"Understanding Gloucestershire
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

4542 the London Gazette, 21 August, 1953
4542 THE LONDON GAZETTE, 21 AUGUST, 1953 Railway Line by way of an overhead reinforced Standish—Hope Cottage, Gloucester Road, Stone- concrete footbridge with approaches. house. A certified copy of the Order and of the map con- Tirley—Torsend Cottage, Tirley. tained in the Order as confirmed by the Minister has Twigworth—c/o Mr. E. J. Jones, Far End, Twig- been deposited at the Council Offices, Argyle Road* worth. Sevenoaks, and will be open for inspection free of Upton St. Leonards—'Village Hall, Upton St. charge between the hours of 9 a.m. and 5.30 p.m. on Leonards. Weekdays and between 9 a.m. and 12 noon on Westbury-on-Severn—Lecture Hall, Westbury-on- Saturday. Severn. The Order becomes operative as from 'the 21st Whitminster—c/o iMr. A. E. Wyer, The Garage, day of August, 1953, but if any person aggrieved Whitminster. by the Order desires to question the validity thereof In exceptional circumstances special arrangements or of any provision contained therein on the grounds will be made for the draft map and statement to be that it is not within the powers of the National Parks inspected out of office hours. and Access to the Countryside Act, 1949, or on the Any objection or representation with respect to ground -that any requirement of the Act or any the draft map or statement may be sent in writ- regulation made thereunder has not been complied ing to the undersigned before the 30th day of April, with in relation to the approval of the Order he 1954, and any such objection or representation should may. -

Mark Chadwick Hunter Page Planning 18 High Street Cheltenham Gloucestershire GL50 1DZ Our Ref: APP/G1630/V/14/2229497 31 March
Mark Chadwick Our Ref: APP/G1630/V/14/2229497 Hunter Page Planning 18 High Street Cheltenham Gloucestershire GL50 1DZ 31 March 2016 Dear Sir TOWN AND COUNTRY PLANNING ACT 1990 – SECTION 77 APPLICATION BY ERLP AND THE MERCHANT VENTURERS LAND AT ‘PERRYBROOK’ TO THE NORTH OF BROCKWORTH AND SOUTH OF THE A417, BROCKWORTH, GLOUCESTERSHIRE APPLICATION REF: 12/01256/OUT 1. I am directed by the Secretary of State to say that consideration has been given to the report of the Inspector, Mrs KA Ellison BA, MPhil, MRTPI, who held a inquiry from 28-30 July 2015 into your client’s application to Tewkesbury Borough Council (‘the Council’) for outline planning permission for the mixed use development of up to 1,500 dwellings including extra care housing, community facilities including Al, A2, A3, A4 and A5 local retail shops, B1 /B8 employment uses, D1 health facilities and formal/informal public open space, in accordance with application ref 12/01256/OUT, dated 5 December 2012. 2. On 24 November 2014, the Secretary of State directed, in pursuance of Section 77 of the Town and Country Planning Act 1990, that your client’s application be referred to him instead of being dealt with by the local planning authority, Tewkesbury Borough Council, after consideration of policy on calling-in applications. Inspector’s recommendation and summary of the decision 3. The Inspector recommended that the application be approved and planning permission granted. For the reasons given below, the Secretary of State agrees with the Inspector’s recommendation. A copy of the Inspector’s report (IR) is enclosed. -
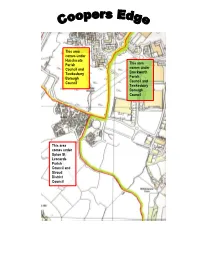
Coopers Edge Boundary Information
This area comes under Hucclecote Parish This area Council and comes under Tewkesbury Brockworth Borough Parish Council Council and Tewkesbury Borough Council This area comes under Upton St Leonards Parish Council and Stroud District Council The Coopers Edge development is shared between 3 parish councils and 2 district councils. The map above shows how the parish boundaries intersect through the development, and 2 of the parishes fall into the Tewkesbury Borough Council authority, and 1 parish falls into Stroud District Council authority. Your parish council is responsible for things like parks and play areas, burial grounds, community facilities, allotments and comments on planning applications and is consulted on policies that the Borough and County Councils implement. The district or borough councils deal with things like bins, planning, benefits and much more. Gloucestershire County Council covers the whole of Coopers Edge and they are responsible for roads, transport, public rights of way, education, and so on. Contacts: Brockworth Parish Council Community Centre Tewkesbury Borough Council Court Road Council Offices Brockworth Gloucester Road Gloucester GL3 4ET Tewkesbury GL20 5TT Email: [email protected] Website: www.brockworth-pc.gov.uk Tel: 01684 295010 Tel: 01452 863123 Website: www.tewkesbury.gov.uk Hucclecote Parish Council Stroud District Council Pineholt Village Hall, Bird Road, Ebley Mill Hucclecote Stroud GL3 3SN GL5 4UB Website: www.hucclecotepc.gov.uk Tel: 01453 766321 Tel: 01452 612485 Website: www.stroud.gov.uk Upton St Leonards Parish Council 11 Broadstone Close Barnwood Gloucester GL4 3TX Email: [email protected] Website: www.uptonstleonards-pc.gov.uk Tel: 01452 621688 . -
Understanding Gloucester 2015
Understanding Gloucester 2015 Produced by the Strategic Needs Analysis Team, Gloucestershire County Council Version: v1.0 Contents 1. Introduction ................................................................................................................ 3 2. Executive summary .................................................................................................... 4 3. Gloucester context ................................................................................................... 13 3.1 About this section ................................................................................................. 13 3.2 Demographics ....................................................................................................... 13 3.3 Deprivation ........................................................................................................... 19 3.4 Life expectancy ..................................................................................................... 26 3.5 Mortality ................................................................................................................ 28 3.6 Economy ............................................................................................................... 31 3.7 Protected characteristics ....................................................................................... 50 3.8 Key messages ...................................................................................................... 57 4. Getting the right start in life ...................................................................................... -

