Open Door Laminoplasty: Creation of a New Vertebral Arch
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Modified Plate-Only Open-Door Laminoplasty Versus Laminectomy and Fusion for the Treatment of Cervical Stenotic Myelopathy
n Feature Article Modified Plate-only Open-door Laminoplasty Versus Laminectomy and Fusion for the Treatment of Cervical Stenotic Myelopathy LILI YANG, MD; YIFEI GU, MD; JUEQIAN SHI, MD; RUI GAO, MD; YANG LIU, MD; JUN LI, MD; WEN YUAN, MD, PHD abstract Full article available online at Healio.com/Orthopedics. Search: 20121217-23 The purpose of this study was to compare modified plate-only laminoplasty and lami- nectomy and fusion to confirm which of the 2 surgical modalities could achieve a better decompression outcome and whether a significant difference was found in postopera- tive complications. Clinical data were retrospectively reviewed for 141 patients with cervical stenotic myelopathy who underwent plate-only laminoplasty and laminectomy and fusion between November 2007 and June 2010. The extent of decompression was assessed by measuring the cross-sectional area of the dural sac and the distance of spinal cord drift at the 3 most narrowed levels on T2-weighted magnetic resonance imaging. Clinical outcomes and complications were also recorded and compared. Significant en- largement of the dural sac area and spinal cord drift was achieved and well maintained in both groups, but the extent of decompression was greater in patients who underwent Figure: T2-weighted magnetic resonance image laminectomy and fusion; however, a greater decompression did not seem to produce a showing the extent of decompression assessed by better clinical outcome. No significant difference was observed in Japanese Orthopaedic measuring the cross-sectional area of the dural sac Association and Nurick scores between the 2 groups. Patients who underwent plate-only (arrow). laminoplasty showed a better improvement in Neck Dysfunction Index and visual ana- log scale scores. -

Analysis of the Cervical Spine Alignment Following Laminoplasty and Laminectomy
Spinal Cord (1999) 37, 20± 24 ã 1999 International Medical Society of Paraplegia All rights reserved 1362 ± 4393/99 $12.00 http://www.stockton-press.co.uk/sc Analysis of the cervical spine alignment following laminoplasty and laminectomy Shunji Matsunaga1, Takashi Sakou1 and Kenji Nakanisi2 1Department of Orthopaedic Surgery, Faculty of Medicine, Kagoshima University; 2Department of Mechanical Engineering, Faculty of Engineering, Kagoshima University, Sakuragaoka, Kagoshima, Japan Very little detailed biomechanical examination of the alignment of the cervical spine following laminoplasty has been reported. We performed a comparative study regarding the buckling- type alignment that follows laminoplasty and laminectomy to know the mechanical changes in the alignment of the cervical spine. Lateral images of plain roentgenograms of the cervical spine were put into a computer and examined using a program we developed for analysis of the buckling-type alignment. Sixty-four patients who underwent laminoplasty and 37 patients who underwent laminectomy were reviewed retrospectively. The subjects comprised patients with cervical spondylotic myelopathy (CSM) and those with ossi®cation of the posterior longitudinal ligament (OPLL). The postoperative observation period was 6 years and 7 months on average after laminectomy, and 5 years and 6 months on average following laminoplasty. Development of the buckling-type alignment was found in 33% of patients following laminectomy and only 6% after laminoplasty. Development of buckling-type alignment following laminoplasty appeared markedly less than following laminectomy in both CSM and OPLL patients. These results favor laminoplasty over laminectomy from the aspect of mechanics. Keywords: laminoplasty; laminectomy; buckling; kyphosis; swan-neck deformity Introduction In 1930, Eiselberg1 reported a case of postoperative of postoperative abnormal alignment from the aspect kyphosis of the spine following laminectomy from the of the presence or absence of buckling-type alignment. -
Subtalar Joint Version 1.0 Effective June 15, 2021
CLINICAL GUIDELINES CMM-407: Arthroscopy: Subtalar Joint Version 1.0 Effective June 15, 2021 Clinical guidelines for medical necessity review of Comprehensive Musculoskeletal Management Services. © 2021 eviCore healthcare. All rights reserved. Comprehensive Musculoskeletal Management Guidelines V1.0 CMM-407: Arthroscopy: Subtalar Joint Definitions 3 General Guidelines 3 Indications 4 Non-Indications 5 Procedure (CPT®) Codes 5 References 6 ______________________________________________________________________________________________________ ©2021 eviCore healthcare. All Rights Reserved. Page 2 of 6 400 Buckwalter Place Boulevard, Bluffton, SC 29910 (800) 918-8924 www.eviCore.com Comprehensive Musculoskeletal Management Guidelines V1.0 Definitions Red flags indicate comorbidities that require urgent/emergent diagnostic imaging and/or referral for definitive therapy. Clinically meaningful improvement is defined as at least 50% improvement noted on global assessment. General Guidelines Either of the following are considered red flag conditions for subtalar joint arthroscopy: Post-reduction evaluation and management of the subtalar dislocation Septic arthritis in the subtalar joint Although imaging may be normal, prior to subtalar joint arthroscopy, radiographic imaging should be performed and include both of the following: Plain X-rays with one or more views (anteroposterior, lateral, axial, and/or Broden’s) to confirm and differentiate any of the following: Degenerative joint changes Loose bodies Osteochondral lesions Impingement -

