SECOND TIME OFFENDER Intermediate Punishment Program Application Criminal Docket # OTN# ___
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

An Atomic Physics Perspective on the New Kilogram Defined by Planck's Constant
An atomic physics perspective on the new kilogram defined by Planck’s constant (Wolfgang Ketterle and Alan O. Jamison, MIT) (Manuscript submitted to Physics Today) On May 20, the kilogram will no longer be defined by the artefact in Paris, but through the definition1 of Planck’s constant h=6.626 070 15*10-34 kg m2/s. This is the result of advances in metrology: The best two measurements of h, the Watt balance and the silicon spheres, have now reached an accuracy similar to the mass drift of the ur-kilogram in Paris over 130 years. At this point, the General Conference on Weights and Measures decided to use the precisely measured numerical value of h as the definition of h, which then defines the unit of the kilogram. But how can we now explain in simple terms what exactly one kilogram is? How do fixed numerical values of h, the speed of light c and the Cs hyperfine frequency νCs define the kilogram? In this article we give a simple conceptual picture of the new kilogram and relate it to the practical realizations of the kilogram. A similar change occurred in 1983 for the definition of the meter when the speed of light was defined to be 299 792 458 m/s. Since the second was the time required for 9 192 631 770 oscillations of hyperfine radiation from a cesium atom, defining the speed of light defined the meter as the distance travelled by light in 1/9192631770 of a second, or equivalently, as 9192631770/299792458 times the wavelength of the cesium hyperfine radiation. -

Building the Bridge Between the First and Second Year Experience: a Collaborative Approach to Student Learning and Development STEP
Building the bridge between the first and second year experience: A collaborative approach to student learning and development STEP Introductions STEP Agenda for Today • Share research and theory that shapes first and second year programs • Differentiate programs, interventions, and support that should be targeted at first year students, second year students, or both • Think about your own department and how to work differently with first and second-year students • Review structure of FYE and STEP at Ohio State and where your office can support existing efforts STEP Learning Outcomes • Participants will reflect on and articulate what services, resources, and programming currently exist in their department for first and/or second year students. • Participants will articulate the key salient needs and developmental milestones that often distinguish the second year experience from the first. • Participants will be able to utilize at least one strategy for curriculum differentiation that will contribute to a more seamless experiences for students between their first and second year. Foundational Research that Informs FYE and STEP STEP Developmental Readiness and Sequencing • Developmental Readiness: “The ability and motivation to attend to, make meaning of, and appropriate new knowledge into one’s long term memory structures” (Hannah & Lester, 2009). • Sequencing: The order and structure in which people learn new skill sets (Hannah & Avolio, 2010). • Scaffolding: Support given during the learning process which is tailored to the needs of an -

Second Time Moms & the Truth About Parenting
Second Time Moms & The Truth About Parenting Summary Why does our case deserve an award? In the US, and globally, every diaper brand obsesses about the emotion and joy experienced by new parents. Luvs took the brave decision to focus exclusively on an audience that nobody was talking to: second time moms. Planning made Luvs the official diaper brand of experienced moms. The depth of insights Planning uncovered about this target led to creative work that did a very rare thing for the diaper category: it was funny, entertaining and sparked a record amount of debate. For the first time these moms felt that someone was finally standing up for them and Luvs was applauded for not being afraid to show motherhood in a more realistic way. And in doing so, we achieved the highest volume and value sales in the brand’s history. 2 Luvs: A Challenger Facing A Challenge Luvs is a value priced diaper brand that ranks a distant fourth in terms of value share within the US diaper category at 8.9%. Pampers and Huggies are both premium priced diapers that make up most of the category, with value share at 31, and 41 respectively. Private Label is the third biggest player with 19% value share. We needed to generate awareness to drive trial for Luvs in order to grow the brand, but a few things stood in our way. Low Share Of Voice Huggies spends $54 million on advertising and Pampers spends $48 million. In comparison, Luvs spends only $9 million in media support. So the two dominant diaper brands outspend us 9 to 1, making our goal of increased awareness very challenging. -