233 08 SD50 Environment Permitting Decision Document
Environment Agency permitting decisions Variation We have decided to issue the variation for Middle Pig Farm, Court Farm and Bentham Farm operated by Alexander and Angell (Farms) Limited. The variation number is EPR/VP3834UB/V004. We consider in reaching that decision we have taken into account all relevant considerations and legal requirements and that the permit will ensure that the appropriate level of environmental protection is provided. Description of the changes introduced by the Variation This is a Substantial Variation. This variation authorises the following changes: • Increase in the number of sow places from 400 to 528. The existing sheds are to be better utilised in order to accommodate this increase. Table S1.1 in the permit has been updated to reflect this change. • Increase in the number of broiler breeder layer places on Court Farm from 29,700 to 36,790. Table S1.1 in the permit has been updated to reflect this change. • Poultry houses BT1, BT2, BT3 and BT4 are to be knocked down and replaced with poultry houses CF5 and CF10 to accommodate the increase in bird numbers on Court Farm. The two new sheds are to be ventilated using side ventilation. A revised site layout and drainage plan has been submitted as part of this application which have been incorporated into the operating techniques. • Extend the installation boundary in order to accommodate poultry houses CF5 and CF10. A revised installation boundary plan has been submitted which has been included in Schedule 7 of this permit. • The previous variation (EPR/VP3834UB/V003) included the rearing of 1810 pigs from birth up to 30kg as a Directly Associated Activity (DAA). -

