Cannock Chase CCG Governing Body Meeting (IN PUBLIC)
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Surface Water Management Plan Phase 1
Southern Staffordshire Surface Water Management Plan Phase 1 Stafford Borough, Lichfield District, Tamworth Borough, South Staffordshire District and Cannock Chase District Councils July 2010 Final Report 9V5955 CONTENTS Page 1 INTRODUCTION 1 1.1 General Overview 1 1.2 Objectives of the SWMP 1 1.3 Scope of the SWMP 3 1.3.1 Phase 1 - Preparation 5 1.3.2 Phase 2 - Risk Assessment 5 2 ESTABLISHING A PARTNERSHIP 7 2.1 Identification of Partners 7 2.2 Roles and Responsibilities 9 2.3 Engagement Plan 10 2.4 Objectives 10 3 COLLATE AND MAP INFORMATION 11 3.1 Data Collection and Quality 11 3.1.1 Historic Flood Event Data 12 3.1.2 Future Flood Risk Data 15 3.2 Mapping and GIS 18 3.2.1 Surface Water Flooding 18 3.2.2 Flood Risk Assets 19 3.2.3 SUDS Map 19 3.2.4 Summary Sheets 20 4 STAFFORD BOROUGH 23 4.1 Surface Water Flood Risk 23 4.2 Surface Water Management 24 4.3 Recommendations 25 5 LICHFIELD DISTRICT 27 5.1 Surface Water Flood Risk 27 5.2 Surface Water Management 28 5.2.1 Canal Restoration 29 5.3 Recommendations 31 6 TAMWORTH BOROUGH 33 6.1 Surface Water Flood Risk 33 6.2 Surface Water Management 34 6.3 Recommendations 35 7 SOUTH STAFFORDSHIRE DISTRICT 37 7.1 Surface Water Flood Risk 37 7.2 Surface Water Management 38 7.2.1 Canal Restoration 39 7.3 Recommendations 41 Southern Staffordshire SWMP Phase 1 9V5955/R00003/303671/Soli Final Report -i- July 2010 8 CANNOCK CHASE DISTRICT 43 8.1 Surface Water Flood Risk 43 8.2 Surface Water Management 44 8.2.1 Canal Restoration 45 8.3 Recommendations 47 9 SELECTION OF AN APPROACH FOR FURTHER ANALYSIS -
Yarnfield Park Location Map
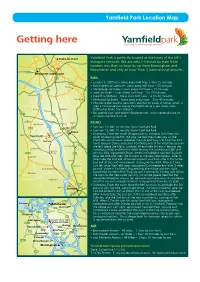
Yarnfield Park Location Map Getting here Yarnfieldpark training & conference centre Stoke-on-Trent Yarnfield Park is perfectly located at the heart of the UK’s transport network. We are only 1 ½ hours by train from London, less than an hour by car from Birmingham and Manchester and only an hour from 3 international airports. A525 Newcastle-under-Lyme A500 RAIL A50 • London to Stafford – trains every half hour – 1hrs 15 minutes Dresden • Birmingham to Stafford – trains every half hour – 30 minutes • Manchester to Stoke – trains every half hour – 35 minutes 15 A34 • Leeds to Stoke - trains every half hour – 1hr 45 minutes Hanchurch • Cardiff to Stafford – trains every half hour – 2 hrs 40 minutes Meir Heath • Edinburgh to Stoke – trains circa every hour – 3hrs 40 minutes • You can either catch a train from Stafford or Stoke to Stone, which is then a 10 minute taxi ride to Yarnfield Park or a taxi direct from Beech Barlaston Stafford or Stoke train stations. Tittensor • For specific train and ticket info please visit: www.nationalrail.co.uk A51 A34 or www.virgintrains.co.uk Cranberry A51 Oulton ROAD Swynnerton Meaford M6 • Junction 14, M6: 10 minutes from Yarnfield Park A519 A520 A34 • Junction 15, M6: 15 minutes from Yarnfield Park Lane Stone rnfield Ya • Directions: From the south (If approaching Yarnfield Park from the Millmeece Yarnfieldpark training & conference centre south on leaving the M6 J14 your Sat Nav may direct you up the Coldmeece Yarnfield A5013/Eccleshall Road. However the quickest way is to take the A34 A51 north towards Stone and enter Yarnfield Lane at the Wayfarer pub on Aston-by-Stone the left) Leave the M6 at Junction 14 and take 3rd exit if leaving the Sturbridge northbound M6 and the first exit if leaving the southbound M6 and Norton A519 Bridge A34 join the A34, signposted Stone. -

