Target-Specific PET Probes for Neurodegenerative Disorders
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
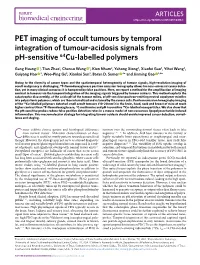
PET Imaging of Occult Tumours by Temporal Integration of Tumour-Acidosis Signals from Ph-Sensitive 64Cu-Labelled Polymers
ARTICLES https://doi.org/10.1038/s41551-019-0416-1 PET imaging of occult tumours by temporal integration of tumour-acidosis signals from pH-sensitive 64Cu-labelled polymers Gang Huang 1, Tian Zhao1, Chensu Wang 1, Kien Nham2, Yahong Xiong2, Xiaofei Gao3, Yihui Wang3, Guiyang Hao 2, Woo-Ping Ge3, Xiankai Sun2, Baran D. Sumer 4* and Jinming Gao 1,4* Owing to the diversity of cancer types and the spatiotemporal heterogeneity of tumour signals, high-resolution imaging of occult malignancy is challenging. 18F-fluorodeoxyglucose positron emission tomography allows for near-universal cancer detec- tion, yet in many clinical scenarios it is hampered by false positives. Here, we report a method for the amplification of imaging contrast in tumours via the temporal integration of the imaging signals triggered by tumour acidosis. This method exploits the catastrophic disassembly, at the acidic pH of the tumour milieu, of pH-sensitive positron-emitting neutral copolymer micelles into polycationic polymers, which are then internalized and retained by the cancer cells. Positron emission tomography imaging of the 64Cu-labelled polymers detected small occult tumours (10–20 mm3) in the brain, head, neck and breast of mice at much higher contrast than 18F-fluorodeoxyglucose, 11C-methionine and pH-insensitive 64Cu-labelled nanoparticles. We also show that the pH-sensitive probes reduce false positive detection rates in a mouse model of non-cancerous lipopolysaccharide-induced inflammation. This macromolecular strategy for integrating tumour acidosis should enable improved cancer detection, surveil- lance and staging. ancer exhibits diverse genetic and histological differences tumours over the surrounding normal tissues often leads to false from normal tissues1. -

A Technique for Standardized Central Analysis of 6-18F-Fluoro-L-DOPA PET Data from a Multicenter Study
A Technique for Standardized Central Analysis of 6-18F-Fluoro-L-DOPA PET Data from a Multicenter Study Alan L. Whone, MRCP1; Dale L. Bailey, PhD2; Philippe Remy, PhD3; Nicola Pavese, MD1; and David J. Brooks, DSc1 1Division of Neuroscience and MRC Clinical Sciences Centre, Faculty of Medicine, Imperial College, Hammersmith Hospital, London, United Kingdom; 2Department of Nuclear Medicine, Royal North Shore Hospital, Sydney, Australia; and 3CEA-Centre National de la Recherche Scientifique Unite´ de Recherche Associe´e 2210, Service Hospitalier Frederic Joliot, Orsay, France tralized analysis offers the potential for improved detection of We have recently completed a large 6-18F-fluoro-L-DOPA (18F- outcomes due to the standardization of the analytic approach DOPA) PET study comparing rates of loss of dopamine terminal and allows the analysis of large numbers of PET studies. function in Parkinson’s disease (PD) patients taking either the Key Words: PET; 18F-DOPA; Parkinson’s disease; progression; dopamine agonist ropinirole or L-DOPA. This trial involved a central analysis “distributed acquisition/centralized analysis” method, in which J Nucl Med 2004; 45:1135–1145 18F-DOPA images were acquired at 6 different PET centers around the world and then analyzed at a single site. To our knowledge, this is the first time such a centralized approach has been employed with 18F-DOPA PET and this descriptive basic science article outlines the methods used. Methods: One hun- With rapid advances in molecular medicine, the pro- dred eighty-six PD patients were randomized (1:1) to ropinirole duction of neuroprotective or neurorestorative agents that or L-DOPA therapy, and 18F-DOPA PET was performed at base- affect the progression of degenerative conditions such as line and again at 2 y. -