King's Stanley
66 Stonehouse - Leonard Stanley - King’s Stanley - Stroud - Painswick - Cheltenham Stagecoach West Timetable valid from 04/08/2019 until further notice. Direction of stops: where shown (eg: W-bound) this is the compass direction towards which the bus is pointing when it stops Mondays to Fridays Service Restrictions SH Sch Sch Notes Stonehouse, after Sherborne Close 1502 § Stonehouse, opp Maidenhill School 1504 § Stonehouse, before Gloucester Road 1505 § Stonehouse, by The Nippy Chippy 1507 Stonehouse, o/s Medical Centre 1510 § Stonehouse, opp Elgin Mall 1510 § Stonehouse, corner of Pearcroft Road 1511 § Stonehouse, by Downton Road 1513 Bridgend, opp Haven Avenue 1514 § Bridgend, opp Crescent Road 1514 § Stanley Downton, nr The Old Fleece 1516 § Leonard Stanley, opp Garage 1518 § Leonard Stanley, nr Bath Road 1519 Leonard Stanley, opp Village Hall 1520 § Leonard Stanley, opp St Swithun’s Church 1521 § Leonard Stanley, opp Wesley Road 1521 § Leonard Stanley, opp Church Road 1521 § Leonard Stanley, by Grange Farm 1522 § Leonard Stanley, before Primary School 1524 § King’s Stanley, before Bathleaze 1524 § King’s Stanley, by High Street South 1525 King’s Stanley, opp King’s Head 1526 § King’s Stanley, before Shute Street 1526 § Middleyard, after Coldwell 1528 § Middleyard, before Coombe Lane 1528 § Selsley, by The Knapp 1529 § Selsley, opp Westville 1531 § Selsley, o/s All Saint’s Church 1531 § Selsley, before New Road 1532 § Selsley, by Cricket Ground 1533 Dudbridge, by Dudbridge Hill Roundabout 1535 § Cainscross, before Marling School 1537 -

Horsbere Brook Barnwood Gloucester Gloucestershire
HORSBERE BROOK BARNWOOD GLOUCESTER GLOUCESTERSHIRE ARCHAEOLOGICAL EVALUATION For ENVIRONMENT AGENCY CA PROJECT: 3064 CA REPORT: 10035 MARCH 2010 1 HORSBERE BROOK BARNWOOD GLOUCESTER GLOUCESTERSHIRE ARCHAEOLOGICAL EVALUATION CA PROJECT: 3064 CA REPORT: 10035 prepared by Steven Sheldon, Project Supervisor date 05 March 2010 checked by Cliff Bateman, Project Manager date 11 March 2010 approved by Simon Cox, Head of Fieldwork signed date 16 March 2010 issue 01 This report is confidential to the client. Cotswold Archaeology accepts no responsibility or liability to any third party to whom this report, or any part of it, is made known. Any such party relies upon this report entirely at their own risk. No part of this report may be reproduced by any means without permission. © Cotswold Archaeology Building 11, Kemble Enterprise Park, Kemble, Cirencester, Gloucestershire, GL7 6BQ Tel. 01285 771022 Fax. 01285 771033 E-mail: [email protected] © Cotswold Archaeology Horsbere Brook, Barnwood, Gloucester, Gloucestershire: Archaeological Evaluation CONTENTS SUMMARY........................................................................................................................2 1. INTRODUCTION ................................................................................................. 3 2. RESULTS (FIG 2)................................................................................................ 5 3. DISCUSSION....................................................................................................... 6 4. CA PROJECT -
Initial Document Template
TEWKESBURY BOROUGH COUNCIL – DEVELOPMENT MANAGEMENT Committee: Planning Date: 22 June 2021 Site Location: Land North Of Perrybrook Shurdington Road Brockworth Gloucester Gloucestershire Application No: 20/00608/FUL Ward: Brockworth East Parish: Brockworth Proposal: The erection of 47 dwellings and associated vehicular access, public open space, landscaping and other associated infrastructure. Report by: Victoria Stone Appendices: Site Location Plan Site Layout Plan Street Scene plan Elevations & Floor Plans – Bibury & Cowley House Types Elevations & Floor Plans – Chester & Bibury House Types Elevations & Floor Plans – Beckford & Cantlow House Types Elevations & Floor Plans – Beckford & Chedworth House Types Elevations & Floor Plans – Ashton & Barrow Apartments Elevations & Floor Plans – Cranham House Type Elevations & Floor Plans – Dereham House Type Elevations & Floor Plans – Derwent House Type Elevations & Floor Plans – Dursley House Type Elevations & Floor Plans – Proposed Garages Perrybrook Masterplan Context and Green Infrastructure Plan Strategic Allocation North Brockworth Indicative Site Layout Plan Perrybrook Conceptual Masterplan Recommendation: Delegated Permit 1.0 SITE DESCRIPTION AND PROPOSAL 1.1. This application relates to a parcel of land located along the A46 Shurdington Road in Brockworth (see attached location plan). 1.2. The site comprises an area of arable farmland covering approximately 2.3 hectares. The site generally falls in an easterly direction from a high point located in the west of the site. Levels range from 76.06m AOD at the high point in the west to 71.27m AOD in the northeast of the site. The site is bound by existing vegetation on all sides, although there are some gaps within the hedgerow that defines the boundary with the A46 road corridor which allows some views into and out of the site. -