Mutual Exchange Register
Mutual Exchange Register Current Property Exchange Bedrooms Current Address Name Type Type Contact Details Required Bedrooms Preferred Areas UPIN Current Number of Bedrooms : 0 5 Collingwood Court, Lichfield Miss L BEDSIT BUNG/FLAT 07555294680 1/2 0 Brocton Road, Stone, Staffordshire, ST15 Whistance 8NB [email protected] Burton Manor Coton Fields Doxey Eccleshall Stafford Town Stone Town Walton Walton On The Hill Weston 69 Park Street, Uttoxeter, ST14 Miss Z Mason BEDSIT BUNG/FLAT 07866768058 1/2 0 Great Haywood 7AQ 07943894962 Highfields 07974618362 Newport [email protected] Rising Brook [email protected] Stafford Town 29 Graiseley Street, Miss D Toovey OTHER HSE 07549046902 2 0 Homcroft Wolverhampton, WV30PA [email protected] North End [email protected] Mutual Exchange Register Current Property Exchange Bedrooms Current Address Name Type Type Contact Details Required Bedrooms Preferred Areas CurrentUPIN Number of Bedrooms : 1 10 Hall Close, Silkmore, Stafford, Mrs K Brindle FLAT BUNG 07879849794 1 1 Barlaston Staffordshire, ST17 4JJ [email protected] Beaconside Rickerscote Silkmore Stafford Town Stone Town 10 Wayside, Pendeford, Mr P Arber FLAT BUNG/FLAT 07757498603 1 1 Highfields Wolverhampton , WV81TE 07813591519 Silkmore [email protected] 12 Lilac Grove, Chasetown, Mr C Jebson BUNG BUNG/FLAT [email protected] 1 1 Eccleshall Burntwood, WS7 4RW Gnosall Newport 12 Penkvale Road, Moss Pit, Mrs D Shutt FLAT BUNG 01785250473 1 1 Burton Manor Stafford, Staffordshire, ST17 -
High Speed Rail Phase 2A: Why the Current Proposals Are Bad for Staffordshire's Existing and Future Railway Links
High Speed Rail Phase 2a: Why the current proposals are bad for Staffordshire’s existing and future railway links Executive summary Staffordshire currently has very good train services to/from London via the West Coast Mainline (WCML) with travel times to London Euston station ranging from 77 minutes for Stafford and 85 minutes for Stoke on-Trent. The frequency of trains to/from London is also good. Stoke-on-Trent is provided with two trains per hour (tph) and Stafford at least 1tph in each direction according to the weekday timetable that operated prior to the Covid-19 outbreak. The current combined total of more than three exPress trains per hour to/from Staffordshire’s two main rail destinations will be dramatically reduced once the western arm of HS2 is fully oPerational. These services will be rePlaced by a single HS2 classic compatible express train per hour in each direction that will be shared between Stafford and Stoke-on-Trent and will terminate at Macclesfield, instead of at Manchester Piccadilly. The existing Pendolino services to Manchester and Liverpool will no longer run to avoid providing competition to HS2 services to the same destinations. HS2 services will be operated by the franchise holder of the West Coast services (currently Avanti) when HS2 oPens. It is very unlikely the operator will run express trains in competition with its flagship new service. Worryingly, even the token HS2 classic comPatible service is very vulnerable to being cut from the timetable before it starts to oPerate. This service was included in the original plan when HS2 schedules were based on the assumption that London Euston would have a capacity of 18tph. -
Digest No 265 of 6 March 2020
