R-Codox-M / R-Ivac Indication
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

How Can We Create Environments Where Hate Cannot Flourish?
How can we create environments where hate cannot flourish? Saturday, February 1 9:30 a.m. – 10:00 a.m. Check-In and Registration Location: Field Museum West Entrance 10:00 a.m. – 10:30 a.m. Introductions and Program Kick-Off JoAnna Wasserman, USHMM Education Initiatives Manager Location: Lecture Hall 1 10:30 a.m. – 11:30 a.m. Watch “The Path to Nazi Genocide” and Reflections JoAnna Wasserman, USHMM Education Initiatives Manager Location: Lecture Hall 1 11:30 a.m. – 11:45 a.m. Break and walk to State of Deception 11:45 a.m. – 12:30 p.m. Visit State of Deception Interpretation by Holocaust Survivor Volunteers from the Illinois Holocaust Museum Location: Upper level 12:30 p.m. – 1:00 p.m. Breakout Session: Reflections on Exhibit Tim Kaiser, USHMM Director, Education Initiatives David Klevan, USHMM Digital Learning Strategist JoAnna Wasserman, USHMM Education Initiatives Manager Location: Lecture Hall 1, Classrooms A and B Saturday, February 2 (continued) 1:00 p.m. – 1:45 p.m. Lunch 1:45 p.m. – 2:45 p.m. A Survivor’s Personal Story Bob Behr, USHMM Survivor Volunteer Interviewed by: Ann Weber, USHMM Program Coordinator Location: Lecture Hall 1 2:45 p.m. – 3:00 p.m. Break 3:00 p.m. – 3:45 p.m. Student Panel: Beyond Indifference Location: Lecture Hall 1 Moderator: Emma Pettit, Sustained Dialogue Campus Network Student/Alumni Panelists: Jazzy Johnson, Northwestern University Mary Giardina, The Ohio State University Nory Kaplan-Kelly, University of Chicago 3:45 p.m. – 4:30 p.m. Breakout Session: Sharing Personal Reflections Tim Kaiser, USHMM Director, Education Initiatives David Klevan, USHMM Digital Learning Strategist JoAnna Wasserman, USHMM Education Initiatives Manager Location: Lecture Hall 1, Classrooms A and B 4:30 p.m. -
The Utility of Genetic Risk Scores in Predicting the Onset of Stroke March 2021 6
DOT/FAA/AM-21/24 Office of Aerospace Medicine Washington, DC 20591 The Utility of Genetic Risk Scores in Predicting the Onset of Stroke Diana Judith Monroy Rios, M.D1 and Scott J. Nicholson, Ph.D.2 1. KR 30 # 45-03 University Campus, Building 471, 5th Floor, Office 510 Bogotá D.C. Colombia 2. FAA Civil Aerospace Medical Institute, 6500 S. MacArthur Blvd Rm. 354, Oklahoma City, OK 73125 March 2021 NOTICE This document is disseminated under the sponsorship of the U.S. Department of Transportation in the interest of information exchange. The United States Government assumes no liability for the contents thereof. _________________ This publication and all Office of Aerospace Medicine technical reports are available in full-text from the Civil Aerospace Medical Institute’s publications Web site: (www.faa.gov/go/oamtechreports) Technical Report Documentation Page 1. Report No. 2. Government Accession No. 3. Recipient's Catalog No. DOT/FAA/AM-21/24 4. Title and Subtitle 5. Report Date March 2021 The Utility of Genetic Risk Scores in Predicting the Onset of Stroke 6. Performing Organization Code 7. Author(s) 8. Performing Organization Report No. Diana Judith Monroy Rios M.D1, and Scott J. Nicholson, Ph.D.2 9. Performing Organization Name and Address 10. Work Unit No. (TRAIS) 1 KR 30 # 45-03 University Campus, Building 471, 5th Floor, Office 510, Bogotá D.C. Colombia 11. Contract or Grant No. 2 FAA Civil Aerospace Medical Institute, 6500 S. MacArthur Blvd Rm. 354, Oklahoma City, OK 73125 12. Sponsoring Agency name and Address 13. Type of Report and Period Covered Office of Aerospace Medicine Federal Aviation Administration 800 Independence Ave., S.W. -

