Hemiplegic Shoulder Pain in Shoulder Subluxation After Stroke: Associated with Range of Motion Limitation
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Evaluation of Humeral and Glenoid Bone Deformity in Glenohumeral Arthritis 5
Evaluation of Humeral and Glenoid Bone Deformity 1 in Glenohumeral Arthritis Brian F. Grogan and Charles M. Jobin Introduction glenoid bone wear helps the surgeon formulate a successful treatment plan and surgical goals Glenohumeral arthritis is the sequela of a vari- to address the pathoanatomy and improve the ety of pathologic shoulder processes, most durability of shoulder arthroplasty. The evalu- commonly degenerative osteoarthritis, but may ation of humeral and glenoid bone deformity also be secondary to post-traumatic conditions, in glenohumeral arthritis has profound surgical inflammatory arthritis, rotator cuff tear arthrop- implications and is fundamental to successful athy, and postsurgical conditions most com- shoulder arthroplasty. monly post-capsulorrhaphy arthritis. Patients with glenohumeral arthritis commonly demon- strate patterns of bony deformity on the glenoid Glenoid Deformity in Osteoarthritis and humerus that are caused by the etiology of the arthritis. For example, osteoarthritis com- Glenoid deformity and glenohumeral subluxation monly presents with posterior glenoid wear, are commonly seen in the setting of primary osteo- secondary glenoid retroversion, and posterior arthritis of the glenohumeral joint. The glenoid humeral head subluxation, while inflammatory wear tends to occur posteriorly and may be best arthritis routinely causes concentric glenoid viewed on axial radiographs or computed tomog- wear with central glenoid erosion. A thorough raphy (CT) axial images. Glenoid erosion, as first history and physical, as well as laboratory and characterized by Walch, is noted to be either central radiographic workup, are keys to understanding or posterior, with varying degrees of wear and pos- the etiology of arthritis and understanding the terior subluxation of the humerus [1, 2] (Fig. -

Peroneal Tendon Subluxation
CHAPTER 4 Peroneal Tendon Subluxation Jessica Lickiss, DPM Jay D. Ryan, DPM INTRODUCTION Peroneal tendon subluxation/ instability can be challenging IMAGING AND CLASSIFICATION to diagnose depending on the level of disruption and deformity present. Subtle cases will appear in the clinical Radiographs can be used to identify an avulsion and rule out setting similar to a lateral ankle sprain. This can cause a delay fracture. Computed tomography (CT) scan and MRI are in care and poorer outcomes for patients. both viable options for evaluation. MRI better evaluates the health of the peroneal tendons and CT scan demonstrates ANATOMY the shape and position of the fibula and fibular groove. While advanced imaging is a great adjunct, the diagnosis is mainly The peroneus longus and brevis muscle bellies travel clinical. For more subtle injuries where the tendons do not posterior to the fibula and fibular groove. At the fibular completely sublux or dislocate the fibula, dynamic ultrasound groove they are combined into one sheath; they separate can be used for diagnosing intrasheath instability (5). usually at the level of the peroneal tubercle. They are bound Eckert and Davis created a classification in 1976 for superiorly by the superior peroneal retinaculum (SPR) and SPR injuries (6). Grade I injuries involve elevation of the inferiorly by the calcaneofibular ligament (CFL) and the retinaculum from the lateral malleolus and the tendons inferior peroneal retinaculum (IPR). The superior peroneal can dislocate between the bone and periosteum. Grade II retinaculum has fibers that extend superiorly, posteriorly, injuries involve the fibrocartilaginous ridge elevating with and medially approximately 3.5 cm from the distal tip of the the retinaculum and tendon subluxed between it and the fibula (1). -

