Effectiveness of Building Systems Strategies for Mitigation of Airborne Transmission of SARS-Cov-2
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Automatically Detects and Cleans the Air You Breathe
Automatically Detects and Cleans the Air you Breathe FAMILY BUSINESS S I N C E 1917 WHAT’S IN THE AIR? Indoor air can be up to 5x more polluted than outdoor air. Bacteria / Viruses Odors Allergens VOCs (Pollen & Ragweed, Mold, Pet Dander, (Volatile Organic Compounds, $2650Dust Mites) Cigarette Smoke, Smog) BAD$60 AIR IMPACTS$2650 THE BOTTOM LINE BILLION $220 BILLION DOLLARS THE AVERAGE COST OF ONE evaporates from the $60 EMPLOYEE SICK DAY IS BILLION economy every year in lost $2,650 8 productivity from sick days.6 PRODUCTIVITY In fact the EPA estimates that SickPRODUCTIVITY Building Syndrome alone is responsible for $60 BILLION IN LOST REVENUE.7 $2650 $60 THE BENEFITS OF CLEANER AIR BILLION BREATHE EASIER 99.97% of harmful germs, allergens and particulates are removed safely and easily.* PRODUCTIVITY INCREASED PRODUCTIVITY 9 Improved indoor air quality improves mental tasks, like concentration and recall, and can reduce absenteeism due to illness. REDUCED ODORS A chemical-free approach to removing odors and VOCs that can trigger allergies and headaches. *as small as 0.3 microns HOSPITAL-TYPE FILTRATION AeraMax® Air Purifiers feature a 4-Stage Purification 4 system similar to those used in hospitals to effectively 3 2 reduce the presence of airborne germs, allergens 1 and odors in the office environment. 1 CARBON FILTER 3 AERASAFE™ Removes odors and ANTIMICROBIAL captures large airborne TREATMENT particulates. Built-in protection from the growth of 2 TRUE HEPA FILTER odor causing bacteria, Captures 99.97% of mildew, and fungi on airborne particles as the True HEPA filter. small as 0.3 microns, ™ including pollen, 4 PLASMATRUE ragweed and other TECHNOLOGY allergens, viruses, Creates an ionized field germs, dust mites and to help safely remove mold spores. -

ASHRAE Position Document on Filtration and Air Cleaning
ASHRAE Position Document on Filtration and Air Cleaning Approved by ASHRAE Board of Directors January 29, 2015 Reaffirmed by Technology Council January 13, 2018 Expires January 23, 2021 ASHRAE 1791 Tullie Circle, NE • Atlanta, Georgia 30329-2305 404-636-8400 • fax: 404-321-5478 • www.ashrae.org © 2015 ASHRAE (www.ashrae.org). For personal use only. Additional reproduction, distribution, or transmission in either print or digital form is not permitted without ASHRAE's prior written permission. COMMITTEE ROSTER The ASHRAE Position Document on Filtration and Air Cleaning was developed by the Society's Filtration and Air Cleaning Position Document Committee formed on January 6, 2012, with Pawel Wargocki as its chair. Pawel Wargocki, Chair Dean A. Saputa Technical University of Denmark UV Resources Kongens Lyngby, Denmark Santa Clarita, CA Thomas H. Kuehn William J. Fisk University of Minnesota Lawrence Berkeley National Laboratory Minneapolis, MN Berkeley, CA H.E. Barney Burroughs Jeffrey A. Siegel Building Wellness Consultancy, Inc. The University of Toronto Johns Creek, GA Toronto, ON, Canada Christopher O. Muller Mark C. Jackson Purafil Inc. The University of Texas at Austin Doraville, GA Austin, TX Ernest A. Conrad Alan Veeck BOMA International National Air Filtration Association Washington DC Virginia Beach, VA Other contributors: Dean Tompkins Madison, WI for his contribution on photocatalytic oxidizers Paul Francisco, Ex-Officio Cognizant Committee Chair Environmental Health Committee University of Illinois Champaign, IL ASHRAE is a registered trademark in the U.S. Patent and Trademark Office, owned by the American Society of Heating, Refrigerating and Air-Conditioning Engineers, Inc. © 2015 ASHRAE (www.ashrae.org). For personal use only. -
Selection and Use of Portable Air Cleaners to Protect Workers from Exposure to SARS-Cov-2
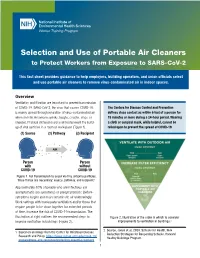
National Institute of Environmental Health Sciences Worker Training Program Selection and Use of Portable Air Cleaners to Protect Workers from Exposure to SARS-CoV-2 This fact sheet provides guidance to help employers, building operators, and union officials select and use portable air cleaners to remove virus-contaminated air in indoor spaces. Overview Ventilation and filtration are important to prevent transmission of COVID-19. SARS-CoV-2, the virus that causes COVID-19, The Centers for Disease Control and Prevention is mainly spread through inhalation of virus-contaminated air defines close contact as within 6 feet of a person for when an infected person speaks, laughs, coughs, sings, or 15 minutes or more during a 24-hour period. Wearing sneezes. Physical distancing alone will not prevent the build- a cloth or surgical mask, while helpful, cannot be up of viral particles in a room or workspace (Figure 1). relied upon to prevent the spread of COVID-19. (1) Source (2) Pathway (3) Recipient AIR Person Person with without COVID-19 COVID-19 Figure 1. For transmission to occur via tiny airborne particles, three things are necessary: source, pathway, and recipient.1 Approximately 40% of people who are infectious are asymptomatic (no symptoms) or presymptomatic (before symptoms begin) and may contaminate air unknowingly. Work settings with inadequate ventilation and/or those that require people to be close together for extended periods of time, increase the risk of COVID-19 transmission. The illustration at right outlines the recommended steps to Figure 2. Illustration of the order in which to consider improve ventilation in buildings (Figure 2). -