M.'S Story Jay and Tava Musial, Who Were Living in Michigan at the Time
M.’s Story Jay and Tava Musial, who were living in Michigan at the time, had planned a family trip for Memorial Day weekend, but not before stopping by their daughter’s pediatrician’s office. Tava had noticed her daughter M. Rhapsody frequently had to go to the bathroom. Assuming she had a urinary tract infection, they hoped to get antibiotics and be on their way. M.’s lab work revealed no signs of bacteria but indicated her blood sugar was extremely high. Five days after her eighth birthday, M. was diagnosed with Type 1 diabetes. The Musials’ weekend getaway quickly rerouted to St. John’s Hospital in Detroit where M. spent a full week learning how to manage diabetes. Shortly after M’s diagnosis, the Musial family relocated to Sheppard Air Force Base in Wichita Falls, Texas. Relocating also meant finding a new endocrinologist for M. It was at that first appointment that Dr. John Caras recommended Diabetes Education at United Regional. Diabetes is a disease that affects the whole family, especially when a child is diagnosed. Diabetes Education also provides a support group for kids and their families. “M. comes to every appointment with a smile on her face and has never let her diabetes hold her back on anything,” said Nicole Benz, Diabetes Nurse Educator at United Regional. Children’s Miracle Network at United Regional provides scholarships for kids with Type 1 Diabetes to go to Camp Sweeney. This three-week camp’s goal is that every child who attends camp will not only learn about his or her condition but will find the inner strength each day to do what it takes to live a healthy lifestyle. -

“Bo Diddley” and “I'm a Man” (1955)
“Bo Diddley” and “I’m a Man” (1955) Added to the National Registry: 2011 Essay by Ed Komara (guest post)* Bo Diddley While waiting in Bo Diddley’s house to conduct an interview for the February 12, 1987 issue of “Rolling Stone,” journalist Kurt Loder noticed a poster. “If You Think Rock and Roll Started With Elvis,” it proclaimed, “You Don’t Know Diddley.” This statement seems exaggerated, but upon listening to Diddley’s April 1955 debut 78 on Checker 814, “Bo Diddley” backed with “I’m A Man,” it becomes apt, perhaps even understated. Bo Diddley (1928-2008) described his own place in music history to Loder. “People wouldn’t even bother with no stuff like ‘Bo Diddley’ and ‘I’m A Man’ and stuff like that ten years earlier [circa 1945] or even a year earlier [1954]. Then Leonard and Phil Chess decided to take a chance, and suddenly a whole different scene, a different kind of music, came in. And that was the beginning of rock and roll.” The composer credit for Checker 814 reads “E. McDaniels,” and there begins the tale. Bo Diddley was born Ellas Otha Bates in McComb, Mississippi on December 30, 1928 to a teenage mother and her local boyfriend. He was raised, however, by his maternal first cousin, Gussie McDaniel, to whom he was taken to Chicago, and given her surname McDaniel. He grew up on the South Side of the city, where he learned violin, trombone and, at age 12, the guitar. Before long, he was playing for change on the local streets. -

List of Approved Special Characters
List of Approved Special Characters The following list represents the Graduate Division's approved character list for display of dissertation titles in the Hooding Booklet. Please note these characters will not display when your dissertation is published on ProQuest's site. To insert a special character, simply hold the ALT key on your keyboard and enter in the corresponding code. This is only for entering in a special character for your title or your name. The abstract section has different requirements. See abstract for more details. Special Character Alt+ Description 0032 Space ! 0033 Exclamation mark '" 0034 Double quotes (or speech marks) # 0035 Number $ 0036 Dollar % 0037 Procenttecken & 0038 Ampersand '' 0039 Single quote ( 0040 Open parenthesis (or open bracket) ) 0041 Close parenthesis (or close bracket) * 0042 Asterisk + 0043 Plus , 0044 Comma ‐ 0045 Hyphen . 0046 Period, dot or full stop / 0047 Slash or divide 0 0048 Zero 1 0049 One 2 0050 Two 3 0051 Three 4 0052 Four 5 0053 Five 6 0054 Six 7 0055 Seven 8 0056 Eight 9 0057 Nine : 0058 Colon ; 0059 Semicolon < 0060 Less than (or open angled bracket) = 0061 Equals > 0062 Greater than (or close angled bracket) ? 0063 Question mark @ 0064 At symbol A 0065 Uppercase A B 0066 Uppercase B C 0067 Uppercase C D 0068 Uppercase D E 0069 Uppercase E List of Approved Special Characters F 0070 Uppercase F G 0071 Uppercase G H 0072 Uppercase H I 0073 Uppercase I J 0074 Uppercase J K 0075 Uppercase K L 0076 Uppercase L M 0077 Uppercase M N 0078 Uppercase N O 0079 Uppercase O P 0080 Uppercase -