Second Amendment Rights
Second Amendment Rights Donald J. Trump on the Right to Keep and Bear Arms The Second Amendment to our Constitution is clear. The right of the people to keep and bear Arms shall not be infringed upon. Period. The Second Amendment guarantees a fundamental right that belongs to all law-abiding Americans. The Constitution doesn’t create that right – it ensures that the government can’t take it away. Our Founding Fathers knew, and our Supreme Court has upheld, that the Second Amendment’s purpose is to guarantee our right to defend ourselves and our families. This is about self-defense, plain and simple. It’s been said that the Second Amendment is America’s first freedom. That’s because the Right to Keep and Bear Arms protects all our other rights. We are the only country in the world that has a Second Amendment. Protecting that freedom is imperative. Here’s how we will do that: Enforce The Laws On The Books We need to get serious about prosecuting violent criminals. The Obama administration’s record on that is abysmal. Violent crime in cities like Baltimore, Chicago and many others is out of control. Drug dealers and gang members are given a slap on the wrist and turned loose on the street. This needs to stop. Several years ago there was a tremendous program in Richmond, Virginia called Project Exile. It said that if a violent felon uses a gun to commit a crime, you will be prosecuted in federal court and go to prison for five years – no parole or early release. -

Accounting Recommended Four-Year Plan (Fall 2010)
Anisfield School of Business Accounting Recommended Four-Year Plan (Fall 2010) This recommended four-year plan is designed to provide a blueprint for students to complete their degrees within four years. These plans are the recommended sequences of courses. Students must meet with their Major Advisor to develop a more individualized plan to complete their degree. This plan assumes that no developmental courses are required. If developmental courses are needed, students may have additional requirements to fulfill which are not listed in the plan and degree completion may take longer. NOTE: This recommended Four-Year Plan is applicable to students admitted into the major during the 2010-2011 academic year. First Year Fall Semester HRS Spring Semester HRS GenEd: INTD 101-First Year Seminar 4 School Core: ECON 101-Microeconomics 4 GenEd: ENGL 180-College English 4 GenEd: Science w/ Experiential 4 GenEd/School Core: BADM 115-Perspectives 4 GenEd: History 4 of Business & Society GenEd: MATH 101, 110 or 121-Mathematics 4 Major: INFO 224-Principles of Information 4 Technology Total: 16 Total: 16 Second Year Fall Semester HRS Spring Semester HRS Major: ACCT 221-Principles of Financial 4 Major: ACCT 222-Principles of Managerial 4 Accounting Accounting Major: MKTG 290-Marketing Principles & 4 GenEd: AIID 201-Readings in Humanities 4 Practices Major: BADM 225-Management Statistics 4 Major: FINC 301-Corporate Finance I 4 School Core: ECON 102-Macroeconomics 4 Major: BADM 223-Business Law 1 4 Total: 16 Total: 16 Third Year Fall Semester HRS Spring -
Guide for the Use of the International System of Units (SI)
Guide for the Use of the International System of Units (SI) m kg s cd SI mol K A NIST Special Publication 811 2008 Edition Ambler Thompson and Barry N. Taylor NIST Special Publication 811 2008 Edition Guide for the Use of the International System of Units (SI) Ambler Thompson Technology Services and Barry N. Taylor Physics Laboratory National Institute of Standards and Technology Gaithersburg, MD 20899 (Supersedes NIST Special Publication 811, 1995 Edition, April 1995) March 2008 U.S. Department of Commerce Carlos M. Gutierrez, Secretary National Institute of Standards and Technology James M. Turner, Acting Director National Institute of Standards and Technology Special Publication 811, 2008 Edition (Supersedes NIST Special Publication 811, April 1995 Edition) Natl. Inst. Stand. Technol. Spec. Publ. 811, 2008 Ed., 85 pages (March 2008; 2nd printing November 2008) CODEN: NSPUE3 Note on 2nd printing: This 2nd printing dated November 2008 of NIST SP811 corrects a number of minor typographical errors present in the 1st printing dated March 2008. Guide for the Use of the International System of Units (SI) Preface The International System of Units, universally abbreviated SI (from the French Le Système International d’Unités), is the modern metric system of measurement. Long the dominant measurement system used in science, the SI is becoming the dominant measurement system used in international commerce. The Omnibus Trade and Competitiveness Act of August 1988 [Public Law (PL) 100-418] changed the name of the National Bureau of Standards (NBS) to the National Institute of Standards and Technology (NIST) and gave to NIST the added task of helping U.S. -