![[123I]FP-CIT SPECT in Atypical Degenerative Parkinsonism](https://docslib.b-cdn.net/cover/2351/123i-fp-cit-spect-in-atypical-degenerative-parkinsonism-242351.webp)
[123I]FP-CIT SPECT in Atypical Degenerative Parkinsonism
CONTRAST AGENT EVALUATION [123I]FP-CIT SPECT in atypical degenerative parkinsonism One of the most widely used techniques to support the clinical diagnosis of Parkinson’s disease is the SPECT scan with [123I]FP-CIT. This tracer binds reversibly and visualizes the striatal presynaptic dopamine transporters. Several uncertainties remain on the value of [123I]FP-CIT and SPECT in atypical degenerative parkinsonian syndromes. In this concise review, we discuss the contribution of SPECT and [123I]FP-CIT in supporting the clinical diagnosis of Parkinson’s disease and their role in the differential diagnosis of Parkinson’s disease and atypical degenerative parkinsonism. The chemistry, pharmacodynamics and pharmacokinetics of [123I]FP-CIT are also discussed. 1,2,3 KEywordS: atypical degenerative parkinsonism n FP-CIT n ioflupane n SPECT Ioannis U Isaias* , Giorgio Marotta4, Gianni Pezzoli2, Parkinson’s disease (PD) is the second most dystonic tremor [15] and psychogenic parkin- Osama Sabri5 [1] [16,17] 5,6 common neurodegenerative disorder , yet sonism . In this concise review, we will & Swen Hesse 123 early accurate diagnosis remains challenging. discuss the role of SPECT and [ I]FP-CIT in 1Università degli Studi di Milano, The estimated prevalence of PD is 0.5–1% in supporting the clinical diagnosis of PD and its Dipartimento di Fisiologia Umana, those aged 65–69 years and 1–3% in those aged differential diagnosis with ADP. Milano, Italy 2Centro per la Malattia di Parkinson e i ≥80 years [1]. Although the clinical diagnosis of Disturbi del Movimento, -

In Vitrocharacterization of Pittsburgh Compound-B Binding to Lewy Bodies
The Journal of Neuroscience, September 26, 2007 • 27(39):10365–10371 • 10365 Neurobiology of Disease In Vitro Characterization of Pittsburgh Compound-B Binding to Lewy Bodies Michelle T. Fodero-Tavoletti,1,2,4 David P. Smith,1,4 Catriona A. McLean,5 Paul A. Adlard,4 Kevin J. Barnham,1,2,4 Lisa E. Foster,1 Laura Leone,1 Keyla Perez,1,2,4 Mikhalina Corte´s,4 Janetta G. Culvenor,1,3,4 Qiao-Xin Li,1,4 Katrina M. Laughton,1,4 Christopher C. Rowe,6 Colin L. Masters,1,4 Roberto Cappai,1,2,4 and Victor L. Villemagne1,4,6 1Department of Pathology, 2Bio21 Institute, and 3Centre for Neuroscience, The University of Melbourne, Melbourne, Victoria 3010, Australia, 4The Mental Health Research Institute of Victoria, Parkville, Victoria 3052, Australia, 5Department of Anatomical Pathology, Alfred Hospital, Prahran, Victoria 3181, Australia, and 6Centre for PET, Austin Hospital, Heidelberg, Victoria 3084, Australia Dementia with Lewy bodies (DLB) is pathologically characterized by the presence of ␣-synuclein-containing Lewy bodies within the neocortical, limbic, and paralimbic regions. Like Alzheimer’s disease (AD), A plaques are also present in most DLB cases. The contri- bution of A to the development of DLB is unclear. [ 11C]-Pittsburgh compound B ([ 11C]-PIB) is a thioflavin-T derivative that has allowed in vivo A burden to be quantified using positron emission tomography (PET). [ 11C]-PIB PET studies have shown similar high cortical [ 11C]-PIB binding in AD and DLB subjects. To establish the potential binding of PIB to ␣-synuclein in DLB patients, we characterized the in vitro binding of PIB to recombinant human ␣-synuclein and DLB brain homogenates. -