Gloucestershire Aircraft Accidents
Gloucestershire Aircraft Accidents Date Mark Details 16.03.17 A3311 Bristol Fighter, 38 TS, Stalled on approach, Rendcomb 03.06.17 A465 Avro 504A, 38 TS, Spun in, Rendcomb 16.06.17 A5911 Avro 504A, 38 TS, Spun on final turn, Rendcomb 26.06.17 5876 B.E.2d, 62 Sqn, , 05.07.17 A3484 R.E.8, 38 TS, Crashed, Rendcomb 11.07.17 A3310 Bristol Fighter, 38 TS, Crashed, North Cerney 10.08.17 A4694 R.E.8, 62 Sqn, , 16.08.17 B741 R.E.8, 62 Sqn, Spun in, near Rendcomb 22.08.17 A3177 R.E.8, 38 TS, , 30.08.17 A3319 Bristol Fighter, 38 TS, Caught fire and crashed into buildings, Rendcomb 10.11.17 A3328 Bristol Fighter, 38 TS, Crashed on approach, Rendcomb 05.12.17 A7197 Bristol Fighter, 62 Sqn, Stalled & crashed, near Rendcomb 11.01.18 C4610 Bristol Fighter, 62 Sqn, Caught fire on landing, Rendcomb Apr.-18 ? ? AFC, Crashed, Leighterton 04.04.18 B9248 Camel, 6 Sqn AFC, Crashed doing low aerobatics, Minchinhampton 08.04.18 C9345 D.H.6, 59 Sqn, Crashed & burned, Rendcomb 09.04.18 ? ?, AFC, Veered on take-off; hit fence & spectators, near Hill Farm, Holcombe, Painswick 23.04.18 B4228 Avro 504J, CFS, Crashed after midair collision, Overbury Park, near Cirencester 23.04.18 B6176 B.E.2e, 7 Sqn AFC, Crashed, Leighterton 01.05.18 4593 B.E.2e, 24 TS, Hit tree on take-off, Broad Marston 03.05.18 B1845 Pup, CFS, Spun off loop, Rendcomb 21.06.18 C103 Sopwith Camel, 5 Sqn AFC, Accident, 03.07.18 E140 R.E.8, 8 Sqn AFC, Aeroplane accident, Leighterton 07.07.18 D1513 R.E.8, 7 Sqn AFC, Aeroplane accident, 16.07.18 B1259 Bristol Fighter, 45 TDS, , 10.08.18 C6915 B.E.2e, -

Gloucestershire Folk Song
Glos.Broadsht.7_Layout 1 15/10/2010 14:35 Page 1 1 4 A R iver Avon A4104 A3 8 9 Randwick cheese rolling and Randwick Wap Dover’s Games and Scuttlebrook Wake, Chipping 2 A about!’ and they routed the 8 Chipping 4 A JANUARY 4 A 43 First Sunday and second Saturday in May Campden – Friday and Saturday after Spring Bank 1 4 Camden French in hand-to-hand 4 Blow well and bud well and bear well Randwick is one Holiday 5 0 fighting. For this feat the 1 8 God send you fare well A3 Gloucestershires were of the two places The ‘Cotswold Olimpicks’ or ‘Cotswold Games’ were A43 A 8 3 Every sprig and every spray in Gloucestershire instituted around 1612 by Robert Dover. They mixed 8 allowed to wear two hat or A bushel of apples to be that still practices traditional games such as backsword fighting and cap badges – the only 2 9 given away cheese-rolling. On shin-kicking with field sports and contests in music 4 10 MORETON- regiment to do so. The Back Dymock A 1 IN-MARSH On New Year’s day in the TEWKESBURY 4 Badge carries an image of the first Sunday in A n 3 Wo olstone 4 morning r 5 A the Sphinx and the word May cheeses are e 1 2 4 ev 4 4 M50 8 S ‘Egypt’. The Regiment is now From dawn on New Year’s Day, rolled three times r 3 Gotherington e A 5 A v i part of The Rifles. -