Pdf/Dudaspji0709.Pdf
Every Second The Impact of the Incarceration Crisis on America’s Families the impact of incarceration on america’s families | section name 1 FWD.us is a bipartisan political organization that believes America’s families, communities, and economy thrive when everyone has the opportunity to achieve their full potential. For too long, our broken immigration and criminal justice systems have locked too many people out from the American dream. Founded by leaders in the technology and business communities, we seek to grow and galvanize political support to break through partisan gridlock and achieve meaningful reforms. Together, we can move America forward. December 2018, Published by: FWD.us For further information, please visit fwd.us. Acknowledgments This report would not have been possible without the hard work, advice, and support of the full FWD.us team and many advocates, directly impacted persons, and academic advisors. In particular, we would like to thank members of our advisory board and all the researchers who contributed to the development and analysis of the survey. We must also acknowledge the thousands of people who responded anonymously to our survey, thus sharing their experiences and stories with us. ADVISORY BOARD RESEARCH TEAM Frederick Hutson Principal Investigator: CEO, Pigeonly Christopher Wildeman Professor of Policy Analysis and REPORT WRITERS AND Patrick McCarthy Management, Provost Fellow for KEY CONTRIBUTORS President and CEO, Annie E. the Social Sciences, and Director Casey Foundation Brian Elderbroom, Laura Bennett, -
Atomic Clocks: an Application of Spectroscopy in the Last Installment of This Column (1), I Talked About Clocks As the First Scientific Instrument
14 Spectroscopy 21(1) January 2007 www.spectroscopyonline.com The Baseline Atomic Clocks: An Application of Spectroscopy In the last installment of this column (1), I talked about clocks as the first scientific instrument. What do clocks have to do with spectroscopy? Actually, the world’s most accurate clocks, atomic clocks, are based upon a spectroscopic transition of cesium or other elements, making spectroscopy a fundamental tool in our measurements of the natural universe. David W. Ball ime is one of the seven fundamental quantities in Originally, a second was defined as part of a minute, nature. I made a case in the last installment of this which was part of an hour, which was in turn defined as T column (1) that mechanical devices for measuring part of a day. Thus, 1 s was 1/(60 ϫ 60 24), or 1/86,400 time — clocks — might be considered the world’s first sci- of a day. However, even by the 17th century, defining the entific instruments. Clocks are ubiquitous because the day itself was difficult. Was the day based upon the position measurement of time is a fundamental activity that is im- of the sun (the solar day) or the position of distant stars portant to computer users, pilots, and lollygaggers alike. (the sidereal day)? At what latitude (that is, position toward the north or south) is a day measured? Over time it was rec- The Second ognized that measuring time accurately was a challenge. Quantities of time are expressed in a variety of units that In 1660, the Royal Society proposed that a second be de- we teach our grade-schoolers, but the IUPAC-approved termined by the half-period (that is, one swing) of a pendu- fundamental unit of time is the second (abbreviated “s” not lum of a given length. -

The International System of Units (SI)
NAT'L INST. OF STAND & TECH NIST National Institute of Standards and Technology Technology Administration, U.S. Department of Commerce NIST Special Publication 330 2001 Edition The International System of Units (SI) 4. Barry N. Taylor, Editor r A o o L57 330 2oOI rhe National Institute of Standards and Technology was established in 1988 by Congress to "assist industry in the development of technology . needed to improve product quality, to modernize manufacturing processes, to ensure product reliability . and to facilitate rapid commercialization ... of products based on new scientific discoveries." NIST, originally founded as the National Bureau of Standards in 1901, works to strengthen U.S. industry's competitiveness; advance science and engineering; and improve public health, safety, and the environment. One of the agency's basic functions is to develop, maintain, and retain custody of the national standards of measurement, and provide the means and methods for comparing standards used in science, engineering, manufacturing, commerce, industry, and education with the standards adopted or recognized by the Federal Government. As an agency of the U.S. Commerce Department's Technology Administration, NIST conducts basic and applied research in the physical sciences and engineering, and develops measurement techniques, test methods, standards, and related services. The Institute does generic and precompetitive work on new and advanced technologies. NIST's research facilities are located at Gaithersburg, MD 20899, and at Boulder, CO 80303. -