Effects of Temperature and Relative Humidity on Filter Loading by Simulated Atmospheric Aerosols & COVID-19 Related Mask and Respirator Filtration Study
Effects of Temperature and Relative Humidity on Filter Loading by Simulated Atmospheric Aerosols & COVID-19 Related Mask and Respirator Filtration Study A DISSERTATION SUBMITTED TO THE FACULTY OF THE UNIVERSITY OF MINNESOTA BY Chenxing Pei IN PARTIAL FULFILLMENT OF THE REQUIREMENTS FOR THE DEGREE OF DOCTOR OF PHILOSOPHY Dr. David Y.H. Pui, Advisor August 2020 © Chenxing Pei 2020 Acknowledgments First and foremost, I am deeply indebted to my advisor, Professor David Y. H. Pui, for his continuous guidance, mentoring, and inspiration throughout my undergraduate and graduate studies. He provided me with the encouragement and freedom to work on any filtration related studies that interested me. His support, patience, and trust have made my years spent in the Particle Technology Laboratory an enjoyable, enriching, and memorable experience in my life. I would like to express my deepest appreciation to my committee members: Prof. Thomas Kuehn, Prof. David Kittelson, and Prof. Kevin Janni for reviewing my dissertation, offering insightful comments and suggestions, and serving on my Ph. D. exam committees. I am extremely grateful to my committee members not only for their time and extreme patience, but for their intellectual contributions to my development as a scientist. I would also like to thank Dr. Qisheng Ou, whose help cannot be overestimated. Dr. Ou provided me with the tools that I needed to choose the right direction and successfully complete my dissertation. Special thanks to Dr. Young H. Chung, who led to many interesting and motivating discussions. His help and advice were invaluable for my research and life. Thanks also to Weiqi Chen, who collaborated with me on the smart sensor project. -