In Patients with End-Stage Ankle Arthritis, How Does Total Ankle Arthroplasty Compared to Arthrodesis Affect Ankle Pain and Function?
University of the Pacific Scholarly Commons Physician's Assistant Program Capstones School of Health Sciences 4-1-2020 In Patients with End-Stage Ankle Arthritis, How Does Total Ankle Arthroplasty Compared to Arthrodesis Affect Ankle Pain and Function? Zachary Whipple University of the Pacific, [email protected] Follow this and additional works at: https://scholarlycommons.pacific.edu/pa-capstones Part of the Medicine and Health Sciences Commons Recommended Citation Whipple, Zachary, "In Patients with End-Stage Ankle Arthritis, How Does Total Ankle Arthroplasty Compared to Arthrodesis Affect Ankle Pain and Function?" (2020). Physician's Assistant Program Capstones. 84. https://scholarlycommons.pacific.edu/pa-capstones/84 This Capstone is brought to you for free and open access by the School of Health Sciences at Scholarly Commons. It has been accepted for inclusion in Physician's Assistant Program Capstones by an authorized administrator of Scholarly Commons. For more information, please contact [email protected]. In Patients with End-Stage Ankle Arthritis, How Does Total Ankle Arthroplasty Compared to Arthrodesis Affect Ankle Pain and Function? By Zachary Whipple Capstone Project Submitted to the Faculty of the Department of Physician Assistant Education of the University of the Pacific in partial fulfilment of the requirements for the degree of MASTER OF PHYSICIAN ASSISTANT STUDIES April 2020 Introduction End-stage ankle arthritis is a debilitating degenerative disease commonly located at the tibiotalar joint. The prevalence of symptomatic arthritis is about nine times lower than the rates associated with those of the knee or hip.1 Though less common than knee and hip arthritis, the US estimates greater than 50,000 new cases are reported each year.2 The most common etiology of ankle arthritis is post-traumatic pathology. -

Differences Between Subtotal Corpectomy and Laminoplasty for Cervical Spondylotic Myelopathy
Spinal Cord (2010) 48, 214–220 & 2010 International Spinal Cord Society All rights reserved 1362-4393/10 $32.00 www.nature.com/sc ORIGINAL ARTICLE Differences between subtotal corpectomy and laminoplasty for cervical spondylotic myelopathy S Shibuya1, S Komatsubara1, S Oka2, Y Kanda1, N Arima1 and T Yamamoto1 1Department of Orthopaedic Surgery, School of Medicine, Kagawa University, Kagawa, Japan and 2Oka Orthopaedic and Rehabilitation Clinic, Kagawa, Japan Objective: This study aimed to obtain guidelines for choosing between subtotal corpectomy (SC) and laminoplasty (LP) by analysing the surgical outcomes, radiological changes and problems associated with each surgical modality. Study Design: A retrospective analysis of two interventional case series. Setting: Department of Orthopaedic Surgery, Kagawa University, Japan. Methods: Subjects comprised 34 patients who underwent SC and 49 patients who underwent LP. SC was performed by high-speed drilling to remove vertebral bodies. Autologous strut bone grafting was used. LP was performed as an expansive open-door LP. The level of decompression was from C3 to C7. Clinical evaluations included recovery rate (RR), frequency of C5 root palsy after surgery, re-operation and axial pain. Radiographic assessments included sagittal cervical alignment and bone union. Results: Comparisons between the two groups showed no significant differences in age at surgery, preoperative factors, RR and frequency of C5 palsy. Progression of kyphotic changes, operation time and volumes of blood loss and blood transfusion were significantly greater in the SC (two- or three- level) group. Six patients in the SC group required additional surgery because of pseudoarthrosis, and four patients underwent re-operation because of adjacent level disc degeneration. -

