Maternal Mortality in Jigawa Central Senatorial District: Trend and Causes
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Nigeria's Constitution of 1999
PDF generated: 26 Aug 2021, 16:42 constituteproject.org Nigeria's Constitution of 1999 This complete constitution has been generated from excerpts of texts from the repository of the Comparative Constitutions Project, and distributed on constituteproject.org. constituteproject.org PDF generated: 26 Aug 2021, 16:42 Table of contents Preamble . 5 Chapter I: General Provisions . 5 Part I: Federal Republic of Nigeria . 5 Part II: Powers of the Federal Republic of Nigeria . 6 Chapter II: Fundamental Objectives and Directive Principles of State Policy . 13 Chapter III: Citizenship . 17 Chapter IV: Fundamental Rights . 20 Chapter V: The Legislature . 28 Part I: National Assembly . 28 A. Composition and Staff of National Assembly . 28 B. Procedure for Summoning and Dissolution of National Assembly . 29 C. Qualifications for Membership of National Assembly and Right of Attendance . 32 D. Elections to National Assembly . 35 E. Powers and Control over Public Funds . 36 Part II: House of Assembly of a State . 40 A. Composition and Staff of House of Assembly . 40 B. Procedure for Summoning and Dissolution of House of Assembly . 41 C. Qualification for Membership of House of Assembly and Right of Attendance . 43 D. Elections to a House of Assembly . 45 E. Powers and Control over Public Funds . 47 Chapter VI: The Executive . 50 Part I: Federal Executive . 50 A. The President of the Federation . 50 B. Establishment of Certain Federal Executive Bodies . 58 C. Public Revenue . 61 D. The Public Service of the Federation . 63 Part II: State Executive . 65 A. Governor of a State . 65 B. Establishment of Certain State Executive Bodies . -

The Izala Movement in Nigeria Genesis, Fragmentation and Revival
n the basis on solid fieldwork in northern Nigeria including participant observation, 18 Göttingen Series in Ointerviews with Izala, Sufis, and religion experts, and collection of unpublished Social and Cultural Anthropology material related to Izala, three aspects of the development of Izala past and present are analysed: its split, its relationship to Sufis, and its perception of sharīʿa re-implementation. “Field Theory” of Pierre Bourdieu, “Religious Market Theory” of Rodney Start, and “Modes Ramzi Ben Amara of Religiosity Theory” of Harvey Whitehouse are theoretical tools of understanding the religious landscape of northern Nigeria and the dynamics of Islamic movements and groups. The Izala Movement in Nigeria Genesis, Fragmentation and Revival Since October 2015 Ramzi Ben Amara is assistant professor (maître-assistant) at the Faculté des Lettres et des Sciences Humaines, Sousse, Tunisia. Since 2014 he was coordinator of the DAAD-projects “Tunisia in Transition”, “The Maghreb in Transition”, and “Inception of an MA in African Studies”. Furthermore, he is teaching Anthropology and African Studies at the Centre of Anthropology of the same institution. His research interests include in Nigeria The Izala Movement Islam in Africa, Sufism, Reform movements, Religious Activism, and Islamic law. Ramzi Ben Amara Ben Amara Ramzi ISBN: 978-3-86395-460-4 Göttingen University Press Göttingen University Press ISSN: 2199-5346 Ramzi Ben Amara The Izala Movement in Nigeria This work is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License. Published in 2020 by Göttingen University Press as volume 18 in “Göttingen Series in Social and Cultural Anthropology” This series is a continuation of “Göttinger Beiträge zur Ethnologie”. -