Sacroiliac Joint Injury and Dysfunction: an Overlooked Cause of Low Back and Buttock Pain
Sacroiliac Joint Injury and Dysfunction: An overlooked cause of Low Back and Buttock Pain. Author: Shannon P. Goossen, AP, LMT, CMTPT- 2003 The sacroiliac joint can be the cause of debilitating low back and buttock pain. It can additionally be the culprit of pseudo-sciatica, which was described by Smith- Peterson in 1926. Unfortunately, in as much as muscles are the “orphan organ” in the diagnosis of chronic pain, the sacroiliac joint is the “orphan joint” in the differential diagnosis of spinal disorders and low back pain. What is more disturbing is that in order to effectively treat SIJ injury and dysfunction, one must have an understanding of both myofascial and joint dysfunction. This could easily explain the controversy in evaluation, diagnosis and treatment. Fortunately, studies in the last decade have validated that the SIJ may be the primary pain generator in up to 30% of patients reporting low back pain below the level of L5 –S1 (Schwarzer, A et. al). Other studies and physicians treating SIJ have supported this conclusion as well. The sacroiliac joint is complex. It has the characteristics of a synovial joint with hyaline cartilage lining the sacral side of the joint, and fibrocartilage lining the ilial side of the joint. It is also defined as a synarthrosis and amphiarthrosis. It has more mobility early in life, and generally between 40-50 years of age, degenerative changes take place, and the joint stiffens in men and women. Although the actual amount of movement in the SIJ has been a source of controversy, up to 4 degrees of rotation and 1.6 mm of translation is expected in young adults (Vleeming et. -

Thumb Carpometacarpal Arthritis 952-920-0970
Douglas Drake, MD Orthopedic Surgeon and Hand Specialist 3250 W. 66th St. Suite #100 Edina, MN 55435 Thumb Carpometacarpal Arthritis 952-920-0970 Thumb CMC Arthritis: Idiopathic thumb basal joint aka thumb CMC arthritis StageIII: Continued joint narrowing with cystic changes is a result of anatomic factors that predispose the CMC and sclerotic bone formarion. Prominent osteophytes joint instability, such as joint configuration and ligamen- are present wiht moderate subluxation at the cmc joint tous laxity. CMC joint instability results in shear forces and subluxation at the MCP joint. at the joint surfaces and subsequent joint degeneration. Stage IV: All the components of stage III along with destruction of the scaphotrapezial joint. At this stage the CMC joint is usually fixed and some patients may have little to no pain. Treatment: In early stages, stage I and sometimes stage II, con- servative treatment should be considered. Conservative treatment consists of a period of thumb immobilization in a removable splint, see picture below, and use of NSAID’s. If splinting fails to relieve the pain then a corticosteroid injection may be performed. Of note, corticosteroid injections will not alter the progression of Prevalence: the disease but it may provide a few months of relief. Idiopathic thumb CMC arthritis is most common If conservative treatment fails to provide relief and pain amount women 40-70 years old. Women are 15 to 20 is making it difficult for the patient to perform daily times more likely than men to have thumb CMC arthri- functions or disease has progressed to stage III or IV tis; this is most likely secondary to increased joint laxity then surgical treatment in healthy patients should be found in women when compared to men. -

Marfan Syndrome: Jeffrey Welder MSIII, Erik L
Marfan Syndrome: Jeffrey Welder MSIII, Erik L. Nylen MSE, Thomas Oetting MS MD May 6, 2010 Chief Complaint: Decreased vision and glare in both eyes. History of Present Illness: A 28 year old woman with a history of Marfan syndrome presented to the comprehensive ophthalmology clinic reporting a progressive decrease in vision and worsening glare in both eyes. She had been seen by ophthalmologists in the past, and had been told that her crystalline lenses were subluxed in both eyes. She had not had problems with her vision until recent months. Past Medical History: Marfan syndrome with aortic stenosis followed by cardiology Medications: Oral beta blocker Family History: No known family members with Marfan Syndrome. Grandmother with glaucoma. Social History: The patient is a graduate student. Ocular Exam: External Exam normal. VA (with correction): OD 20/40 OS 20/50 Current glasses: OD: 6.75+ 5.00 x 135 OS: -5.25 + 4.25 x 60 Pupils: No anisocoria and no relative afferent pupillary defect Motility: Ocular motility full OU. Anterior segment exam: Inferiorly subluxed lenses OU (figure 1 and 2). The angle was deep OU and there was no lens apposition to the cornea in either eye. Dilated funduscopic exam: Posterior segment was normal OU with no peripheral retinal degeneration . Course: The patient’s subluxed lenses led to poor vision from peripheral lenticular irregular astigmatism and glare. She was taken to the operating room where her relatively clear lenses were removed and iris sutured intraocular lenses were placed. The surgical video for one of the eyes may be viewed at http://www.facebook.com/video/video.php?v=153379281140 Page | 1 Figure One: Note the inferiorly subluxed lens. -