Procedure Coding in ICD-9-CM and ICD- 10-PCS
Procedure Coding in ICD-9-CM and ICD- 10-PCS ICD-9-CM Volume 3 Procedures are classified in volume 3 of ICD-9-CM, and this section includes both an Alphabetic Index and a Tabular List. This volume follows the same format, organization and conventions as the classification of diseases in volumes 1 and 2. ICD-10-PCS ICD-10-PCS will replace volume 3 of ICD-9-CM. Unlike ICD-10-CM for diagnoses, which is similar in structure and format as the ICD-9-CM volumes 1 and 2, ICD-10-PCS is a completely different system. ICD-10-PCS has a multiaxial seven-character alphanumeric code structure providing unique codes for procedures. The table below gives a brief side-by-side comparison of ICD-9-CM and ICD-10-PCS. ICD-9-CM Volume3 ICD-10-PCS Follows ICD structure (designed for diagnosis Designed and developed to meet healthcare coding) needs for a procedure code system Codes available as a fixed or finite set in list form Codes constructed from flexible code components (values) using tables Codes are numeric Codes are alphanumeric Codes are 3-4 digits long All codes are seven characters long ICD-9-CM and ICD-10-PCS are used to code only hospital inpatient procedures. Hospital outpatient departments, other ambulatory facilities, and physician practices are required to use CPT and HCPCS to report procedures. ICD-9-CM Conventions in Volume 3 Code Also In volume 3, the phrase “code also” is a reminder to code additional procedures only when they have actually been performed. -

Knee Arthrodesis After Failed Total Knee Arthroplasty
650 COPYRIGHT Ó 2019 BY THE JOURNAL OF BONE AND JOINT SURGERY,INCORPORATED Current Concepts Review Knee Arthrodesis After Failed Total 04/12/2019 on 1mhtSo9F6TkBmpGAR5GLp6FT3v73JgoS8Zn360/N4fAEQXu6c15Knc+cXP2J5+wvbQY2nVcoOF2DIk3Zd0BSqmOXRD8WUDFCPOJ9CnEHMNOmtIbs3S0ykA== by http://journals.lww.com/jbjsjournal from Downloaded Knee Arthroplasty Downloaded Asim M. Makhdom, MD, MSc, FRCSC, Austin Fragomen, MD, and S. Robert Rozbruch, MD from http://journals.lww.com/jbjsjournal Investigation performed at the Hospital for Special Surgery, Weill Cornell Medicine, Cornell University, New York, NY ä Knee arthrodesis after failure of a total knee arthroplasty (TKA) because of periprosthetic joint infection (PJI) may provide superior functional outcome and ambulatory status compared with above-the-knee amputation. by 1mhtSo9F6TkBmpGAR5GLp6FT3v73JgoS8Zn360/N4fAEQXu6c15Knc+cXP2J5+wvbQY2nVcoOF2DIk3Zd0BSqmOXRD8WUDFCPOJ9CnEHMNOmtIbs3S0ykA== ä The use of an intramedullary nail (IMN) for knee arthrodesis following removal of TKA components because of a PJI may result in higher fusion rates compared with external fixation devices. ä The emerging role of the antibiotic cement-coated interlocking IMN may expand the indications to achieve knee fusion in a single-stage intervention. ä Massive bone defects after failure of an infected TKA can be managed with various surgical strategies in a single- stage intervention to preserve leg length and function. Primary total knee arthroplasty (TKA) is a common procedure suppressive antibiotics for recurrent PJIs are generally reserved with a reported increase of 162% from 1991 to 2010 in the for patients with more severe preoperative disability and United States1,2. From 2005 to 2030, it is projected that the medical comorbidity and those who are not candidates to number of TKA procedures will grow by 673% or 3.5 million. -