Jigawa State Due Process Project Monitoring Bureau Contracts Awarded January to December, 2020 End of Year Report
JIGAWA STATE DUE PROCESS PROJECT MONITORING BUREAU CONTRACTS AWARDED JANUARY TO DECEMBER, 2020 END OF YEAR REPORT COMP. S/N DATE PROJECT CONTRACT NO. CONTRACTOR AMOUNT (N) EXECUTING MINISTRIES PERIOD WORKS Constr. Of 31No. Hand Pump Borehole water supply schemes (2019 First Quarter Constituency Project) LOT-16 at G/Tela Kabo Fulanin Dandabino, G/Musa Shanu Fulanin Tsanfau, Mekekiya Gari, Gidan Haruna Babe, Dungundun Gari, Fulanin Danmodi, Dangoho Gari, Muku Gari, Maigatari Albasu, G.A gaiya Fulanin Dantsakuwa, Karangi Gari, Tsangayar Kirgi, G/Shu'aibu Ajiya Fulanin Kakudi, Dankulli Gari, Lululu, Zangunan Jeke, Gidan Hardo Yahaya,Gidan Dashi, G/ Hardo Amadu Fulanin Kukule, Gidan Alh. Dare, Gidan Hardo Katore Fulanin Dan Marke, Haro Kandir, Fulanin Barawa, Gidan Mati, Gidan Jikan Banki, Fulanin Jarimawa, Tashar Hajja, Fulanin Dukuku, Hardo Murnai, Gidan Bulama Suna and 1 21/01/2020 Fulanin Mailefe in Sule Tankarkar constituency JEC/478/2019/VOL.I/7 H.M Dangara Ltd 22,872,730.00 Min of Water Res 12 weeks 2 30/01/2020 Upgarde of Malam Madori Primary Health Care to General Hospital (Additional work) FGPC/149/2018/VOL.I/12 Sassauchi Multi Trade Invest Ltd 23,257,704.02 Min of Health 6 Month Constr. Of 1 Block of 2 classroom Islamiyya School Each Lot-8 (2019 Second Quarter Constituency Projects) at andaza 3 21/01/2020 Gabas, Zakwaro and Karangi in Kiyawa Constituency JEC/486/2019/VOL.I/14 Alkayawa Multi services 9,438,765.00 Cabinet Office 8 weeks Constr. Of 3No Daily Prayer Mosques ( 2019 Second Quarter Constituency Projects) Lot-35 at Hariyal, madawa Bello 4 14/01/2020 and Sharbi in Kafin Hausa Constituency JEC/380/2019/VOL.I/29 K-Manu Gen Constr Ltd 5,870,869.00 Cabinet Office 8 weeks Constr. -

In Changing Nigerian Society: a Discussion from the Perspective of Ibn Khaldun’S Concept Ofñumran
THE CONTRIBUTION OF UTHMAN BIN FODUYE (D.1817) IN CHANGING NIGERIAN SOCIETY: A DISCUSSION FROM THE PERSPECTIVE OF IBN KHALDUN’S CONCEPT OFÑUMRAN SHUAIBU UMAR GOKARUMalaya of ACADEMY OF ISLAMIC STUDIES UNIVERSITY OF MALAYA KUALA LUMPUR University 2017 THE CONTRIBUTION OF UTHMAN BIN FODUYE (D.1817) IN CHANGING NIGERIAN SOCIETY: A DISCUSSION FROM THE PERSPECTIVE OF IBN KHALDUN’S CONCEPT OF ÑUMRAN SHUAIBU UMAR GOKARU Malaya THESIS SUBMITTED IN FULFILMENTof OF THE REQUIREMENTS FOR THE DEGREE OF DOCTOR OF PHILOSOPHY UniversityACADEMY OF ISLAMIC STUDIES UNIVERSITY OF MALAYA KUALA LUMPUR 2017 UNIVERSITY OF MALAYA ORIGINAL LITERARY WORK DECLARATION Name of Candidate: Shuaibu Umar Gokaru Matric No: IHA140056 Name of Degree: Doctor of Philosophy Title of Project Paper/Research Report/Dissertation/Thesis (“this Work”) THE CONTRIBUTION OF UTHMAN BIN FODUYE (D. 1817) IN CHANGING NIGERIAN SOCIETY: A DISCUSSION FROM THE PERSPECTIVE OF IBN KHALDUN’S CONCEPT OF ÑUMRAN Field of Study: Islamic Civilisation (Religion) I do solemnly and sincerely declare that: (1) I am the sole author/author of this Work; (2) This Work is original; (3) Any use of any work in which copyright exists was done by way of fair dealing and for permitted purposes and any excerpt or extract from, or reference to or reproduction of any copyrightMalaya work has been disclosed expressly and sufficiently and the title of the Work and its authorship have been acknowledged in this Work; (4) I do not have any actual knowledge nor do I ought reasonably to know that the making of this work -