Peroneal Tendon Disorders
Dr Todd Gothelf www.orthosports.com.au 47‐49 Burwood Road, Concord 29‐31 Dora Street, Hurstville 119‐121 Lethbridge Street, Penrith 160 Belmore Road, Randwick Dr Todd Gothelf Shoulder, Foot & Ankle Surgery Peroneal Tendon Disorders Dr Todd Gothelf Shoulder, Foot & Ankle Surgery Peroneal Tendon Disorders • Tenosynovitis •Tears • Snapping Peroneal Tendons Dr Todd Gothelf Shoulder, Foot & Ankle Surgery Cause of injury •Occur during acute ankle sprain •Can occur as well by attrition over time. • Multiple ankle sprains/recurrent instability Dr Todd Gothelf Shoulder, Foot & Ankle Surgery Lateral Ankle Sprain •“Complete Rupture of the ATFL Ligament” •Treated Non‐ operatively Dr Todd Gothelf Shoulder, Foot & Ankle Surgery ACL Rupture/ Rotator Cuff Tear •“Complete Rupture of the ACL ligament” •“Full Thickness tear of the Rotator Cuff • Usually require surgery Dr Todd Gothelf Shoulder, Foot & Ankle Surgery Dr Todd Gothelf Shoulder, Foot & Ankle Surgery Dr Todd Gothelf Shoulder, Foot & Ankle Surgery Lateral Ankle Sprains •Treat the complete ATFL rupture NON‐ operatively • Similar outcomes to surgical treatment with LESS RISK. •Can Always do surgery later on. Dr Todd Gothelf Shoulder, Foot & Ankle Surgery Causes of Pain after Lateral Ankle Sprain‐ NOT ATFL •Talardome lesions •Intra‐articular scar tissue, impingement • Peroneal tendon tears • Peroneal tendon dislocations •Missed achilles •Missed Syndesmosis •Missed Lis Franc Dr Todd Gothelf Shoulder, Foot & Ankle Surgery Anatomy Peroneal Tendons •Acute Angle around fibula • Eversion/Flexion •SPR‐ -
Shoulder Instability and Labral Tears
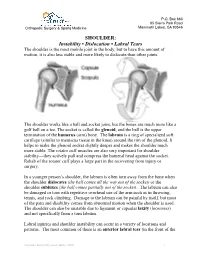
P.O. Box 660 85 Sierra Park Road Orthopedic Surgery & Sports Medicine Mammoth Lakes, CA 93546 SHOULDER: Instability • Dislocation • Labral Tears The shoulder is the most mobile joint in the body, but to have this amount of motion, it is also less stable and more likely to dislocate than other joints. The shoulder works like a ball and socket joint, but the bones are much more like a golf ball on a tee. The socket is called the glenoid, and the ball is the upper termination of the humerus (arm) bone. The labrum is a ring of specialized soft cartilage (similar to meniscus tissue in the knee) around the rim of the glenoid. It helps to make the glenoid socket slightly deeper and makes the shoulder much more stable. The rotator cuff muscles are also very important for shoulder stability—they actively pull and compress the humeral head against the socket. Rehab of the rotator cuff plays a large part in the recovering from injury or surgery. In a younger person’s shoulder, the labrum is often torn away from the bone when the shoulder dislocates (the ball comes all the way out of the socket) or the shoulder subluxes (the ball comes partially out of the socket). The labrum can also be damaged or torn with repetitive overhead use of the arm such as in throwing, tennis, and rock climbing. Damage to the labrum can be painful by itself, but most of the pain and disability comes from abnormal motion when the shoulder is used. The shoulder can also be unstable due to ligament or capsular laxity (looseness) and not specifically from a torn labrum. -