Members’ Digest ISSUE DATE CALL IN DATE NUMBER INDEX Page No Section 1 Cabinet Decisions 1.1 - 1.6 Section 2 Reports Supporting Cabinet Decisions 2.1 - 2.44 Section 3 Minutes of the Council 3.1 - 3.13 Section 4 Minutes of the Scrutiny Committees 4.1 - 4.8 Section 5 Minutes of the Regulatory and Joint Committees 5.1 - 5.9 Section 6 Corporate Information and Articles 6.1 - 6.20 SECTION ONE Cabinet Decisions Call-in Process Any Member of the Council may by notice in writing to the Head of Law and Administration request that a decision of the Cabinet be referred to the appropriate Scrutiny Committee. The reports supporting the decisions are reproduced in Section 2 and further information can be obtained from the Officer contact identified in the report. The notice must state the reason why the Member wishes the decision to be referred and must be received by the Head of Law and Administration by 5.00 pm on the last day of the call-in period - shown on the front cover of the Digest. If notices are received signed by one Member of the appropriate Scrutiny Committee and any two other Members, the decision will be referred to the Scrutiny Committee. It is, therefore, important that Members who wish to call in a decision should seek support from other appropriate Members. If you return the call-in response without securing support from other appropriate Members you risk there not being the necessary three signatures to support the call-in. If you cannot obtain the support of two other appropriate Members, you may still return the call-in request to register your concern/objection but this will not result in call in unless two other appropriate Members act independently of you on the same issue. -

North Housing Market Area Gypsy and Traveller Accommodation Needs Assessment : Final Report Brown, P, Scullion, LC and Niner, P
North housing market area Gypsy and Traveller accommodation needs assessment : Final report Brown, P, Scullion, LC and Niner, P Title North housing market area Gypsy and Traveller accommodation needs assessment : Final report Authors Brown, P, Scullion, LC and Niner, P Type Monograph URL This version is available at: http://usir.salford.ac.uk/id/eprint/35864/ Published Date 2007 USIR is a digital collection of the research output of the University of Salford. Where copyright permits, full text material held in the repository is made freely available online and can be read, downloaded and copied for non-commercial private study or research purposes. Please check the manuscript for any further copyright restrictions. For more information, including our policy and submission procedure, please contact the Repository Team at: [email protected]. North Housing Market Area Gypsy and Traveller Accommodation Needs Assessment Final report Philip Brown and Lisa Hunt Salford Housing & Urban Studies Unit University of Salford Pat Niner Centre for Urban and Regional Studies University of Birmingham December 2007 2 About the Authors Philip Brown and Lisa Hunt are Research Fellows in the Salford Housing & Urban Studies Unit (SHUSU) at the University of Salford. Pat Niner is a Senior Lecturer in the Centre for Urban and Regional Studies (CURS) at the University of Birmingham The Salford Housing & Urban Studies Unit is a dedicated multi-disciplinary research and consultancy unit providing a range of services relating to housing and urban management to public and private sector clients. The Unit brings together researchers drawn from a range of disciplines including: social policy, housing management, urban geography, environmental management, psychology, social care and social work. -

Superfast Staffordshire Live Cabinet List