Foot and Ankle Systems Coding Reference Guide
Foot and Ankle Systems Coding Reference Guide Physician CPT® Code Description Arthrodesis 27870 Arthrodesis, ankle, open 27871 Arthrodesis, tibiofibular joint, proximal or distal 28705 Arthrodesis; pantalar 28715 Arthrodesis; triple 28725 Arthrodesis; subtalar 28730 Arthrodesis, midtarsal or tarsometatarsal, multiple or transverse 28735 Arthrodesis, midtarsal or tarsometatarsal, multiple or transverse; with osteotomy (eg, flatfoot correction) 28737 Arthrodesis, with tendon lengthening and advancement, midtarsal, tarsal navicular-cuneiform (eg, miller type procedure) 28740 Arthrodesis, midtarsal or tarsometatarsal, single joint 28750 Arthrodesis, great toe; metatarsophalangeal joint 28755 Arthrodesis, great toe; interphalangeal joint 28760 Arthrodesis, with extensor hallucis longus transfer to first metatarsal neck, great toe, interphalangeal joint (eg, jones type procedure) Bunionectomy 28292 Correction, hallux valgus (bunionectomy), with sesamoidectomy, when performed; with resection of proximal phalanx base, when performed, any method 28295 Correction, hallux valgus (bunionectomy), with sesamoidectomy, when performed; with proximal metatarsal osteotomy, any method 28296 Correction, hallux valgus (bunionectomy), with sesamoidectomy, when performed; with distal metatarsal osteotomy, any method 28297 Correction, hallux valgus (bunionectomy), with sesamoidectomy, when performed; with first metatarsal and medial cuneiform joint arthrodesis, any method 28298 Correction, hallux valgus (bunionectomy), with sesamoidectomy, when performed; with -

Biomechanical Analysis of Posterior Ligaments of Cervical Spine and Laminoplasty
applied sciences Article Biomechanical Analysis of Posterior Ligaments of Cervical Spine and Laminoplasty Norihiro Nishida 1 , Muzammil Mumtaz 2, Sudharshan Tripathi 2, Amey Kelkar 2, Takashi Sakai 1 and Vijay K. Goel 2,* 1 Department of Orthopedic Surgery, Yamaguchi University Graduate School of Medicine, 1-1-1 Minami-Kogushi, Ube, Yamaguchi Prefecture 755-8505, Japan; [email protected] (N.N.); [email protected] (T.S.) 2 Engineering Center for Orthopaedic Research Excellence (E-CORE), Departments of Bioengineering and Orthopaedics, The University of Toledo, Toledo, OH 43606, USA; [email protected] (M.M.); [email protected] (S.T.); [email protected] (A.K.) * Correspondence: [email protected]; Tel.: +1-(419)-530-8035 Abstract: Cervical laminoplasty is a valuable procedure for myelopathy but it is associated with complications such as increased kyphosis. The effect of ligament damage during cervical lamino- plasty on biomechanics is not well understood. We developed the C2–C7 cervical spine finite element model and simulated C3–C6 double-door laminoplasty. Three models were created (a) in- tact, (b) laminoplasty-pre (model assuming that the ligamentum flavum (LF) between C3–C6 was preserved during surgery), and (c) laminoplasty-res (model assuming that the LF between C3–C6 was resected during surgery). The models were subjected to physiological loading, and the range of motion (ROM), intervertebral nucleus stress, and facet contact forces were analyzed under flex- ion/extension, lateral bending, and axial rotation. The maximum change in ROM was observed Citation: Nishida, N.; Mumtaz, M.; under flexion motion. Under flexion, ROM in the laminoplasty-pre model increased by 100.2%, Tripathi, S.; Kelkar, A.; Sakai, T.; Goel, 111.8%, and 98.6% compared to the intact model at C3–C4, C4–C5, and C5–C6, respectively. -
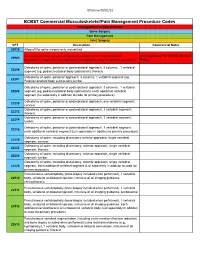
Commercial MSK Procedure Code List Effective 09.01.21.Xlsx
Effective 09/01/21 BCBST Commercial Musculoskeletal/Pain Management Procedure Codes Investigational or Non-Covered Spine Surgery Pain Management Joint Surgery CPT Description Commercial Notes 20930 Allograft for spine surgery only morselized Computer-assisted surgical navigational procedure for musculoskeletal Investigational Per BCBST Medical 20985 procedures, image-less (List separately in addition to code for primary procedure) Policy Osteotomy of spine, posterior or posterolateral approach, 3 columns, 1 vertebral 22206 segment (eg, pedicle/vertebral body subtraction); thoracic Osteotomy of spine, posterior approach, 3 columns, 1 vertebral segment (eg. 22207 Pedicle/vertebral body subtraction);lumbar Osteotomy of spine, posterior or posterolateral approach, 3 columns, 1 vertebral 22208 segment (eg, pedicle/vertebral body subtraction); each additional vertebral segment (list separately in addition to code for primary procedure) Osteotomy of spine, posterior or posterolateral approach, one vertebral segment; 22210 cervical Osteotomy of spine, posterior or posterolateral approach, 1 vertebral segment; 22212 thoracic Osteotomy of spine, posterior or posterolateral approach, 1 vertebral segment; 22214 lumbar Osteotomy of spine, posterior or posterolateral approach, 1 vertebral segment; 22216 each additional vertebral segment (List separately in addition to primary procedure) Osteotomy of spine, including discectomy anterior approach, single vertebral 22220 segment; cervical Osteotomy of spine, including discectomy, anterior approach, single -