A Case of Peroneal Tendon Subluxation Following Trivial Ankle
Hong Kong Journal of Orthopaedic Research 2020; 3(2): 32-34 Case Report A Case of Peroneal Tendon Subluxation following Trivial Hong Kong J Orthop Res ISSN (e): 2663-8231 Ankle Injury and Review of the Literature ISSN (p): 2663-8223 2020; 3(2): 32-34 Suman Kumar Shrestha1, Pramod Devkota2, Balakrishnan M Acharya3, Toya Raj Bhatta4 © 2020, All rights reserved 1 Department of Orthopaedics and Trauma Surgery, Patan Academy of Health Sciences, Patan Hospital, Lalitpur, www.hkorthopaedicjournal.com Nepal. https://orcid.org/0000-0001-8793-6466 2 Department of Orthopaedics and Trauma Surgery, Patan Academy of Health Sciences, Patan Hospital, Lalitpur, Nepal. https://orcid.org/0000-0003-4088-0199 3 Department of Orthopaedics and Trauma Surgery, Patan Academy of Health Sciences, Patan Hospital, Lalitpur, Nepal. https://orcid.org/0000-0002-5543-6317 4 Department of Orthopaedics and Trauma Surgery, Patan Academy of Health Sciences, Patan Hospital, Lalitpur, Nepal. https://orcid.org/0000-0002-6067-8177 Abstract Subluxation or dislocation of the peroneal tendon is uncommon ankle disorder and most of the time misdiagnosed as ankle sprain. Young adults and adolescents who are active on sports activities are more prone to get this problem. The main cause of this disorder is because of the superior peroneal retinaculum avulsion from its insertion with fibular bone. We report a case of peroneal subluxation in a 19-year-old girl after twisting of the ankle one year back. She was initially treated with ankle splintage, rest and analgesics but her problem did not improve. Magnetic resonance imaging (MRI) of the ankle showed subluxation of the peroneal tendon and managed operatively. -

Anterosuperior Dislocation of the Shoulder Joint in an Older Patient with Parkinson’S Disease
Kobe J. Med. Sci., Vol. 54, No. 5, pp. E237-E240, 2008 Anterosuperior Dislocation of the Shoulder Joint in an Older Patient with Parkinson’s Disease TOKIO MATSUZAKI, TAKESHI KOKUBU*, ISSEI NAGURA, NARIKAZU TOYOKAWA, ATSUYUKI INUI, HIROYUKI FUJIOKA, MINORU DOITA and MASAHIRO KUROSAKA Department of Orthopaedic Surgery, Kobe University Graduate School of Medicine, Japan Received 10 September 2008/ Accepted 17 December 2008 Key Words: anterosuperior dislocation, shoulder, trauma, Parkinson’s disease An 83-year-old woman, subsequently diagnosed with Parkinson’s disease, fell on her right shoulder. Radiographs showed the humeral head dislocated anterosuperiorly. The supraspinatus tendon was massively disrupted and judged irreparable. The subscapularis tendon was repaired, however re-dislocation of the humeral head was confirmed after the surgery but further treatment was rejected as she was almost pain free and had a low activity level. The patient was followed up for one year after surgery and her shoulder became almost pain-free, but range of motion with active elevation was limited. In such cases a goal of absence or reduction of pain rather than real repair might be considered appropriate. Traumatic dislocations of the shoulder joint are usually described as anteroinferior dislocations. Anterosuperior dislocations are extremely rare, since the coracoacromial arch prevents the humeral head from translating to the superior direction anatomically. We report a rare case of traumatic anterosuperior shoulder dislocation in an older patient with Parkinson’s disease and discuss its clinical manifestations. CLINICAL CASE An 83-year-old woman fell on her right shoulder. Five days after injury, she was referred to our hospital as the pain had not abated. -

SUBLUXATION of the ANKLE Cases of Subluxation of The
92 PENNAL: SUBLUXATION OF THE ANKLE rCan. M. A. J. L[Aug. 1943,vol.49 and showed fibromuscular proliferation, hyalini- zation or complete necrosis (see Fig. 6). SUBLUXATION OF THE ANKLE By Major G. F. Pennal, R.C.A.M.C. SUMMARY AND CONCLUSIONS The nephroselerosis produced by D.C.A. over- TJHE basis of this article is a series of fourteen dosage in the rat is particularly pronounced if cases of subluxation of the ankle encountered the animals are kept on a high NaCl intake. in the past year at Camp Borden Military Hos- Under such conditions D.C.A. causes a pro- pital. The term subluxation is used to define nounced rise in systolic and diastolic blood pres- those injuries resulting in a complete tear of sure, marked diuresis with increased excretion the external lateral ligament of the ankle with of sodium and chloride, proteinuria and clinical a subsequent momentary or recurrent outward signs of severe cardiac decompensation. In some dislocation of the astragalus, unaccompanied by instances death ensues, due to htemorrhagic fracture. lung cedema. The following case history may indicate that The characteristic pathological findings in these injuries are disabling and merit further rats so treated are hypertrophy and capsular consideration. fibrosis of the renal glomeruli with hyaliniza- CASE 12 tion of their tuft capillaries. Fibrosis, hyalini- A man aged 34. Three and one-half months previous zation and even actual necrosis of the arteriolar to consultation, he had slipped and severely wrenched the left ankle whilst running. At that time he was walls is evident not only in the kidney itself- removed to hospital. -