JG 403 In-Depth Capacity Assessment of Csos in Jigawa State
Education Sector Support Programme in Nigeria (ESSPIN) Assignment Report In‐Depth Capacity Assessment of Civil Society Organisations in Jigawa State Report Number JG 403 Sarah Mkeryi Amahson and Iliya Ambi November 2009 www.esspin.org In‐Depth Capacity Assessment of Civil Society Organisations in Jigawa State Report Distribution and Revision Sheet Project Name: Education Sector Support Programme in Nigeria Code: 244333TA02 Report No.: JG 403 Report Title: In‐Depth Capacity Assessment of Civil Society Organisations in Jigawa State Rev No Date of issue Originator Checker Approver Scope of checking 1 April Sarah Amahson Fatima Steve Formatting/ 2010 and Aboki Baines Checking Iliya Ambi Scope of Checking This report has been discussed with the originator and checked in the light of the requirements of the terms of reference. In addition the report has been checked to ensure editorial consistencies. Distribution List Name Position DFID Kathleen Reid Human Development Programme Coordinator, DFID Ian Attfield Education Adviser, DFID Northern Nigeria Office Roseline Onyemachi Education Project Officer, DFID ESSPIN Ron Tuck National Programme Manager Kayode Sanni Deputy Programme Manager Richard Hanson Assistant Programme Manager Steve Baines Technical Team Coordinator Gboyega Ilusanya State Team Leader Lagos Emma Williams State Team Leader Kwara Richard Dalgarno State Team Leader Kano Steve Bradley State Team Leader Kaduna Pius Elumeze State Team Leader Enugu Kalli Kori Deputy State Team Leader Jigawa John Kay Lead Specialist, Education Quality -

Granite Formations and Granite Cavities in Northern Nigeria
8012096-XEOLOXIA N 33.qxd:maquet. 1 7/1/09 19:47 Página 10 Cadernos Lab. Xeolóxico de Laxe Coruña. 2009. Vol. 34, pp. 13 - 26 ISSN: 0213-4497 As citas bibliográficas dentro do texto poránse en maxúscula e a abreviatura para os seguin- tes autores será: "et al.". Os textos enviados serán sometidos á crítica dos Censores Científicos designados pola Revista. Bibliografía: Autores en maxúsculas e as revistas ou textos citados en cursiva. Granite formations and granite cavities in Os autores dos traballos deberán incluir a súa dirección completa, incluído código postal. northern Nigeria Formaciones graníticas y cavidades Separatas graníticas en el Norte de Nigeria Enviaráse a cada autor un PDF co artículo na versión final. Envío de manuscritos SZENTES, G1. - Os traballos originais enviaránse a: (1) Alte Frankfurter Str. 22b, 61118 Bad Vilbel, Germany. E-mail: [email protected] Instituto Universitario de Xeoloxía Recibido: 9/8/2007 Revisado: 10/3/2008 Aceptado: 15/6/2008 Edificio Servicios Centrales de Investigación Campus de Elviña s/n Telephone: (+34) 981 167000 Ext. 2910 Fax: (+34) 981 167172 [email protected] 15071 A Coruña (Spain) incluindo dirección habitual e teléfono. Abstract — Unha vez terminada a impresión, os originais serán devoltos ao seu autor/es, si así o des- exan e expresan. The Author worked as geologist in Northern Nigeria during several years. This study presents — O número máximo de follas que se admitirá por traballo será quince (15) incluindo figu- his experiences concerning the granite formations of the region. The geological base of Northern ras, fotografías, mapas, etc.. Para traballos de maior extensión rógase consultar ao editor Nigeria is the so-called Basement Complex. -

Survey Report for Out-Of-School Children in Jigawa