DICOM Conformance Template
g GE Heathcare Technical Publications Direction 5507068-1EN (DOC1584283) Revision 1 DaTQUANT Application™ DICOM CONFORMANCE STATEMENT Copyright 2015 by General Electric Co. Do not duplicate g GE Heathcare LIST OF REVISIONS REV DATE DESCRIPTION PAGES APPR. 1 May 2015 Initial Release All M. Mesh DATQUANT APPLICATION GE Healthcare DICOM CONFORMANCE STATEMENT DIR 5507068-1EN (DOC1584283) REV 1 THIS PAGE LEFT INTENTIONALLY BLANK DATQUANT APPLICATION GE Healthcare DICOM CONFORMANCE STATEMENT DIR 5507068-1EN (DOC1584283) REV 1 CONFORMANCE STATEMENT OVERVIEW DaTQUANT application is an application that uses NM and CT images and creates NM, SC and MFSC images. Table 0.1 provides an overview of the network services supported by the DaTQUANT application. Table 0.1 – APPLICATION SOP Classes User of Object Creator of Instances Object Instances Transfer Secondary Capture Image Storage No Yes Multi-frame True Color Secondary Capture Image Storage No Yes Nuclear Medicine Image Storage Yes Yes Computerized Tomography Image Storage Yes No 4 DATQUANT APPLICATION GE Healthcare DICOM CONFORMANCE STATEMENT DIR 5507068-1EN (DOC1584283) REV 1 1. INTRODUCTION ............................................................................................................... 8 1.1 Overview ..................................................................................................................................................................... 8 1.2 Overall DICOM Conformance Statement Document Structure .......................................................................... -

Brain Imaging
Publications · Brochures Brain Imaging A Technologist’s Guide Produced with the kind Support of Editors Fragoso Costa, Pedro (Oldenburg) Santos, Andrea (Lisbon) Vidovič, Borut (Munich) Contributors Arbizu Lostao, Javier Pagani, Marco Barthel, Henryk Payoux, Pierre Boehm, Torsten Pepe, Giovanna Calapaquí-Terán, Adriana Peștean, Claudiu Delgado-Bolton, Roberto Sabri, Osama Garibotto, Valentina Sočan, Aljaž Grmek, Marko Sousa, Eva Hackett, Elizabeth Testanera, Giorgio Hoffmann, Karl Titus Tiepolt, Solveig Law, Ian van de Giessen, Elsmarieke Lucena, Filipa Vaz, Tânia Morbelli, Silvia Werner, Peter Contents Foreword 4 Introduction 5 Andrea Santos, Pedro Fragoso Costa Chapter 1 Anatomy, Physiology and Pathology 6 Elsmarieke van de Giessen, Silvia Morbelli and Pierre Payoux Chapter 2 Tracers for Brain Imaging 12 Aljaz Socan Chapter 3 SPECT and SPECT/CT in Oncological Brain Imaging (*) 26 Elizabeth C. Hackett Chapter 4 Imaging in Oncological Brain Diseases: PET/CT 33 EANM Giorgio Testanera and Giovanna Pepe Chapter 5 Imaging in Neurological and Vascular Brain Diseases (SPECT and SPECT/CT) 54 Filipa Lucena, Eva Sousa and Tânia F. Vaz Chapter 6 Imaging in Neurological and Vascular Brain Diseases (PET/CT) 72 Ian Law, Valentina Garibotto and Marco Pagani Chapter 7 PET/CT in Radiotherapy Planning of Brain Tumours 92 Roberto Delgado-Bolton, Adriana K. Calapaquí-Terán and Javier Arbizu Chapter 8 PET/MRI for Brain Imaging 100 Peter Werner, Torsten Boehm, Solveig Tiepolt, Henryk Barthel, Karl T. Hoffmann and Osama Sabri Chapter 9 Brain Death 110 Marko Grmek Chapter 10 Health Care in Patients with Neurological Disorders 116 Claudiu Peștean Imprint 126 n accordance with the Austrian Eco-Label for printed matters. -