Peroneal Tendon Dislocations Are Traumatic Events
324 MANKEY TENDON INJURY AND RECONSTRUCTION 1083-7515/96 $0.00 + .20 a tendon graft is used it is assumed that the repair is not under undue tension; therefore, the cast need not be applied in dorsiflexion and weight bearing is allowed. PERONEAL TENDON RESULTS DISLOCATIONS Surgical repair or reconstruction of a ruptured tibialis anterior pro duced uniformly good results with return to preinjury activity in almost William C. McGarvey, MD, and Thomas O. Clanton, MD all reported cases. Only one case in which surgery had been performed was noted to have persistent disability.3 Persistent symptoms have been reported in patients treated nonoperatively, although they seem to do well overall because of their low level of activity. Most investigators recommend surgical repair for the symptomatic patient, with a moderate 1 6 7 % to high activity level unless otherwise contraindicated. ' - ' n Although 5 no significant complications have been reported, Mann outlined potential Subluxation or dislocation of the peroneal tendons is an uncommon risks of surgical intervention: to prevent adhesions the incision should injury compounded by the fact that there are frequently only subtle differ not lie directly over the tendon, and if possible, should lie slightly medial ences separating these injuries from the much more common and better to it; the pull-out wire should draw the tendon beneath the extensor recognized lateral ankle sprain. The first description dates back to 1803, retinaculum, otherwise the wire will tent the tendon, resulting in a difficult when Monteggia reported this problem on a ballet dancer.30 The first wound closure. reports of treatment directed at this injury were submitted by Blanulet5 in 1875 and Gutierrez17 two years later. -

The Pesky Peroneal Tendons & Tales of Subluxation
The Pesky Peroneal Tendons & Tales of Subluxation Jason R. Miller, DPM, FACFAS Residency Director, Phoenixville Hospital PMSR/RRA Director, PA Intensive Lower Extremity Fellowship Program Adjunct Associate Professor, Dept. of Surgery, TUSPM Chief, Foot & Ankle Surgery, Pennsylvania Orthopaedic Center/Premier Orthopedics Presentation • Overall, peroneal tendon disorders are reportedly rare, with peroneal brevis involvement being more common than peroneus longus involvement, and with both longus and brevis involvement being the least common • Associated with lateral ankle sprain or insult, but occasionally no traumatic event is noted in patient’s history • Frequently overlooked and misdiagnosed due to assumption the injury is to the lateral ankle ligaments Molloy, R. et al (2003). Failed Treatment of Peroneal Tendon Injuries. Foot and Ankle Clinics of North America, 8, pp. 115-129. Becker, H.P. et al (1996). Functional Disorders of the Foot After Tenodesis: Is the Method Still Currently Acceptable? Sportverletz Sportschanden, 10:4, pp. 94-99. Presentation • Tears are generally degenerative in nature, look for history of repetitive lateral ankle sprains/lateral ankle instability • More commonly associated with a cavus foot type, hindfoot varus, and peroneal subluxation • Swelling along the peroneals is the most consistent clinical finding on exam (as much as 90%) Molloy, R. et al (2003). Failed Treatment of Peroneal Tendon Injuries. Foot and Ankle Clinics of North America, 8, pp. 115-129. Slater, H.K (2007). Acute Peroneal Tendon Tears. Foot and Ankle Clinics of North America, 12, pp. 759-674. Squires, N. et al (2007). Surgical Treatment of Peroneal Tendon Tears. Foot and Ankle Clinics of North America, 12, pp.