Secondsecond Dayday
THE CAMP INVENTION DAILY SECONDSECOND DAYDAY HERE’S WHAT’S HAPPENING AT CAMP! CAMP INVENTION CHAMPIONS™ Today we met the inventors behind our sports gear—like National Inventors Hall of Fame® (NIHF) Inductees Stephanie Kwolek, the inventor of Kevlar® fiber, which is used in safety equipment, and Joseph Shivers, the inventor of LYCRA® fiber, which is used in sportswear for activities on land and water! It was tough to choose our next draft picks for our Innovation Dream Team after hearing all about these game-changing innovations. The focus on our sports complex today was to add moving pieces and simple machines. RESCUE SQUAD™ We zipped into a riverside town and met with the local Wildlife Resource Ranger to receive our next mission. He explained that because salmon are in short supply, bears are raiding city trash cans. We discovered that beavers LED BODY SPEAKER play an important role in balancing this river’s ecosystem. Today’s level OUTER SHELL LEDs on the Speaker to included airdropping beavers, creating habitats for hatching salmon and airplane’s shell A plane’s outer speak to control safely moving young salmon past hydroelectric dams. The river’s ecosystem shell tower balance has been restored and we’re ready to level up! CAMP INVENTION FLIGHT LAB™ We earned our second wing from today’s flight simulation challenge! We CAMP INVENTION AT HOME explored thrust and experimented with wing dynamics using gliders and paper airplanes. LINK provided a moving, illuminated target as we tested MAKING CONNECTIONS our aeronautical designs. We also got to personalize our own LINK, adding feathers and customized stickers. -
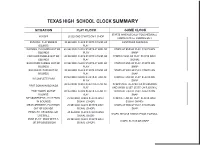
Texas High School Clock Summary
TEXAS HIGH SCHOOL CLOCK SUMMARY SITUATION PLAY CLOCK GAME CLOCK STARTS WHEN LEGALLY TOUCHED/BALL KICKOFF 25 SECOND STARTS ON R CHOP CROSSES B'S GL COMING OUT RUNNING PLAY ENDS IN 40 SECOND CLOCK STARTS AT END OF CONTINUES RUNNING BOUNDS PLAY RUNNING PLAY ENDS OUT OF 40 SECOND CLOCK STARTS AT END OF STOPS AT END OF PLAY. STARTS ON BOUNDS PLAY SNAP FORWARD FUMBLE OUT OF 40 SECOND CLOCK STARTS AT END OF STOPS AT END OF PLAY. STARTS ON R BOUNDS PLAY SIGNAL BACKWARD FUMBLE OUT OF 40 SECOND CLOCK STARTS AT END OF STOPS AT END OF PLAY. STARTS ON BOUNDS PLAY SNAP BACKWARD PASS OUT OF 40 SECOND CLOCK STARTS AT END OF STOPS AT END OF PLAY. STARTS ON BOUNDS PLAY SNAP 40 SECOND CLOCK STARTS AT END OF STOPS AT END OF PLAY. STARTS ON INCOMPLETE PASS PLAY SNAP 40 SECOND CLOCK STARTS AT END OF STOPS UNTIL RE-SPOTTED IN BOUNDS FIRST DOWN IN BOUNDS PLAY AND CHAIN IS SET. START ON R SIGNAL FIRST DOWN OUT OF 40 SECOND CLOCK STARTS AT END OF STOPS AT END OF PLAY. STARTS ON BOUNDS PLAY SNAP MEASUREMENT-- PLAY ENDS 25 SECOND CLOCK STARTS ON R STOPS AT END OF PLAY. STARTS ON R IN BOUNDS SIGNAL (CHOP) SIGNAL {WIND) MEASUREMENT- PLAY ENDS 25 SECOND CLOCK STARTS ON R STOPS AT END OF PLAY. STARTS ON OUT OF BOUNDS SIGNAL (CHOP) SNAP PENALTV- DEAD BALL OR 25 SECOND CLOCK STARTS ON R STOPS. RETAINS STATUS PRIOR TO FOUL LIVE BALL SIGNAL (CHOP) PUNT PLAY- ENDS WITH A 25 SECOND CLOCK STARTS ON R STOPS. -

1. Measurements in Physics.Nb
Lecture #1: Measurements in Physics Base Quantities: Length, time, and mass. Base Units: meter, second, kilogram System Internationale Units or S.I. Units ü Formerly the "metric system" or M.K.S. system (1971) ü Other systems: 1.C.G.S. System (centimeter, grams, seconds) 2.English System (inches, pounds, seconds) ü Common Metric System Prefixes (powers of 10) kilo- (e.g. kilogram, kilometer) 1000=103 1 kilometer=1,000 meters mega- (e.g. mega-meter) 1,000,000=106 1 mega-meter=1,000,000 meters=1,000 kilometers milli (e.g. millimeter or mu) 1 millimeter = 10-3 m micro- (e.g. micrometer or micron) 1 mM= 10-6 m Nano (e.g nanometer) 1 nm = 10-9 m Properties of a Unit Standard ü Easily accessible for users around the globe. 1. Second was originally defined in terms of the rotation of the Earth in one day. Now defined in terms of frequency of an atomic (Cesium) "Atomic Clocks" 2. Meter was originally defined as the distance between two marks on a standard metal bar in Paris. Now defined as the distance light travels in a given time. 3. The kilogram or kg was originally defined by a standard mass in Paris. Now the kilogram is defined in terms of the isotope of Carbon 12. ü The standard should not be variable. ü Independent of spatial location 1. The unit standard of time (and space) should be the same in Paris as in New York. The unit standard of time (and space) should be the same at Alpha Centari star system as it is on Earth.