describe the demographic structure of the community 43 SECTION C Indicator 1 B.2 Describe the SC/IP at present and the plans for the future. -

Youth Directory
YOUTH DIRECTORY The Youth Directory was originally produced by the Youth One Stop Shop (‘YOSS’) in 1995. It is not a complete listing of all the agencies and organisations that work with young people in Palmerston North – but a list of community groups that we use as referral sources. On request from community groups YOSS in co-operation with START, have made this information available and it is important that it is used as a living document, needing amendments and additions. Please feel free to photocopy and hand the Youth Directory on to friends and colleagues. Please contact us with any amendments or additions that can be made in subsequent editions of the Youth Directory. Corner Andrew Young & Cuba Streets PO Box 2074, Palmerston North (06) 355 5143 [email protected] This directory was updated on 23 June 2011. CONTENTS Manawatu Lesbian & Gay Rights Association ......... 10 24 Hour Help .................................5 MASH Trust ....................................................... 10 MUSA Advocacy Service...................................... 10 Alcoholics Anonymous .......................................... 5 Netsafe – The Internet Safety Group.................... 10 Al’Anon ............................................................... 5 NZ Federation of Disability Information Centre’s.... 10 City Doctors ........................................................ 5 No Bully ............................................................ 10 Department of Child Youth and Family Services ...... 5 P.A.C.I.F.I.C.A Inc............................................. -
What Our Local Data Tells Us Contents
Health Equity Data Report 2018 What our local data tells us Contents Executive Summary ........................................................................................................... 6 Key findings .................................................................................................................................................... 6 Our people ................................................................................................................................................. 6 Our health .................................................................................................................................................. 7 Socioeconomic opportunities for good health ...................................................................................... 7 Inequities in key health indicators......................................................................................................... 8 Conclusion ............................................................................................................................................... 11 Introduction ...................................................................................................................... 12 Purpose ......................................................................................................................................................... 12 Methodology ............................................................................................................................................... -

Palmerston North Technical School (Former), PALMERSTON NORTH (List No.1266, Category 2)
New Zealand Heritage List/Rārangi Kōrero – Review Report for a Historic Place Palmerston North Technical School (Former), PALMERSTON NORTH (List No.1266, Category 2) Palmerston North Technical School (Former), Karen Astwood, Heritage New Zealand, 14 Jan 2021 Karen Astwood 4 June 2021 Heritage New Zealand Pouhere Taonga TABLE OF CONTENTS PURPOSE OF REVIEW 3 EXECUTIVE SUMMARY 4 1. IDENTIFICATION 5 1.1. Name of Place 5 1.2. Location Information 5 1.3. Legal Description 6 1.4. Extent of List Entry 6 1.5. Eligibility 6 1.6. Existing Heritage Recognition 6 2. SUPPORTING INFORMATION 7 2.1. Historical Information 7 2.2. Physical Information 18 2.3. Chattels 25 2.4. Sources 25 3. SIGNIFICANCE ASSESSMENT 27 3.1. Section 66 (1) Assessment 27 3.2. Section 66 (3) Assessment 28 4. APPENDICES 30 4.1. Appendix 1: Visual Identification Aids 30 4.2. Appendix 2: Visual Aids to Historical Information 36 4.3. Appendix 3: Visual Aids to Physical Information 38 4.4. Appendix 4: Significance Assessment Information 42 Disclaimer Please note that entry on the New Zealand Heritage List/Rārangi Kōrero identifies only the heritage values of the property concerned, and should not be construed as advice on the state of the property, or as a comment of its soundness or safety, including in regard to earthquake risk, safety in the event of fire, or insanitary conditions. Archaeological sites are protected by the Heritage New Zealand Pouhere Taonga Act 2014, regardless of whether they are entered on the New Zealand Heritage List/Rārangi Kōrero or not. -
Heading Chapter
Palmerston North Urban Bus Service Review Phase Two Report May 2014 Author Kelly Curry Transport Planner May 2014 CONTACT 24hr Freephone 0508 800 800 [email protected] www.horizons.govt.nz Kairanga Cnr Rongotea & Kairanga-Bunnythorpe Rds Palmerston North Levin Palmerston North 11 Bruce Road 11-15 Victoria Avenue SERVICE Marton REGIONAL Cnr Hammond & Hair Sts DEPOTS CENTRES HOUSES Taihape Wanganui Torere Road Taumarunui 181 Guyton Street 34 Maata Street Ohotu Woodville Cnr Vogel (SH2) & Tay Sts POSTAL Horizons Regional Council, Private Bag 11025, Manawatu Mail Centre, Palmerston North 4442 | 06 9522 929 ADDRESS F CONTENTS 1. Introduction 1.1 Purpose of the Review 1.1.1 Be value for money 1.1.2 Promote passenger growth 1.1.3 Be supported by the community 1.2 The Review Process 2. Key Themes Emerging In Phase One 2.1 Coverage of the City 2.2 Frequency 2.3 Structure of the Urban Routes 2.4 Transfers 2.5 Distance to bus stops 2.6 Hours of service 2.7 Weekend Services 2.8 Massey University Services 3. Local Travel Patterns 3.1 2013 Census Data 3.2 The New Zealand Household Travel Survey 3.3 Bus Ticketing System Analysis 3.3.1 Transfers 3.4 Comparisons with other Networks 4. Description of Options Considered 4.1 Assumptions 4.1.1 Bus travel time 4.1.2 Standard bus size 4.1.3 Transfers 4.2 Current Services 4.3 Option One (Status Quo Plus) Table Five: Option One summary 4.4 Option Two (includes Lollipop, Orbiter, Hospital-City-Massey, Massey Shuttle, Ashhurst-Longburn network) 4.4.1 Network operating hours 4.4.2 Frequency Two options for frequency for the lollipop routes have been developed: Table Six: Option Two summary 4.5 Option Three (Grid) 5. -