Proposal for Generation Panel for Latin Script Label Generation Ruleset for the Root Zone
Generation Panel for Latin Script Label Generation Ruleset for the Root Zone Proposal for Generation Panel for Latin Script Label Generation Ruleset for the Root Zone Table of Contents 1. General Information 2 1.1 Use of Latin Script characters in domain names 3 1.2 Target Script for the Proposed Generation Panel 4 1.2.1 Diacritics 5 1.3 Countries with significant user communities using Latin script 6 2. Proposed Initial Composition of the Panel and Relationship with Past Work or Working Groups 7 3. Work Plan 13 3.1 Suggested Timeline with Significant Milestones 13 3.2 Sources for funding travel and logistics 16 3.3 Need for ICANN provided advisors 17 4. References 17 1 Generation Panel for Latin Script Label Generation Ruleset for the Root Zone 1. General Information The Latin script1 or Roman script is a major writing system of the world today, and the most widely used in terms of number of languages and number of speakers, with circa 70% of the world’s readers and writers making use of this script2 (Wikipedia). Historically, it is derived from the Greek alphabet, as is the Cyrillic script. The Greek alphabet is in turn derived from the Phoenician alphabet which dates to the mid-11th century BC and is itself based on older scripts. This explains why Latin, Cyrillic and Greek share some letters, which may become relevant to the ruleset in the form of cross-script variants. The Latin alphabet itself originated in Italy in the 7th Century BC. The original alphabet contained 21 upper case only letters: A, B, C, D, E, F, Z, H, I, K, L, M, N, O, P, Q, R, S, T, V and X. -

5 Curl-Free Fields and Electrostatic Potential
5Curl-freefieldsandelectrostaticpotential • Mathematically, we can generate a curl-free vector field E(x, y, z) as ∂V ∂V ∂V E = −( , , ), ∂x ∂y ∂z by taking the gradient of any scalar function V (r)=V (x, y, z).The gradient of V (x, y, z) is defined to be the vector ∂V ∂V ∂V ∇V ≡ ( , , ), ∂x ∂y ∂z pointing in the direction of increasing V ;inabbreviatednotation,curl- free fields E can be indicated as E = −∇V. – Verification: Curl of vector ∇V is xˆ yˆ zˆ ! ∂ ∂ ∂ ! ∇×(∇V )=! ∂x ∂y ∂z ! =ˆx0 − yˆ0 − zˆ0=0. ! ∂V ∂V ∂V ! ! ! ! ∂x ∂y ∂z ! ! ! – If E = −∇V represents! an electrostatic! field,thenV is called the electrostatic potential. ◦ Simple dimensional analysis indicates that units of electro- static potential must be volts (V). 1 – The prescription E = −∇V ,includingtheminussign(optional, but taken by convention in electrostatics), ensures that electro- static field E points from regions of “high potential” to “low po- tential” as illustrated in the next example. Electrostatic fields E point from regions of “high V ” to “low V ” Example 1: Given an electrostatic potential V (x, y, z)=x2 − 6y V 4 in a certain region of space, determine the corresponding electrostatic field E = −∇V in the same region. 2 Solution: The electrostatic field is ∂ ∂ ∂ 0 E = −∇(x2 − 6y)=−( , , )(x2 − 6y)=(−2x, 6, 0) = −xˆ 2x +ˆy6 V/m. ∂x ∂y ∂z !2 Note that this field is directed from regions of high potentialtolowpotential.Alsonote that electric field vectors are perpendicular everywhere to “equipotential” contours. !4 !4 !2 0 2 4 Given an electrostatic potential V (x, y, z),findingthecorrespondingelec- Light colors indicate “high V ” trostatic field E(x, y, z) is a straightforward procedure (taking the negative dark colors “low V ” gradient) as already illustrated in Example 1. -