Efficacy of Portable Air Cleaners and Masking for Reducing Indoor Exposure to Simulated Exhaled SARS-Cov-2 Aerosols — United States, 2021
Morbidity and Mortality Weekly Report Efficacy of Portable Air Cleaners and Masking for Reducing Indoor Exposure to Simulated Exhaled SARS-CoV-2 Aerosols — United States, 2021 William G. Lindsley, PhD1; Raymond C. Derk, MS1; Jayme P. Coyle, PhD1; Stephen B. Martin, Jr., PhD2; Kenneth R. Mead, PhD3; Francoise M. Blachere, MS1; Donald H. Beezhold, PhD1; John T. Brooks, MD4; Theresa Boots, MS1; John D. Noti, PhD1 On July 2, 2021, this report was posted as an MMWR Early conference room with a heating, ventilation, and air condition- Release on the MMWR website (https://www.cdc.gov/mmwr). ing (HVAC) system that provided 0.1 m3 per second of air flow SARS-CoV-2, the virus that causes COVID-19, can be (202 ft3 per minute; two air changes per hour) with no air spread by exposure to droplets and aerosols of respiratory fluids recirculation. Two HEPA air cleaners (Honeywell 50250-S, that are released by infected persons when they cough, sing, Kaz Inc.) were used, each rated to provide 250 ft3 per minute talk, or exhale. To reduce indoor transmission of SARS-CoV-2 (0.12 m3 per second) of air filtration for a combined total of between persons, CDC recommends measures including 5.2 air changes per hour. The two air cleaners were used in four physical distancing, universal masking (the use of face masks different locations: 1) center of the room on the floor behind in public places by everyone who is not fully vaccinated), and the source simulator; 2) left and right sides of the room on the increased room ventilation (1). -

AHAM Comments
December 6, 2018 Via E-Mail Robert Burchard U.S. Environmental Protection Agency [email protected] Re: ENERGY STAR Room Air Cleaners Version 2.0 Specification Discussion Guide Dear Mr. Burchard: On behalf of the Association of Home Appliance Manufacturers (AHAM), I would like to provide our comments on the ENERGY STAR Room Air Cleaners Version 2.0 Specification Discussion Guide (Oct. 2018). AHAM represents manufacturers of major, portable and floor care home appliances, and suppliers to the industry. AHAM’s membership includes over 150 companies throughout the world. In the U.S., AHAM members employ tens of thousands of people and produce more than 95% of the household appliances shipped for sale. The factory shipment value of these products is more than $30 billion annually. The home appliance industry, through its products and innovation, is essential to U.S. consumer lifestyle, health, safety and convenience. Through its technology, employees and productivity, the industry contributes significantly to U.S. jobs and economic security. Home appliances also are a success story in terms of energy efficiency and environmental protection. New appliances often represent the most effective choice a consumer can make to reduce home energy use and costs. AHAM supports EPA and the Department of Energy (DOE) in their efforts to provide incentives to manufacturers, retailers, and consumers for energy efficiency improvement, as long as product performance can be maintained for the consumer. AHAM strongly supports a change from dust CADR to smoke CADR which is used to calculate room size and is a proxy for the smallest particulates in consumers’ homes. -

Investigations on Parameters for Analysing Effectiveness of an Air Purification System
Publication Since 2012 | ISSN: 2321-9939 | ©IJEDR 2020 Year 2020, Volume 8, Issue 3 Investigations On Parameters For Analysing Effectiveness Of An Air Purification System 1Saurabh Dhanpal Bankar, 2Dr. Dheeraj Deshmukh 1Student, 2Associate Professor G H Raisoni College of Engineering, Nagpur _____________________________________________________________________________________________________ Abstract - Pollution has turn out to be a part of our day to day activities due to modernisation and unsustainability issues, therefore degrading place for stay in and making it a hell for our future generations. With or without our understanding constantly heading towards to a time, when everyones live turn out to be a point of starvation. Owing to indoor air pollution children are deadliest victims and air as an essential element, stays uncontrollable not like other pollutions. All humans cannot easily visualise indoor air pollution except it gets mentioned on our medicals reports. Investigation on parameters associated with air purification system methodology begins with analyzing various trends in indoor air pollution via facts available, continuing mitigation measures, and finalizing a measure which needs concentration and feasible are carried out. It is observed that filtration is a measure that desires to be integrated with various innovations in the related field. In this paper, all required and desired parameters and methods available are focused and summarised for development of better air purification system. keywords - Air Purifier, Indoor -