Palmerston North Children's Profile
Palmerston North Children’s Profile October 2011 DMS #680827 This Palmerston North Children’s Profile is the latest in a series of sector profiles prepared by the Palmerston North City Council. Information here is drawn from a variety of government and non-government sources. The Palmerston North City Council thanks all those agencies who have contributed to this picture of children in the City. Particular thanks are due to Pat Ruiz, who undertook the preliminary research for this profile while working as an Intern with the Palmerston North City Council for the Migrant Internship Programme. For further information please contact Julie Macdonald, Policy Analyst, Palmerston North City Council (email: [email protected]). Published by: Palmerston North City Council Private Bag 11034 Palmerston North Phone: 06 356 8199 Fax: 06 355 4115 www.pncc.govt.nz 2 Table of Contents Executive Summary ..................................................................................................... 4 1. Introduction ........................................................................................................... 6 2. National Context ................................................................................................... 6 3. Demographic information ...................................................................................... 8 4. Social Wellbeing ................................................................................................. 13 5. Health ................................................................................................................ -

Palmerston North-Manawatū Strategic Transport Study
Palmerston North-Manawatu Strategic Transport Study Contract No 2009/18 Phase 2 Report June 2010 PO Box 30 721 Lower Hutt 5040 P: +64 4 569 8497 www.tdg.co.nz New Zealand 10426_1 v2 phase 2 report.doc 10426_1 v2 phase 2 report.doc Table of Contents 1. Purpose...................................................................................................................................1 2. Background.............................................................................................................................2 2.1 Regional Economy ....................................................................................................2 2.2 Current Proposals......................................................................................................2 2.3 Issues for Consideration............................................................................................3 3. Methodology ...........................................................................................................................4 3.1 Road Hierarchy Criteria .............................................................................................4 3.2 Traffic Modelling ........................................................................................................4 3.3 Cost Estimation .........................................................................................................5 3.4 Network Option Development and Evaluation Criteria...............................................5 4. Existing Road and Traffic Conditions