Lettirs to Th Editor Radiation Injury from Interstitial Injection Of
DEPARTMENTS Lettirs to th Editor Radiation Injury from Interstitial Injection of measuring approximately 2 cm x 1 cm. Monitoring of the site Iodine-131-Iodocholesterol demonstrated retention of 131!(Fig. 2). On the basis of serial counts, the half-time was 5.5 days at the i.v. injection site. TO THE EDITOR: A 44-yr-oldman wasinvestigatedfor recur The absorbeddose deliveredto the overlyingskin cannot be rent Cushing's disease. An adrenal gland scan was initiated with precisely calculated because it has a very strong inverse depend injection of 34-MBq of ‘31I-iodocholesterol over a 5-mm interval. ence on the interstitial volume occupied by the injectate, and this Prior to injection, blood was withdrawn into the hub of the volume is not accurately known. The absorbed dose can be syringe to ensure correct i.v. placement. At the conclusion of the estimated by treating the interstitial volume occupied by the injection, the patient volunteered that the injection had been the injectate as a disk of the same area as the erythematous patch; least painful i.v. entry he had experienced. Seven days later, the thickness of this volume can be roughly estimated. The imaging failed to detect any radioactivity in the field of view volumeofdistributionwasassumedto remainconstantovertime centered on the adrenal glands. Monitoring of the injection site since the injectate is not water-soluble. The absorbed dose in this demonstrated essentially complete retention of the radiophar volume can be calculated by the method of Johns and Cun maceutical at the site. ningham (1). Because the model assumes no activity outside the The patient returned 13 days later (i.e., 20 days after the volume,the absorbeddose in the regionadjacentto this volume injection) to inquire about the tender pruritic and erythematous within the range of the beta particles (i.e., the skin) can be patch at the injection site at which time the photograph in Figure estimated to be halfthe dose inside the volume. -

Nuclear Pharmacy Quick Sample
12614-01_CH01-rev3.qxd 10/25/11 10:56 AM Page 1 CHAPTER 1 Radioisotopes Distribution for Not 1 12614-01_CH01-rev3.qxd 10/25/1110:56AMPage2 2 N TABLE 1-1 Radiopharmaceuticals Used in Nuclear Medicine UCLEAR Chemical Form and Typical Dosage P Distribution a b HARMACY Radionuclide Dosage Form Use (Adult ) Route Carbon C 11 Carbon monoxide Cardiac: Blood volume measurement 60–100 mCi Inhalation Carbon C 11 Flumazenil injection Brain: Benzodiazepine receptor imaging 20–30 mCi IV Q UICK Carbon C 11 Methionine injection Neoplastic disease evaluation in brain 10–20 mCi IV R Carbon C 11 forRaclopride injection Brain: Dopamine D2 receptor imaging 10–15 mCi IV EFERENCE Carbon C 11 Sodium acetate injection Cardiac: Marker of oxidative metabolism 12–40 mCi IV Carbon C 14 Urea Diagnosis of Helicobacter pylori infection 1 µCi PO Chromium Cr 51 Sodium chromate injection Labeling red blood cells (RBCs) for mea- 10–80 µCi IV suring RBC volume, survival, and splenic sequestration Cobalt Co 57 Cyanocobalamin capsules Diagnosis of pernicious anemia and 0.5 µCi PO Not defects of intestinal absorption Fluorine F 18 Fludeoxyglucose injection Glucose utilization in brain, cardiac, and 10–15 mCi IV neoplastic disease Fluorine F 18 Fluorodopa injection Dopamine neuronal decarboxylase activity 4–6 mCi IV in brain Fluorine F 18 Sodium fluoride injection Bone imaging 10 mCi IV Gallium Ga 67 Gallium citrate injection Hodgkin’s disease, lymphoma 8–10 mCi IV Acute inflammatory lesions 5 mCi IV Indium In 111 Capromab pendetide Metastatic imaging in patients with biopsy- -

Molecular Imaging in Alzheimer's Disease
CORE Metadata, citation and similar papers at core.ac.uk Provided by PubMed Central Nordberg Alzheimer’s Research & Therapy 2011, 3:34 http://alzres.com/content/3/6/34 REVIEW Molecular imaging in Alzheimer’s disease: new perspectives on biomarkers for early diagnosis and drug development Agneta Nordberg* Introduction Abstract Alzheimer’s disease (AD) is characterized by a slow Recent progress in molecular imaging has provided continued deterioration of cognitive processes. Th e fi rst new important knowledge for further understanding symptoms of episodic memory disturbances might be the time course of early pathological disease processes quite subtle. When the patient is assessed for memory in Alzheimer’s disease (AD). Positron emission problems the disease has most probably been ongoing in tomography (PET) amyloid beta (Aβ) tracers such as the brain for several years and has most probably induced Pittsburgh Compound B detect increasing deposition nonrepairable disturbances of important functional of fi brillar Aβ in the brain at the prodromal stages of neuronal networks and loops of the brain. It is a challenge AD, while the levels of fi brillar Aβ appear more stable to test whether some of these changes could be reversed at high levels in clinical AD. There is a need for PET or slowed down with early drug treatment. ligands to visualize smaller forms of Aβ, oligomeric Th e recent progress in AD research has provided new forms, in the brain and to understand how they knowledge for further understanding the pathology interact with synaptic activity and neurodegeneration. processes of AD that precede the onset of clinical disease The infl ammatory markers presently under by many years. -

In Vivo TSPO Signal and Neuroinflammation in Alzheimer's
cells Review In Vivo TSPO Signal and Neuroinflammation in Alzheimer’s Disease Benjamin B. Tournier 1,2,* , Stergios Tsartsalis 1 , Kelly Ceyzériat 1,3,4 , Valentina Garibotto 3 and Philippe Millet 1,2 1 Division of Adult Psychiatry, Department of Psychiatry, University Hospitals of Geneva, 1205 Geneva, Switzerland; [email protected] (S.T.); [email protected] (K.C.); [email protected] (P.M.) 2 Department of Psychiatry, University of Geneva, 1211 Geneva, Switzerland 3 Division of Nuclear Medicine and Molecular Imaging, Diagnostic Department, Geneva University and Geneva University Hospitals, 1205 Geneva, Switzerland; [email protected] 4 Division of Radiation Oncology, Department of Oncology, University Hospitals of Geneva, 1205 Geneva, Switzerland * Correspondence: [email protected]; Tel.: +41-22-305-5379 Received: 21 July 2020; Accepted: 18 August 2020; Published: 21 August 2020 Abstract: In the last decade, positron emission tomography (PET) and single-photon emission computed tomography (SPECT) in in vivo imaging has attempted to demonstrate the presence of neuroinflammatory reactions by measuring the 18 kDa translocator protein (TSPO) expression in many diseases of the central nervous system. We focus on two pathological conditions for which neuropathological studies have shown the presence of neuroinflammation, which translates in opposite in vivo expression of TSPO. Alzheimer’s disease has been the most widely assessed with more than forty preclinical and clinical studies, showing overall that TSPO is upregulated in this condition, despite differences in the topography of this increase, its time-course and the associated cell types. In the case of schizophrenia, a reduction of TSPO has instead been observed, though the evidence remains scarce and contradictory. -

Pharmaceuticals Appendix
)&f1y3X PHARMACEUTICAL APPENDIX TO THE HARMONIZED TARIFF SCHEDULE )&f1y3X PHARMACEUTICAL APPENDIX TO THE TARIFF SCHEDULE 3 Table 1. This table enumerates products described by International Non-proprietary Names (INN) which shall be entered free of duty under general note 13 to the tariff schedule. The Chemical Abstracts Service (CAS) registry numbers also set forth in this table are included to assist in the identification of the products concerned. For purposes of the tariff schedule, any references to a product enumerated in this table includes such product by whatever name known. Product CAS No. Product CAS No. ABAMECTIN 65195-55-3 ADAPALENE 106685-40-9 ABANOQUIL 90402-40-7 ADAPROLOL 101479-70-3 ABECARNIL 111841-85-1 ADEMETIONINE 17176-17-9 ABLUKAST 96566-25-5 ADENOSINE PHOSPHATE 61-19-8 ABUNIDAZOLE 91017-58-2 ADIBENDAN 100510-33-6 ACADESINE 2627-69-2 ADICILLIN 525-94-0 ACAMPROSATE 77337-76-9 ADIMOLOL 78459-19-5 ACAPRAZINE 55485-20-6 ADINAZOLAM 37115-32-5 ACARBOSE 56180-94-0 ADIPHENINE 64-95-9 ACEBROCHOL 514-50-1 ADIPIODONE 606-17-7 ACEBURIC ACID 26976-72-7 ADITEREN 56066-19-4 ACEBUTOLOL 37517-30-9 ADITOPRIME 56066-63-8 ACECAINIDE 32795-44-1 ADOSOPINE 88124-26-9 ACECARBROMAL 77-66-7 ADOZELESIN 110314-48-2 ACECLIDINE 827-61-2 ADRAFINIL 63547-13-7 ACECLOFENAC 89796-99-6 ADRENALONE 99-45-6 ACEDAPSONE 77-46-3 AFALANINE 2901-75-9 ACEDIASULFONE SODIUM 127-60-6 AFLOQUALONE 56287-74-2 ACEDOBEN 556-08-1 AFUROLOL 65776-67-2 ACEFLURANOL 80595-73-9 AGANODINE 86696-87-9 ACEFURTIAMINE 10072-48-7 AKLOMIDE 3011-89-0 ACEFYLLINE CLOFIBROL 70788-27-1 -

Qualification Opinion on Dopamine Transporter Imaging As an Enrichment Biomarker for Parkinson’S Disease Clinical Trials in Patients with Early Parkinsonian Symptoms
29 May 2018 EMA/CHMP/SAWP/765041/2017 Committee for Medicinal Products for Human Use (CHMP) Qualification opinion on dopamine transporter imaging as an enrichment biomarker for Parkinson’s disease clinical trials in patients with early Parkinsonian symptoms Draft agreed by Scientific Advice Working Party 26 October 2017 Adopted by CHMP for release for consultation 09 November 20171 Start of public consultation 24 January 20182 End of consultation (deadline for comments) 07 March 20183 Adoption by CHMP 26 April 2018 Biomarker, Molecular neuroimaging, Parkinson’s disease Keywords 1 Last day of relevant Committee meeting. 2 Date of publication on the EMA public website. 3 Last day of the month concerned. 30 Churchill Place ● Canary Wharf ● London E14 5EU ● United Kingdom Telephone +44 (0)20 3660 6000 Facsimile +44 (0)20 3660 5555 Send a question via our website www.ema.europa.eu/contact An agency of the European Union © European Medicines Agency, 2018. Reproduction is authorised provided the source is acknowledged. Executive summary Critical Path Global Ltd.’s Critical Path for Parkinson’s (CPP) is a multinational consortium of the Critical Path Institute supported by Parkinson’s UK and industry. This broad collaboration of pharmaceutical companies, government agencies, academic institutions, and charities aims to accelerate the development of therapies for Parkinson’s disease (PD). The CPP Imaging Biomarker team aims to achieve a qualification opinion by EMA Committee for Medical Products for Human Use (CHMP) for the use of low baseline Dopamine Transporter levels for subject enrichment in clinical trials in early stages of PD. This package reports the results of the Critical Path Global Ltd.