USE of INTERPOSITIONAL BONE GRAFTS for FIRST METARSOPHALANGEAL ARTHRODESIS: a Review of Current Literature
CHAPTER 8 USE OF INTERPOSITIONAL BONE GRAFTS FOR FIRST METARSOPHALANGEAL ARTHRODESIS: A Review of Current Literature Thomas A. Brosky, II, DPM Cayla Conway, DPM INTRODUCTION incidence of nonunion with the use of autogenic iliac crest graft (26.7%) compared to the allograft (0%). Surgical procedures for fi rst metarsophalangeal joint (MPJ) In contrast to the Myerson study, Mankovecky et al arthritis have been well outlined in podiatric literature. (2) suggested a much lower rate of nonunion with the use The fi rst MPJ fusion is a procedure that is commonly autogenous bone graft. In 2013, they reported a review of 6 used for initial treatment of this condition or subsequent studies, which reported a total of 42 procedures of fi rst MPJ treatment, after another surgical procedure has failed. A arthrodesis with autogenous graft as a salvage procedure for failed arthroplasty may result in an excessively shortened a failed Keller arthroplasty. Out of the 42 cases, there were fi rst metatarsal or an overly resected proximal phalanx, 2 reported nonunions for a nonunion rate of 4.8%, which which may necessitate the use of an interpositional bone- is signifi cantly less than the rate reported by Myerson. One block graft to restore adequate length. The preservation of of the nonunions was revised, and the other was reported length can pose a surgical challenge, however, it is integral as asymptomatic. The review states the cases were highly in preventing complications that may result from altered varied in technique and fi xation approach. Mankovecky et al biomechanics, such as inadequate propulsion and lesser reported a need for further research to standardize the data metatarsalgia. -

Cervical Laminoplasty - Principles, Surgical Methods, Results, and Issues
Open Access Austin Journal of Surgery Special Article – Cervical Surgery Cervical Laminoplasty - Principles, Surgical Methods, Results, and Issues Hirabayashi S*, Kitagawa T and Kawano H Department of Orthopaedic Surgery, Teikyo University Abstract Hospital, Japan Cervical laminoplasty (CL) is one of the surgical methods via posterior *Corresponding author: Hirabayashi S, Department approach for treating patients with cervical myelopathy. The main purpose of of Orthopaedic Surgery, Teikyo University Hospital, CL is to decompress the cervical spinal cord by widening the narrowed spinal Japan canal, combined with preserving the posterior anatomical structures to the degree possible. At present, these surgical methods are broadly divided into Received: November 23, 2017; Accepted: December two types from the viewpoints of the site of osteotomy: Double-door type 12, 2017; Published: December 19, 2017 (DDL) and Open-door type (ODL). Various materials are used to maintain the enlarged spinal canal such as autogeneous bone (spinous process, iliac bone), hydroxyapatite spacer, titanium plate and screw, thread, and so on. Although the surgical methods and techniques of CL and the methods of assessment are various, recovery rates have been reported to be about 60~70%. The main influential factors on the surgical results are the age of the patients, the duration of the diseases, accompanying injuries to the cervical spine, and the neurological findings just before surgery. CL can be safely performed and stable surgical results maintained for a long period; more than 10 years. However, patients with large prominence-type of ossification of the posterior longitudinal ligament (OPLL) and severe kyphotic alignment of the cervical spine are relatively contraindicated because of possibility of inadequate posterior shift of the spinal cord.