Fonts for Latin Paleography
FONTS FOR LATIN PALEOGRAPHY Capitalis elegans, capitalis rustica, uncialis, semiuncialis, antiqua cursiva romana, merovingia, insularis majuscula, insularis minuscula, visigothica, beneventana, carolina minuscula, gothica rotunda, gothica textura prescissa, gothica textura quadrata, gothica cursiva, gothica bastarda, humanistica. User's manual 5th edition 2 January 2017 Juan-José Marcos [email protected] Professor of Classics. Plasencia. (Cáceres). Spain. Designer of fonts for ancient scripts and linguistics ALPHABETUM Unicode font http://guindo.pntic.mec.es/jmag0042/alphabet.html PALEOGRAPHIC fonts http://guindo.pntic.mec.es/jmag0042/palefont.html TABLE OF CONTENTS CHAPTER Page Table of contents 2 Introduction 3 Epigraphy and Paleography 3 The Roman majuscule book-hand 4 Square Capitals ( capitalis elegans ) 5 Rustic Capitals ( capitalis rustica ) 8 Uncial script ( uncialis ) 10 Old Roman cursive ( antiqua cursiva romana ) 13 New Roman cursive ( nova cursiva romana ) 16 Half-uncial or Semi-uncial (semiuncialis ) 19 Post-Roman scripts or national hands 22 Germanic script ( scriptura germanica ) 23 Merovingian minuscule ( merovingia , luxoviensis minuscula ) 24 Visigothic minuscule ( visigothica ) 27 Lombardic and Beneventan scripts ( beneventana ) 30 Insular scripts 33 Insular Half-uncial or Insular majuscule ( insularis majuscula ) 33 Insular minuscule or pointed hand ( insularis minuscula ) 38 Caroline minuscule ( carolingia minuscula ) 45 Gothic script ( gothica prescissa , quadrata , rotunda , cursiva , bastarda ) 51 Humanist writing ( humanistica antiqua ) 77 Epilogue 80 Bibliography and resources in the internet 81 Price of the paleographic set of fonts 82 Paleographic fonts for Latin script 2 Juan-José Marcos: [email protected] INTRODUCTION The following pages will give you short descriptions and visual examples of Latin lettering which can be imitated through my package of "Paleographic fonts", closely based on historical models, and specifically designed to reproduce digitally the main Latin handwritings used from the 3 rd to the 15 th century. -

Kathleen M. O'neill
Kathleen M. O'Neill Associate T: +1.312.499.6366 70 West Madison Street, 48th Floor F: +1.619.515.4181 Chicago, IL 60602 [email protected] Kathleen M. O'Neill is an associate in the Corporate Practice Group in the firm's Chicago office. Areas of Practice Kathleen focuses her practice on mergers and acquisitions, corporate governance and operations, and regulatory advising for clients in the healthcare industry. Kathleen is dedicated to understanding each client’s needs to assist them in navigating legal issues and achieving desired outcomes. Kathleen advises clients regularly on structuring considerations and risk mitigation strategies in transactions. Kathleen’s transactional practice is supported by her experience with federal and state law governing corporate practice of medicine, fraud and abuse, licensure, commercial and governmental payor reimbursement, and peer review/fair hearings, including related state and federal reporting requirements. As a former registered nurse, Kathleen’s clinical experience and insight inform her practical understanding of the issues and concerns clients face in doing business in the healthcare industry. She is passionate about serving clients effectively, thereby enabling them to serve patients, providers, and other stakeholders. Before joining the firm, Kathleen began her legal career at another prominent healthcare firm in Chicago. She attended Northwestern University Pritzker School of Law, graduated with high honors, and was named to the Order of the Coif. During law school, Kathleen was a Note and Comment Editor for the Northwestern Journal of Law and Social Policy. Prior to attending Northwestern, Kathleen worked for several years as a registered nurse at the University of Chicago, and continues to hold a registered professional nurse license in Illinois. -

John M. O'neal
John M. O'Neal Partner John O'Neal is a tenacious advocate for his clients both inside and outside the court room. John's practice includes the following areas: • Corporate and commercial matters, including contract disputes, defense and assertion of claims related to officers and directors, shareholder and LLC member disputes, commercial torts, non- solicitation and non-compete agreements, creditor claims, and insurance claims. • Real estate matters, including title claims, contract disputes, real estate professional claims, commission disputes, construction matters, lien claims, lease enforcement and defense, and administrative claims. • Securities matters, including defense of state and federal claims. • Defense and prosecution of professional liability claims and select personal and financial injury matters. [email protected] Representative Experience Phoenix Office • Obtained dismissal of securities claims against board of directors Tel: (602) 229-5436 and officers of a publicly traded company Fax: (602) 417-2923 • Obtained unanimous defense jury verdict for municipality in a $100 million breach of contract/promissory estoppel case • Prevailed on summary judgement on multimillion dollar claims against a national bank for alleged dangerous real property conditions • Prevailed at arbitration for investment firm's commission claim Legal Services • Real Estate and Construction Litigation • Banking & Financial Institutions • Litigation & Dispute Resolution • Financial Institutions Litigation • Securities Litigation Education and Honors -