SURVEY REPORT FOR OUT-OF-SCHOOL CHILDREN IN JIGAWA STATE, NIGERIA CO-ORDINATED BY JIGAWA STATE GOVERNMENT IN COLLABORATION WITH ESSPIN August, 2014 Page | 1 Table of Contents Cover page i Acknowledgements iii Preface iv List of Tables v List of Figures vi Acronyms vii Executive Summary viii Section One: Introduction 1 1.1 Background 1 1.2 Objectives 2 1.3 Framework for Out-of-School Children 2 1.4 Profile of Jigawa State 4 Section Two: Methodology 6 2.1 Survey Planning for Out-of-School Children 6 2.2 Sampling Design 7 2.3 Data Quality and Supervision 7 2.4 Pilot Survey 8 2.5 Process of Data Collection and Analysis 9 Section Three: Results for Out-of-School Children 10 3.1 Number of Households and Population Size 10 3.2 Number of Out-of-School Children 12 3.3 Number of Children Attending Schools 20 3.4 Percentages of Out-of-School Children 24 Section Four: Possible Risk Factors for Out-of-School Children 27 4.1 Reasons for Out-of-School Children 27 4.2 Socio-Economic Relationships with Out-of-School Status 28 Section Five: Conclusion and Recommendations 42 5.1 Conclusion 42 5.2 Suggestions and the way forward 45 5.3 Limitations 46 References 47 Appendix A: Questionnaire 48 Page | 2 Appendix B: Interview Guide 52 Appendix C: Number of Children in the Sampled Household 53 Appendix D: Percentages of Children that Dropout from School 54 Appendix E: Percentages of Children that Never Attended School 55 Appendix F: Percentages of Children Attending Only Islamiyya/Quranic 56 Schools Appendix G: Percentages of Children Attending any Form of School 57 Appendix H: Population Projection (3-18) by Age, Sex and LGA, 2014 58 Appendix I: Sampling Variability and Ranges for OOS Children 59 Page | 3 Acknowledgements Education planning is incomplete without credible statistics on out-of-school children. -

A Study of Violence-Related Deaths in Nafada Local Government Area Of
# Makai DANIEL http://www.ifra-nigeria.org/IMG/pdf/violence-related-deaths-gombe-jigawa-state-nigeria.pdf A Study of Violence-Related Deaths in Nafada Local Government Area of Gombe State and Auyo, Gagarawa, Gumel, Gwiwa, Kaugama and Yankwasi Local Government Areas of Jigawa State (2006-2014) IFRA-Nigeria working papers series, n°46 20/01/2015 The ‘Invisible Violence’ Project Based in the premises of the French Institute for Research in Africa on the campus of the University of Ibadan, Nigeria Watch is a database project that has monitored fatal incidents and human security in Nigeria since 1 June 2006. The database compiles violent deaths on a daily basis, including fatalities resulting from accidents. It relies on a thorough reading of the Nigerian press (15 dailies & weeklies) and reports from human rights organisations. The two main objectives are to identify dangerous areas and assess the evolution of violence in the country. However, violence is not always reported by the media, especially in remote rural areas that are difficult to access. Hence, in the last 8 years, Nigeria Watch has not recorded any report of fatal incidents in some of the 774 Local Government Areas (LGAs) of the Nigerian Federation. There are two possibilities: either these places were very peaceful, or they were not covered by the media. This series of surveys thus investigates ‘invisible’ violence. By 1 November 2014, there were still 23 LGAs with no report of fatal incidents in the Nigeria Watch database: Udung Uko and Urue-Offong/Oruko (Akwa Ibom), Kwaya Kusar (Borno), Nafada (Gombe), Auyo, Gagarawa, Kaugama and Yankwashi (Jigawa), Ingawa and Matazu (Katsina), Sakaba (Kebbi), Bassa, Igalamela- Odolu and Mopa-Muro (Kogi), Toto (Nassarawa), Ifedayo (Osun), Gudu and Gwadabaw (Sokoto), Ussa (Taraba), and Karasuwa, Machina, Nguru and Yunusari (Yobe). -
Jigawa Code: 17 Lga : Auyo Code: 01 Name of Registration Name of Reg