Air Cover on D-Day • Lithgow in Libya Jet Fighters of the Second World War Major Dixon's Diary • Trouble at Thorney
Air Cover on D-Day • Lithgow in Libya Jet Fighters of the Second World War Major Dixon’s Diary • Trouble at Thorney Tangmere Military Aviation Museum Trust Company Limited Patron: The Duke of Richmond and Gordon Hon. President: Air Marshal Sir Dusty Miller, KBE Hon. Life Vice-President: Alan Bower Hon. Life Vice-President: Duncan Simpson, OBE Council of Trustees Chairman: Group Captain David Baron, OBE David Burleigh, MBE Reginald Byron David Coxon Dudley Hooley Ken Shepherd Phil Stokes Joyce Warren Officers of the Company Hon. Treasurer: Ken Shepherd Hon. Secretary: Joyce Warren Management Team Director: Dudley Hooley Curator: David Coxon General Manager and Chief Engineer: Phil Stokes Events Manager: David Burleigh, MBE Publicity Manager: Cherry Greveson Staffing Manager: Mike Wieland Treasurer: Ken Shepherd Shop Manager: Sheila Shepherd Registered in England and Wales as a Charity Charity Commission Registration Number 299327 Registered Office: Tangmere, near Chichester, West Sussex PO20 2ES, England Telephone: 01243 790090 Fax: 01243 789490 Website: www.tangmere-museum.org.uk E-mail: [email protected] 2 . from Charles Dixon’s Diary 4 A personal record of life on the Western Front in 1917-18 David Coxon Jet Fighters of the Second World War, Part 1 7 Meteors, Me262s, Shooting Stars, and their precursors Matt Wright The Swift Souvenir Book 18 Photographs of the successful air speed record attempt in Libya, 1953 Courtesy of Les Cobbett Tangmere and Operation Neptune 24 The air cover plan for D-Day, and Tangmere’s part in it Andrew Smith Letters, Notes, and Queries 29 The Hunter that wouldn’t land, and Over the Andes Published by the Society of Friends of the Tangmere Military Aviation Museum, Tangmere, near Chichester, West Sussex PO20 2ES, England Edited by Dr Reginald Byron, who may be contacted care of the Museum at the postal address given above, or by e-mail at [email protected] Copyright © 2014 by the Tangmere Military Aviation Museum Trust Company All rights reserved. -

12 Pound Farm Courtyard, Brockworth , Gloucester, GL3 4EA Two Double Bedrooms Garden Two Parking Spaces Ensuite and Family Bathroom Corner Plot Local Amenities
12 Pound Farm Courtyard, Brockworth , Gloucester, GL3 4EA Two double bedrooms Garden Two parking spaces Ensuite and family bathroom Corner plot Local amenities Approximately 655 sq ft Price Guide: £185,000 ‘A well presented two bedroom home situated within a small cul-de-sac in Brockworth convenient to an array of local amenities.’ The Property Situation Directions This excellent modern home is situated Known locally for its annual cheese rolling From junction 11A of the M5, take the within a small cul-de-sac in Brockworth contest down Cooper's Hill, Brockworth is A417 towards Ullenwood for 2 miles. At convenient to an array of local amenities. a district of Gloucester located within easy the roundabout, take the thrid exit on the The property is beautifully presented distance of the M5 with Gloucester 4 miles A46 towards Stroud. At the next throughout with benefits including gas away and Cheltenham only 5 miles. These roundabout, take the third exit onto Ermin fired central heating and double glazing. towns offer an array of independent and Street and take the second left onto Green high street shops and restaurants. Street. Then take the first left onto Pound An entrance hall with WC off leads Farm Courtyard and locate the property in through to a fitted kitchen with rear door to Further everyday needs locally include a the right-hand corner. the garden and a good sized living room large supermarket, surgeries, a well- with patio doors leading to the garden. On equipped sports centre and post office Local Authority the first floor there are two bedrooms, a whilst there are also excellent schools bathroom, store cupboard and shower room catering for all ages.