Flourish: Positive Psychology and Positive Interventions
Flourish: Positive Psychology and Positive Interventions MARTIN SELIGMAN T T L H V Delivered at e University of Michigan October , ¥ works on positive psychology, learned helplessness, depression, optimism, and pessimism. He is currently Zellerbach Family Professor of Psychology in the Department of Psychology at the Univer- sity of Pennsylvania and the director of the Positive Psychology Center. He was elected president of the American Psychological Association in by the largest vote in history. Dr. Seligman’s bibliography includes twenty-one books and more than articles. Among his better-known works are the best-selling Authentic Happiness (), Helplessness ( ), Learned Optimism ( ), What You Can Change and What You Can’t ( ), e Optimistic Child ( ), and Character Strengths and Virtues (, with Christopher Peterson). His books have been translated into more than thirty languages. His latest book is Flourish (). Dr. Seligman is the recipient of three Distinguished Scientic Contri- bution Awards from the American Psychological Association, the Laurel Award of the American Association for Applied Psychology and Preven- tion, the Lifetime Achievement Award of the Society for Research in Psychopathology, and the rst Wiley Psychology Lifetime Award of the British Academy. § § Á ¶ We have a strange heritage about the positive and negative sides of life. Our heritage comes from Schopenhauer and Freud who told us that the best we can ever hope for is to keep our misery and suering to a mini- mum. I want to suggest today the possibility of a positive human future. Until the possibility that there is more to life than minimizing suering gets on the radar screen, a positive human future is much less likely. -
Ju N E 20 21 M E Nu
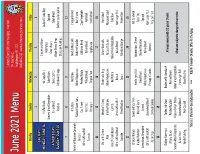
Dutchess County Offi ce for the Aging - Nutrition 114 Delafi eld St Poughkeepsie NY 12601 June 2021 Menu (845) 486-2555 • www.dutchessny.gov/ofanutrition Monday Tuesday Wednesday Thursday Friday 1 2 3 4 FLAG DAY Chicken and Gravy MONDAY, JUNE 14 Stuff ed Shells Hot Dogs/Rolls Seafood Creole Rice Red Potato Sonoma Mixed Vegetables Baked Beans Spinach Green Beans FATHER’S DAY Italian Bread Sliced Carrots Italian Bread Whole Wheat Bread SUNDAY, JUNE 20 Peaches Mandarin Orange Snickerdoodle Cookies Chocolate Pudding 7 8 9 10 11 Ham Steak Beef Stew Swedish Meatballs Cheese Omelet Beef and Macaroni Casserole Mashed Sweet Yams Mixed Vegetables Bu ered Noodles Hash Brown Broccoli Caulifl ower Parslied Potato California Blend Capri Vegetable Whole Wheat Roll Rye Bread Wheat Bread Italian Bread Rye Bread Apricots Pineapple Tropical Fruit Applesauce Fruit Cocktail 14 15 16 17 18 Chili with Cheese Meatloaf / Gravy Chicken a la King Italian Meatballs Ham Salad Rice Mashed Potatoes Mixed Vegetables Pasta with Sauce Macaroni Salad French Green Beans Carrots Red Potato Italian Mixed Vegetables Cole Slaw Whole Wheat Bread Whole Wheat Roll Biscuit Italian Bread Hamburger Roll Cupcake Sliced Peaches Apple Mandarin Orange Protein Bar 21 22 23 24 25 Chicken Marsala Sweet and Sour Pork Fish Sandwich Hamburger / Roll Macaroni and Cheese Mashed Potatoes Rice and Beans Tater Tots Baked Beans Stewed Tomatoes Green Bean Almondine Broccoli Spinach Mixed Vegetables Italian Bread Whole Wheat Roll Stonewheat Bread Hamburger Roll Pineapple Chunks Apricots Apple Crisp Oatmeal Cookies Tropical Fruit 28 29 30 Chicken Parmesan Turkey and Gravy Barbecue Rib Sandwich All meals served with 1/2 pint of 1% milk Zi and Sauce Parslied Potatoes Rice and Beans Sonoma Mixed Vegetables Peas and Pearl Onions Italian Mixed Vegetables Meals are subject to change without no ce Italian Bread Stonewheat Bread Hamburger Roll Vanilla Pudding Fruit Cocktail Sliced Peaches Marcus J.