From Wikipedia, the Free Encyclopediathis Article Is About
HVAC From Wikipedia, the free encyclopediaThis article is about heating, ventilation, and air conditioning; HVAC may also stand for high-voltage alternating current."Climate control" redirects here. For efforts to reduce changes to Earth's climate, see Climate change mitigation. Rooftop HVAC unit with view of fresh air intake vent. Ventilation duct with outlet vent. These are installed throughout a building to move air in or out of a room. HVAC (heating, ventilating, and air conditioning; also heating, ventilation, and air conditioning)[1] is the technology of indoor and vehicular environmental comfort. Its goal is to provide thermal comfort and acceptable indoor air quality. HVAC system design is a subdiscipline of mechanical engineering, based on the principles of thermodynamics, fluid mechanics, and heat transfer. Refrigeration is sometimes added to the field's abbreviation as HVAC&R or HVACR, or ventilating is dropped as in HACR (such as the designation of HACR-rated circuit breakers). HVAC is important in the design of medium to large industrial and office buildings such as skyscrapers and in marine environments such as aquariums, where safe and healthy building conditions are regulated with respect to temperature and humidity, using fresh air from outdoors. Ventilating or Ventilation (the V in HVAC) is the process of "changing" or replacing air in any space to provide high indoor air quality which involves temperature control, oxygen replenishment, and removal of moisture, odors, smoke, heat, dust, airborne bacteria, and carbon dioxide. Ventilation removes unpleasant smells and excessive moisture, introduces outside air, keeps interior building air circulating, and prevents stagnation of the interior air. -

Improving Ventilation and Indoor Air Quality During Wildfire Smoke Events Recommendations for Schools and Buildings with Mechanical Ventilation
Improving Ventilation and Indoor Air Quality during Wildfire Smoke Events Recommendations for Schools and Buildings with Mechanical Ventilation Overview • Smoke is a complex mixture of carbon dioxide (CO2), water vapor, carbon monoxide (CO), hydrocarbons, other organic chemicals, nitrogen oxides (NOX), trace minerals, and particulate matter. o Particulate matter consists of solid particles and liquid droplets suspended in the air. Particles with diameters less than 10 microns (PM10) are upper respiratory tract and eye irritants. o Smaller particles (PM2.5) are the greatest health concern – they can be inhaled deep into the lungs, and can affect respiratory and heart health. o Carbon monoxide, a colorless, odorless gas produced by incomplete combustion, is a particular health concern and levels are highest during the smoldering stages of a fire. • Outdoor (ambient) air pollutants, including smoke, enter and leave buildings in three primary ways: 1. Mechanical ventilation systems, which actively draw in outdoor air through intake vents and distribute it throughout the building. 2. Natural ventilation (opening of doors or windows). 3. Infiltration, the passive entry of unfiltered outdoor air through small cracks and gaps in the building shell. • Tightly closed buildings reduce exposure to outdoor air pollution. Upgrading the filter efficiency of the heating, ventilating, and air-conditioning (HVAC) system and changing filters frequently during smoke events greatly improves indoor air quality. Supplementing with HEPA filters, particularly those with activated charcoal or other adsorbents, improves air quality even more. • During long-term smoke events, take advantage of periods of improved air quality (such as during rain or shifts in wind) to use natural ventilation to flush-out the building. -

Effectiveness of Portable Air Cleaners in Particulate Contaminant Removal
10710 EFFECTIVENESS OF PORTABLE AIR CLEANERS IN PARTICULATE CONTAMINANT REMOVAL P. Gricar, P. Novak University of Ljubljana, Faculty of Mechanical Engineering 5 Askerceva 6, 1000 Ljubljana, Slovenia ABSTRACT The primary objective of this study was to evaluate the effectiveness of different commercially available portable indoor air cleaning technologies in removing dust particulates from the indoor air. Suspended respirable particles are of great concern and often identified as important source of indoor air quality problems. The concentrations of particulate and gaseous pollutants encountered in the indoor environment frequently exceed those found outdoors by factor ranging from 2 to 20. Indoor particulates and some contaminants are found to cause or worsen respiratory ailments like asthma and allergies. Commercially available air cleaners with different sets of air filters were tested in a test chamber according to modified ANSI/AHAM AC-I 1988. The number of airborne particles v ithin a set of fixed size ranges was measured with a laser light scattering instrument. The purpose of the study was to test how effectively different sets of filters remove the particulates from the air. The types of filters used were fibrous filters for coarse particles, electrostatic precipitators, electronic filters and HEPA tilter. Some devices have incorporated the use of activated charcoal to remove gaseous contaminants from the air but these contaminants were not evaluated in this study. It was seen that different air cleaners perform very different in terms of their efficiency. What determines the overall rate of removal or the space cleaning efficiency is the product of the air flow rate through the air cleaner and filter efficiency. -