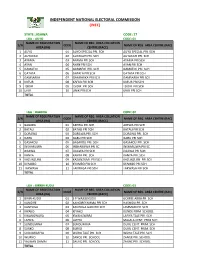
INDEPENDENT NATIONAL ELECTORAL COMMISSION (INEC) STATE: JIGAWA CODE: 17 LGA : AUYO CODE: 01 NAME OF REGISTRATION NAME OF REG. AREA COLLATION S/N CODE NAME OF REG. AREA CENTRE (RAC) AREA (RA) CENTRE (RACC) 1 AUYO 01 AUYO SPECIAL PRI. SCH AUYO SPECIAL PRI. SCH 2 AUYAKAYI 02 AUYAKAYI PRI. SCH AUYAKAYI PRI. SCH 3 AYAMA 03 AYAMA PRI SCH AYAMA PRI SCH 4 AYAN 04 AYAN PRI SCH AYAN PRI SCH 5 GAMAFOI 05 GAMAFOI PRI. SCH GAMAFOI PRI. SCH 6 GATAFA 06 GATAFA PRI SCH GATAFA PRI SCH 7 GAMSARKA 07 GAMSARKA PRI SCH GAMSARKA PRI SCH 8 KAFUR 08 KAFUR PRI SCH KAFUR PRI SCH 9 TSIDIR 09 TSIDIR PRI SCH TSIDIR PRI SCH 10 UNIK 10 UNIK PRI SCH UNIK PRI SCH TOTAL LGA : BABURA CODE: 02 NAME OF REGISTRATION NAME OF REG. AREA COLLATION S/N CODE NAME OF REG. AREA CENTRE (RAC) AREA (RA) CENTRE (RACC) 1 BABURA 01 AREWA PRI.SCH AREWA PRI.SCH 2 BATALI 02 BATALI PRI SCH BATALI PRI SCH 3 DORAWA 03 DORAWA PRI. SCH DORAWA PRI. SCH 4 GARU 04 GARU PRI SCH GARU PRI SCH 5 GASAKOLI 05 GASAKOLI PRI. SCH GASAKOLI PRI. SCH 6 INSHARUWA 06 INSHARUWA PRI SC INSHARUWA PRI SC 7 JIGAWA 07 JIGAWA PRI SCH JIGAWA PRI SCH 8 KANYA 08 KANYA PRI. SCH KANYA PRI. SCH 9 KAZUNZUMI 09 KAZUNZUMI PRI SCH KAZUNZUMI PRI SCH 10 KYAMBO 10 KYAMBO PRI SCH KYAMBO PRI SCH 11 TAKWASA 11 TAKWASA PRI SCH TAKWASA PRI SCH TOTAL LGA : BIRRIN-KUDU CODE: 03 NAME OF REGISTRATION NAME OF REG. -

States and Lcdas Codes.Cdr
PFA CODES 28 UKANEFUN KPK AK 6 CHIBOK CBK BO 8 ETSAKO-EAST AGD ED 20 ONUIMO KWE IM 32 RIMIN-GADO RMG KN KWARA 9 IJEBU-NORTH JGB OG 30 OYO-EAST YYY OY YOBE 1 Stanbic IBTC Pension Managers Limited 0021 29 URU OFFONG ORUKO UFG AK 7 DAMBOA DAM BO 9 ETSAKO-WEST AUC ED 21 ORLU RLU IM 33 ROGO RGG KN S/N LGA NAME LGA STATE 10 IJEBU-NORTH-EAST JNE OG 31 SAKI-EAST GMD OY S/N LGA NAME LGA STATE 2 Premium Pension Limited 0022 30 URUAN DUU AK 8 DIKWA DKW BO 10 IGUEBEN GUE ED 22 ORSU AWT IM 34 SHANONO SNN KN CODE CODE 11 IJEBU-ODE JBD OG 32 SAKI-WEST SHK OY CODE CODE 3 Leadway Pensure PFA Limited 0023 31 UYO UYY AK 9 GUBIO GUB BO 11 IKPOBA-OKHA DGE ED 23 ORU-EAST MMA IM 35 SUMAILA SML KN 1 ASA AFN KW 12 IKENNE KNN OG 33 SURULERE RSD OY 1 BADE GSH YB 4 Sigma Pensions Limited 0024 10 GUZAMALA GZM BO 12 OREDO BEN ED 24 ORU-WEST NGB IM 36 TAKAI TAK KN 2 BARUTEN KSB KW 13 IMEKO-AFON MEK OG 2 BOSARI DPH YB 5 Pensions Alliance Limited 0025 ANAMBRA 11 GWOZA GZA BO 13 ORHIONMWON ABD ED 25 OWERRI-MUNICIPAL WER IM 37 TARAUNI TRN KN 3 EDU LAF KW 14 IPOKIA PKA OG PLATEAU 3 DAMATURU DTR YB 6 ARM Pension Managers Limited 0026 S/N LGA NAME LGA STATE 12 HAWUL HWL BO 14 OVIA-NORTH-EAST AKA ED 26 26 OWERRI-NORTH RRT IM 38 TOFA TEA KN 4 EKITI ARP KW 15 OBAFEMI OWODE WDE OG S/N LGA NAME LGA STATE 4 FIKA FKA YB 7 Trustfund Pensions Plc 0028 CODE CODE 13 JERE JRE BO 15 OVIA-SOUTH-WEST GBZ ED 27 27 OWERRI-WEST UMG IM 39 TSANYAWA TYW KN 5 IFELODUN SHA KW 16 ODEDAH DED OG CODE CODE 5 FUNE FUN YB 8 First Guarantee Pension Limited 0029 1 AGUATA AGU AN 14 KAGA KGG BO 16 OWAN-EAST -

Effectiveness of Small Plot Adoption Technology in Agricultural Development Programme, Birnin Kudu Local Government, Jigawa State, Nigeria
Engineering Research Journal | ISSN: 2782-8212 Vol. 1, Issue 6 (June, 2021) | www.ijaar.org EFFECTIVENESS OF SMALL PLOT ADOPTION TECHNOLOGY IN AGRICULTURAL DEVELOPMENT PROGRAMME, BIRNIN KUDU LOCAL GOVERNMENT, JIGAWA STATE, NIGERIA *ALI ABDU GIGINYU1, BALA ABDU2, HAYATU MISBAHU ABDULLAHI3 AND DANLADI BALA4 *1 Faculty of Education, Federal University Dutse, Email: [email protected] 2State Universal Basic Education Board, Jigawa State Email: [email protected] 3Department of Welding and Fabrication Engineering, Jigawa State Polytechnics Dutse Email: [email protected] 4 Nnamdi Azikiwe University, Anambra State, Nigeria, E-mail: [email protected] ABSTRACT The study investigated the Effectiveness of Small Plot Adoption Techniques (SPAT) in Agricultural Development Programmes in Birnin Kudu Local Government, Jigawa State, Nigeria The objectives of this study were to; identify the scope of small plot adoption technology programme in Birnin Kudu Local Government Area, determine effectiveness of the small pilot adoption technology on farmers’ productivity in Birnin Kudu Lacal Government Area and to examine the challenge facing small plot adoption technology programme in Birnin Kudu Local Government Area. The sample for this study comprised seventy seven (77) farmers and ten (10) extension agents. A stratified random sampling technique was used in selecting the sample from each category. The method of analysis findings of the study small plot adoption technology was found to be effective in terms of irrigation practice, feed formulation, livestock management, and storage technique and marketing. Small Plot Technology improves farmers’ income, accessibility of agricultural credit facility, accessibility of pest and herbicides respectively. The challenges facing SPAT in Birnin Kudu were inadequate number of extension agent’s lack of technical knowhow by extension workers to introduce new packages to farmers. -

(Nigeria) As the Growth Centre of Jigawa State A.A Jolaoye, Garba I.A
International Journal of Scientific & Engineering Research Volume 10, Issue 2, February-2019 300 ISSN 2229-5518 An Investigation into the Performance of Dutse (Nigeria) as the Growth Centre of Jigawa State A.A Jolaoye, Garba I.A Abstract— This paper seeks to investigate some key elements of a growth centre; the principle upon which local government headquarters and state capitals creation rest. It attempts to consider in a spatial dimension, the different channels by which the establishment and development of Dutse (Nigeria) has affected its’ region (the rest major settlements in the state) after twenty-seven years of operation. The paper categorized the effects into three distinct classes: direct, indirect and induced effects. The study area is Dutse Capital, Jigawa state, Nigeria. Particular issues considered are related to population movement, (migration and commuting), industrial linkages/interference, labour recruitment and shopping patterns. Primary data was gathered through closed- ended questionnaires administered to the city’s dwellers, the industrialists and their employees for the various aspect of the study. Descriptive analysis was adopted while presentation of the findings was done with charts and tables. The study reveals that the recruitment of labour has had some pronounced effects on the settlements in the region/state. That notwithstanding, industrial linkage and the gener- ation of economic activities is limited to Dutse itself. In other words, these effects have not appreciably affected the towns and villages in the state. The trickle-down effects of the growth centre have not manifested to a stage reliable enough to sustain economic growth in the state under the investigation Index Terms— Growth centre, region, population movement, industrial linkage, the trickle-down effect.