SUPERFAST STAFFORDSHIRE LIVE CABINET LIST Cabinet Name Location District Parish S/O The Cash Store, Ashbrook East Staffordshire Abbots Bromley 2 Abbots Bromley Lane, Abbots Bromley Borough Council High St, O/S Sycamore House, East Staffordshire Abbots Bromley 3 Abbots Bromley Abbots Bromley Borough Council Tuppenhurst Lane, S/O 2 Lichfield District Armitage with Armitage 1 Proctor Road, Rugeley Council Handsacre S/O 73 Uttoxeter Road, Hill Lichfield District Armitage 3 Mavesyn Ridware Ridware, Rugeley Council Opp 65 Brook End, Longdon, Lichfield District Armitage 4 Longdon Rugeley Council Opp Rugeley Road, Armitage, Lichfield District Armitage with Armitage 5 Rugeley Council Handsacre Opp 31 Lichfield Road, Lichfield District Armitage with Armitage 6 Armitage, Rugeley Council Handsacre Lichfield District Armitage with Armitage 7 S/O 1 Station Dr Rugeley Council Handsacre Lichfield District Armitage with Armitage 8 S/O 6 Hood Lane Armitage Council Handsacre S/O 339 Ash Bank Road, Staffordshire Ash Bank 1 Werrington Washerwall Lane Moorlands District Staffordshire S/O 160 Ash Bank Road, New Ash Bank 2 Moorlands District Werrington Road Council Staffordshire S/O 1 Moss Park Ave, Stoke-on- Ash Bank 3 Moorlands District Werrington Trent Council Staffordshire S/O 425 Ash Bank Road, Ash Bank 5 Moorlands District Werrington Johnstone Avenue Council S/O 1 Chatsworth Drive, Salters Staffordshire Ash Bank 6 Werrington Lane Moorlands District S/O 1 Brookhouse Lane, Ash Bank 7 Werrington Road, Stoke On Stoke City Council Trent Staffordshire S/O 51 -

Trader Register Report
Trader Region: Added by Staffordshire & Stoke Partnership Company Name: Brooks Brothers Street Address: 8 Woodland Road, Rode Heath City / Town: Stoke on Trent Postcode: ST7 3TJ Company Website: Company Number: NA Distance from you: 0.00Miles Contact First Name: Nigel Brooks Contact Last Name: Neil Brooks Contact Telephone: 01270 883072 Contact Mobile: 07850 779722 Contact Email: [email protected] Contact Fax: Trader Region: Added by Staffordshire & Stoke Partnership Company Name: E J Leese Street Address: 19 Moreton Close, Kidsgrove City / Town: Stoke on Trent Postcode: ST7 4HP Company Website: http://n/a Company Number: Distance from you: 0.00Miles Contact First Name: Edward Contact Last Name: Leese Contact Telephone: 01782 775927 Contact Mobile: 07989105731 Contact Email: [email protected] Contact Fax: Trader Region: Added by Staffordshire & Stoke Partnership Company Name: Hibbitt Decorators Staffs Ltd Street Address: Boardmans Bank, Brown Edge City / Town: Stoke on Trent Postcode: ST6 8TE Company Website: http://wwwhibbittdecorators.co.uk Company Number: 8800881 Distance from you: 0.00Miles Contact First Name: Brian Contact Last Name: Hibbitt Contact Telephone: 01782 505550 Contact Mobile: 07957415049 Contact Email: [email protected] Contact Fax: Trader Region: Added by Staffordshire & Stoke Partnership Company Name: Stewarts Property Developments Street Address: 51 Spitfire Way, Tunstall City / Town: Staffordshire Postcode: ST6 5XQ Company Website: http://www.stewartspropertydevelopments.co.uk Company Number: Distance -
Statement of Persons Nominated and Notice of Poll
Stafford Borough Council Election of Member of Parliament for the Stone Constituency STATEMENT AS TO PERSONS NOMINATED AND NOTICE OF POLL Notice is hereby given that: 1. The following persons have been and stand validly nominated: SURNAME OTHER NAMES HOME ADDRESS DESCRIPTION (if any) NAMES OF THE PROPOSER (P), SECONDER (S) AND THE PERSONS WHO SIGNED THE NOMINATION PAPER Cash Bill The Tithe Barn, Upton The Conservative Party J H V Prendergast(P), S H Prendergast(S), J W Cressett, Bridgenorth, Candidate Farnham, C M Clark, R Harvey, A G James, R WV16 6UH P Barnard, J Barnard, P W Jones, R M Smith Hale Sam 21 Ayrshire Close, Labour and Co-operative H A C Main(P), Mary Lucy(S), T Laws, Nicholas Buckshaw Village, Party Hale, R Chidley, V M Chidley, F L Broadbent, Lancashire, PR7 7DA Alan Baker, J Palfreyman, J Palfreyman Lewis Martin Wyn 3 The Saplings, Clayton, Liberal Democrats D G Kirby(P), John Russell(S), Terence Morley, Newcastle, Staffs, ST5 Alex Sefton, N M Russell, P A Tweed, D P 4HW Tweed, Hazel Kirby, John Conchie, Barbara Conchie Pancheri Samantha Jay Stoke-on-Trent South The Green Party Karen Wilkes(P), S Wilkes(S), Richard Taylor, C Parliamentary A Forrester, S Blakeman, Lisa Smith, N W Constituency Frankish, L Griffin, R Krzysica, S McNicholas Whitfield Edward Henry Smiths Cottage, UK Independence Party D Scott(P), P H Green-Whitfield(S), P Scott, A R Wetwood, Stafford, (UKIP) Pace, M Pace, M E Jervis, B J R Letts, Anthea ST21 6NW Treanor, John Treanor, R H Beddall 2. -
![TRADE~. FAR 785 Shaw; John.A]Bert,Kingswood Common, Shuffiebotham Matthew, Lee .House, Slack Mrs](https://docslib.b-cdn.net/cover/5279/trade-far-785-shaw-john-a-bert-kingswood-common-shuffiebotham-matthew-lee-house-slack-mrs-1855279.webp)
TRADE~. FAR 785 Shaw; John.A]Bert,Kingswood Common, Shuffiebotham Matthew, Lee .House, Slack Mrs
Sl'AFFORDSHIRE.] TRADE~. FAR 785 Shaw; John.A]bert,Kingswood common, Shuffiebotham Matthew, Lee .house, Slack Mrs. William, Aver Hill side. A.lbrighton, Wolverhampton Rushton James, Macclesfield Lower Elkstone, Buxton Shaw Mrs. Mary~ Cheddleton, Leek Shuffiebotham Saml. Yarnfield, Ston~ Slack Wm. Wootton, Eccleshall,Stffrd $haw· R. Ma:rchingtou, Uttoxeter ShufHebotham William, . High lee, Slat~r Mrs. E. Fradley,A.lrewas,Burtn. Sha.w T. Ludg_ate st, Tutbury, Burtn Rushton James, Macclesfield Slater Mrs. Emma., Drayton Bassett,.. Shaw W. Burton st. Tutbury, Burton Shnker Waiter, Longnor hall, Penk- Tamworth Shaw W.jun. Old hall,Fradle-y ,Lichfid ridge, Stafford Slater G. Lightwood, Cheadle Grang~ Shaw Wm. Weston-on-Trent, Stafford Shuker William Edward, Wichnor Slater George, Milton, Stoke Shaw William Henry, Pershall green, bridges, Wichnor, Burton Slater J. The Mill,Marchington, Uttxtr Pershall, Eccleshall, Stafford Sidwells W. Clifton Campville,Tmwrth Slater John. Bentley, Walsall Sheldon John Prince J.P. Brund, Sigley Thos. Weston Coyney,Longton Slater J oseph. Tamhorn, Whitting-J Sheen. Buxton Silcock 'Mrs. Mary• Ann, Stubwood, ton, Lichfield Sheldon Thos. Walsall Wood, Walsall Rocester, Stafford Slater William, Fisherwick, Lichfield Shelley Willia~n; & Henry, Leawood Sillito Geor.ge, Gayton, Stafford Slater William Joseph, Marchington pits, High Offiey, Newport, Salop Sillito James, Bromley hall, Gerard's Woodlands, Uttoxeter ~helley Frederick William, Wetwood, Bromley, Eccleshall Sleath Rd. Church Eaton, Stafford Broughton, Ecclesball Sillito W. J.Greenfields,Bradly.Stffrd Sleigh Mrs. Jn. Barrow Moor, Heathy Shelleiy Henry, Beacon, Coton, Staffrd .Sillitc William, The Wellings, Ashley, Lee, Buxton Shelley James, Croxton, Stafford · Market Dra.yt-on SmallwOQd Leonard,Whitgreave,Stone Shelley John, Dilhorne, Stoke Sillitoe Frederick, Wootton, ;Eccles- Smallwood Wm. -

North Housing Market Area Gypsy and Traveller Accommodation Needs Assessment
North Housing Market Area Gypsy and Traveller Accommodation Needs Assessment Final report Philip Brown and Lisa Hunt Salford Housing & Urban Studies Unit University of Salford Pat Niner Centre for Urban and Regional Studies University of Birmingham December 2007 2 About the Authors Philip Brown and Lisa Hunt are Research Fellows in the Salford Housing & Urban Studies Unit (SHUSU) at the University of Salford. Pat Niner is a Senior Lecturer in the Centre for Urban and Regional Studies (CURS) at the University of Birmingham The Salford Housing & Urban Studies Unit is a dedicated multi-disciplinary research and consultancy unit providing a range of services relating to housing and urban management to public and private sector clients. The Unit brings together researchers drawn from a range of disciplines including: social policy, housing management, urban geography, environmental management, psychology, social care and social work. Study Team Core team members: Community Interviewers: Dr Philip Brown Sharon Finney Dr Lisa Hunt Tracey Finney Pat Niner Violet Frost Jenna Condie Joe Hurn Ann Smith Steering Group Karen Bates Staffordshire Moorlands District Council Abid Razaq Newcastle-under-Lyme Borough Council Philip Somerfield East Staffordshire Borough Council Eleanor Taylor Stoke-on-Trent City Council Stephen Ward Stafford Borough Council 3 4 Acknowledgements This study was greatly dependent upon the time, expertise and contributions of a number of individuals and organisations, without whom the study could not have been completed. Members of the project Steering Group provided guidance and assistance throughout the project and thanks must go to all of them for their support to the study team. Special thanks are also due to all those who took the time to participate in the study, helped organise the fieldwork and provided invaluable information and support in the production of this report. -

Appendix 1: Permitted and Operational Waste Management Facilities Within the Plan Area at March 2018 the First Review of the Waste Local Plan, December 2018
Appendix 1: Permitted and operational waste management facilities within the plan area at March 2018 The First Review of the Waste Local Plan, December 2018 Appendix 1: Permitted and operational waste management facilities within the plan area at March 2018 Measuring Waste Treatment Capacity Aggregate Recycling Facilities Landfill Sites Materials Recycling Facilities Organic Treatment Facilities Residual Treatment Facilities Waste Transfer Facilities 2 Appendix 1: Permitted and operational waste management facilities within the plan area at March 2018 The First Review of the Waste Local Plan, December 2018 Measuring Waste Treatment Capacity This Appendix provides a list of the 214 permitted and operational waste management facilities within the plan area as at end of March 2018. Capacity per waste management category has used a combination of actual capacity (Environment Agency Waste Data Interrogator 2017) and notional capacity (planning permissions up to 31 March 2018). There is no single measure of waste management capacity. It is often considered as either notional capacity or actual capacity. Notional capacity is the potential throughput which could be achieved if operations were to work to the maximum levels permitted in the planning permission or waste management licence or permit or exemption. Actual capacity is the quantity of waste which the facility manages i.e. the throughput /input recorded into the site, which tends to vary due to the market and other commercial factors. In assessing the existing waste infrastructure within the plan area, this Waste Local Plan review considered a combination of both notional capacity (when the planning permission for a site set out the maximum throughput by condition) and actual capacity (using the latest Environment Agency data on waste input into a site).