OHA 3725 R COVID 19 Public Health Recommendations: Indoor Air
OFFICE OF THE DIRECTOR Kate Brown, Governor 500 Summer St NE E20 Salem OR 97301 Voice: 503-947-2340 Fax: 503-947-2341 June 30, 2021 COVID-19 Public Health Recommendations: Indoor air considerations for smaller spaces Improved indoor air quality is associated with improved productivity and better health outcomes, regardless of COVID-19. Improvements on those conditions, where needed, will be an investment that can provide benefits extending beyond mitigating infectious disease transmission. Indoor air spaces need special consideration because of COVID-19 transmission potential from the buildup in air of aerosols that we generate from breathing, talking, laughing, shouting, singing, coughing, and sneezing. Maintaining a distance of at least 6 feet between people will help prevent exposure to droplets that we emit, but smaller particles or aerosols can be airborne for minutes to hours depending on ventilation, humidity, and other indoor space factors. Poor ventilation of indoor settings, with larger numbers of people, significantly increases the risk of viral transmission. Below are steps that building managers and property owners can take to improve the indoor air quality in the settings they manage. In general, these steps aim to 1) increase the amount of fresh outside air that is introduced into the system, 2) exhaust air from indoors to the outdoors, and 3) clean the air that is recirculated indoors by using various filtration methods (e.g., HEPA filters) to remove virus-containing particles from the air. Ventilation public health recommendations for indoor spaces • Increase outdoor ventilation of clean air into indoor spaces. • Aim for fewer people in larger rooms. -
Improving Indoor Air Quality Through Botanical Air Filtration in Energy Efficient Residences Daniel William Newkirk Purdue University
Purdue University Purdue e-Pubs Open Access Theses Theses and Dissertations Spring 2014 Improving Indoor Air Quality through Botanical Air Filtration in Energy Efficient Residences Daniel William Newkirk Purdue University Follow this and additional works at: https://docs.lib.purdue.edu/open_access_theses Part of the Mechanical Engineering Commons, and the Oil, Gas, and Energy Commons Recommended Citation Newkirk, Daniel William, "Improving Indoor Air Quality through Botanical Air Filtration in Energy Efficient Residences" (2014). Open Access Theses. 228. https://docs.lib.purdue.edu/open_access_theses/228 This document has been made available through Purdue e-Pubs, a service of the Purdue University Libraries. Please contact [email protected] for additional information. *UDGXDWH6FKRRO(7')RUP 5HYLVHG 01 14 PURDUE UNIVERSITY GRADUATE SCHOOL Thesis/Dissertation Acceptance 7KLVLVWRFHUWLI\WKDWWKHWKHVLVGLVVHUWDWLRQSUHSDUHG %\ Daniel W. Newkirk (QWLWOHG Improving Indoor Air Quality through Botanical Air Filtration in Energy Efficient Residences Master of Science )RUWKHGHJUHHRI ,VDSSURYHGE\WKHILQDOH[DPLQLQJFRPPLWWHH William Hutzel Michael Dana Ming Qu 7RWKHEHVWRIP\NQRZOHGJHDQGDVXQGHUVWRRGE\WKHVWXGHQWLQWKH Thesis/Dissertation Agreement. Publication Delay, and Certification/ Disclaimer (Graduate Schoo l Form 32 ) WKLVWKHVLVGLVVHUWDWLRQ adheres to the provisions of 3XUGXH8QLYHUVLW\¶V³3ROLF\RQ,QWHJULW\LQ5HVHDUFK´DQGWKHXVHRI FRS\ULJKWHGPDWHULDO William J. Hutzel $SSURYHGE\0DMRU3URIHVVRU V BBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBB BBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBB