Nagaland District Team Members Block Type of HI Number Ms
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

NAGALAND Basic Facts
NAGALAND Basic Facts Nagaland-t2\ Basic Facts _ry20t8 CONTENTS GENERAT INFORMATION: 1. Nagaland Profile 6-7 2. Distribution of Population, Sex Ratio, Density, Literacy Rate 8 3. Altitudes of important towns/peaks 8-9 4. lmportant festivals and time of celebrations 9 5. Governors of Nagaland 10 5. Chief Ministers of Nagaland 10-11 7. Chief Secretaries of Nagaland II-12 8. General Election/President's Rule 12-13 9. AdministrativeHeadquartersinNagaland 13-18 10. f mportant routes with distance 18-24 DEPARTMENTS: 1. Agriculture 25-32 2. Animal Husbandry and Veterinary Services 32-35 3. Art & Culture 35-38 4. Border Afrairs 39-40 5. Cooperation 40-45 6. Department of Under Developed Areas (DUDA) 45-48 7. Economics & Statistics 49-52 8. Electricallnspectorate 52-53 9. Employment, Skill Development & Entrepren€urship 53-59 10. Environment, Forests & Climate Change 59-57 11. Evalua6on 67 t2. Excise & Prohibition 67-70 13. Finance 70-75 a. Taxes b, Treasuries & Accounts c. Nagaland State Lotteries 3 14. Fisheries 75-79 15. Food & Civil Supplies 79-81 16. Geology & Mining 81-85 17. Health & Family Welfare 85-98 18. Higher & Technical Education 98-106 19. Home 106-117 a, Departments under Commissioner, Nagaland. - District Administration - Village Guards Organisation - Civil Administration Works Division (CAWO) b. Civil Defence & Home Guards c. Fire & Emergency Services c. Nagaland State Disaster Management Authority d. Nagaland State Guest Houses. e. Narcotics f. Police g. Printing & Stationery h. Prisons i. Relief & Rehabilitation j. Sainik Welfare & Resettlement 20. Horticulture tl7-120 21. lndustries & Commerce 120-125 22. lnformation & Public Relations 125-127 23. -

Directory Establishment
DIRECTORY ESTABLISHMENT SECTOR :RURAL STATE : NAGALAND DISTRICT : Dimapur Year of start of Employment Sl No Name of Establishment Address / Telephone / Fax / E-mail Operation Class (1) (2) (3) (4) (5) NIC 2004 : 0121-Farming of cattle, sheep, goats, horses, asses, mules and hinnies; dairy farming [includes stud farming and the provision of feed lot services for such animals] 1 STATE CATTLE BREEDING FARM MEDZIPHEMA TOWN DISTRICT DIMAPUR NAGALAND PIN CODE: 797106, STD CODE: 03862, 1965 10 - 50 TEL NO: NA , FAX NO: NA, E-MAIL : N.A. NIC 2004 : 0122-Other animal farming; production of animal products n.e.c. 2 STATE CHICK REPARING CENTRE MEDZIPHEMA TOWN DISTRICT DIMAPUR NAGALAND PIN CODE: 797106, STD CODE: 03862, TEL 1965 10 - 50 NO: NA , FAX NO: NA, E-MAIL : N.A. NIC 2004 : 3610-Manufacture of furniture 3 MS MACHANIDED WOODEN FURNITURE DELAI ROAD NEW INDUSTRIAL ESTATE DISTT. DIMAPUR NAGALAND PIN CODE: 797112, STD 1998 10 - 50 UNIT CODE: NA , TEL NO: NA , FAX NO: NA, E-MAIL : N.A. 4 FURNITURE HOUSE LEMSENBA AO VILLAGE KASHIRAM AO SECTOR DISTT. DIMAPUR NAGALAND PIN CODE: 797112, STD CODE: 2002 10 - 50 NA , TEL NO: 332936, FAX NO: NA, E-MAIL : N.A. NIC 2004 : 5220-Retail sale of food, beverages and tobacco in specialized stores 5 VEGETABLE SHED PIPHEMA STATION DISTT. DIMAPUR NAGALAND PIN CODE: 797112, STD CODE: NA , TEL NO: NA 10 - 50 NA , FAX NO: NA, E-MAIL : N.A. NIC 2004 : 5239-Other retail sale in specialized stores 6 NAGALAND PLASTIC PRODUCT INDUSTRIAL ESTATE OLD COMPLEX DIMAPUR NAGALAND PIN CODE: 797112, STD CODE: NA , 1983 10 - 50 TEL NO: 226195, FAX NO: NA, E-MAIL : N.A. -
Sl.No. STATES/UTS DISTRICT SUB DISTRICT CATEGORY REPORTING UNITS NAME ADDRESS
Sl.No. STATES/UTS DISTRICT SUB DISTRICT CATEGORY REPORTING UNITS NAME ADDRESS 1 Andaman & Nicobar Islands Andamans Andamans Urban Stand Alone-Fixed ICTC BAMBOOFLAT CHC BAMBOOFLAT, SOUTH ANDAMAN 2 Andaman & Nicobar Islands Andamans Andamans Urban Stand Alone-Fixed ICTC BARATANG PHC BARATANG MIDDLE ANDAMAN 3 Andaman & Nicobar Islands Andamans Andamans Urban Stand Alone-Fixed ICTC DR. R.P HOSPITAL DR.R.P HOSPITAL, MAYABUNDER. 4 Andaman & Nicobar Islands Andamans Andamans Urban Stand Alone-Fixed ICTC G.B.PANT HOSPITAL G.B. PANT HOSPITAL, PORT BLAIR 5 Andaman & Nicobar Islands Andamans Andamans Urban Stand Alone-Fixed ICTC,CHC RANGAT CHC RANGAT,MIDDLE ANDAMAN 6 Andaman & Nicobar Islands Andamans Andamans Urban Stand Alone-Fixed ICTC,PHC HUT BAY PHC HUT BAY, LITTLE ANDAMAN 7 Andaman & Nicobar Islands Andamans Andamans Urban Stand Alone-Fixed ICTCS, PHC HAVELOCK PHC HAVELOCK, HAVELOCK 8 Andaman & Nicobar Islands Andamans Andamans Urban Stand Alone-Fixed ICTCS, PHC NEIL ISLANDS PHC NEIL ISLANDS, NEIL ISLANDS 9 Andaman & Nicobar Islands Andamans Andamans Urban Stand Alone-Fixed ICTCS,PHC GARACHARMA, DISTRICT HOSPITAL GARACHARMA 10 Andaman & Nicobar Islands Andamans Diglipur Stand Alone-Fixed ICTC DIGLIPUR CHC DIGLIPUR , NORTH & MIDDLE ANDAMAN 11 Andaman & Nicobar Islands Nicobars Car Nicobar Stand Alone-Fixed ICTC CAMPBELL BAY PHC CAMPBELL BAY, NICOBAR DISTRICT 12 Andaman & Nicobar Islands Nicobars Car Nicobar Stand Alone-Fixed ICTC CAR NICOBAR B.J.R HOSPITAL, CAR NICOBAR,NICOBAR 13 Andaman & Nicobar Islands Nicobars Car Nicobar Stand Alone-Fixed -

Government of Nagaland
Government of Nagaland Contents MESSAGES i FOREWORD viii ACKNOWLEDGEMENT x VISION STATEMENT xiv ACRONYMS xvii EXECUTIVE SUMMARY 1 1. INTRODUCTION AND OVERVIEW 5 2. AGRICULTURE AND ALLIED SECTORS 12 3. EmPLOYMENT SCENARIO IN NAGALAND 24 4. INDUSTRIES, INDUSTRIALIZATION, TRADE AND COMMERCE 31 5. INFRASTRUCTURE AND CONNECTIVITY 42 6. RURAL AND URBAN PERSPECTIVES 49 7. EDUCATION, HEALTH AND SOCIAL SERVICES 56 8. GENDER MAINSTREAMING 76 9. REGIONAL DISPARITIES 82 10. GOVERNANCE 93 11. FINANCING THE VISION 101 12. CONCLUSION 107 13. APPENDIX 117 RAJ BHAVAN Kohima-797001 December 03,2016 Message I value the efforts of the State Government in bringing out documentation on Nagaland Vision Document 2030. The Vision is a destination in the future and the ability to translate the Vision through Mission, is what matters. With Vision you can plan but with Mission you can implement. You need conviction to translate the steps needed to achieve the Vision. Almost every state or country has a Vision to propel the economy forward. We have seen and felt what it is like to have a big Vision and many in the developing world have been inspired to develop a Vision for their countries and have planned the way forward for their countries to progress. We have to be a vibrant tourist destination with good accommodation and other proper facilities to showcase our beautiful land and cultural richness. We need reformation in our education system, power and energy, roads and communications, etc. Our five Universities have to have dialogue with Trade & Commerce and introduce academic courses to create wealth out of Natural Resources with empowered skill education. -

Text Set Mkg 2040.Cdr
VISION MOKOKCHUNG 2040 A collaboration between the Mokokchung QQC Planning & Organising Committee and the Citizens of Mokokchung. Prepared by; Mayangnokcha Award Trust. Published by Mokokchung District Art & Culture Council (MDACC) On behalf of the people of Mokokchung 300 copies 2019 Printed at Longpok Offset Press, Mokokchung VISION MOKOKCHUNG 2040 Contents Acknowledgements Foreword Preface Executive Summary Introduction …………………………………..………….…………………. 5 Vision Mokokchung 2040 ……………………………………………... 7 Core Values of Vision Mokokchung 2040 ……………………... 8 The Foundation of Vision Mokokchung 2040 ……..…………... 9 Economic Development Model ………………………….…………… 13 Conclusion …………………………………………………………………….. 22 MAT Position Papers. Papers from Resource Persons. Papers from Department & NGOs. Transcribes. VISION MOKOKCHUNG 2040 Acknowledgements Over the years, there have been discussions and isolated papers or documents for Mokokchung in terms of development and related issues. There are also Plan documents for development of various sectors by different Government Departments. We also appreciate that the Concerned Citizens Forum of Mokokchung (CCFM), had earlier brought out documents on their Vision of Mokokchung and its development. But a comprehensive Vision document for Mokokchung in this format is perhaps the first of its kind, and for this, we wish to place on record our appreciation to the Mokokchung QQC Planning and Organising Committee and the District Administration for the initiative and unstinted support. Mokokchung District Art & Culture Council (MDACC), who did all the legwork, liaising and various arrangements. All India Radio (AIR) Mokokchung, for giving wide publicity and producing local programmes on the theme, social media group – I Love Mokokchung (ILM), and many more. Countless individuals have taken the trouble to give their personal views and opinions, well-wishers, and many more others whose contributions havebeen immense. -

Statisticai. Iiatvd Book of Nagaland 1984
STATISTICAI. IIATVD BOOK OF NAGALAND 1984 3 lO SONOMICS a STATISTICS IT OF SAC >-S Ih 1 M A j STATISTICAL HAND BOOK OF NAGALAND 1984 DIRECTORATE OF ECONOMICS & STATISTICS Government of Nagaland KOHIMA Sob. National Systems Unit, National Institute of Educational Pl^nmrr and AminifcrRtion 17-V .lA'^it'-ndo Maig.Ne-^Delhi-UOOl^ DOC. No............................ D a t e ........................................... .....................- r K F F \ C’ E Statistical Hanil Book ot Nagaland 1984 is a puhlication inrc'senting Statistical intormation on various aspects of Naga- lland EcoiKMTiy Data incorporated in this publication have Ibeem collected from various I'epartraents of the Govt by the lEctTinomics Sc Statistics Department and froni Official puhlica- ttioras as also from 'sources not published so far. It is hoped that ihe publication would be of some help tto thi public interested to have iv bird’s eve view of Nagaland, tto students of Economics, to Ihe Planners & others willing to piarticipate in Nagaland’s piogres^ and Development. I thank the variou > Departments and agencies which sui> polled the necessary information and rendered unstinted coope r-ation in preparing this hook. r thank Stui. H O. OUPTA, Joint Director, Economics Sk Statistics, but for whose special efforts it would not have bieen possible to bring out this issue. si> expeditiously. 1 also tlnank other officers of the Dej»tt and particularly Shri D R- F aul, inspector of Statistics, who shouldered the responsibility olf collection. compilation and proof readitig of the Bool< Suggestions for further improvement of the Hand Hook SiTP welctiine r»ated. Kohiina T.C.K LCITHA tine 15th Nov. -
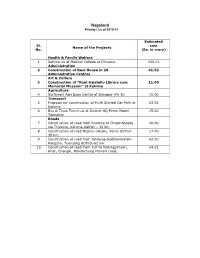
Nagaland Priority List of 2010-11
Nagaland Priority List of 2010-11 Estimated Sl. cost Name of the Projects No. (Rs. in crore) Health & Family Welfare 1 Setting up of Medical College at Dimapur 340.22 Administration 2 Construction of Rest House in 28 41.52 Administrative Centres Art & Culture 3 Construction of “Rani Gaidinliu Library cum 11.00 Memorial Museum” at Kohima Agriculture 4 Northeast Agri Expo Centre at Dimapur (Ph-II) 15.00 Transport 5 Proposal for construction of Multi Storied Car Park at 53.05 Kohima 6 Bus & Truck Terminus at District HQ Peren Model 15.00 Township Roads 7 Construction of road from Rusoma to Chiephobozou 40.00 via Thizama, Kohima district – 32 km 8 Construction of road Hebron-Jalukie, Peren district- 17.00 20 km 9 Construction of road from Jendang-Saddle-Noklak- 62.00 Pangsha, Tuensang district-62 km 10 Construction of road from Tuli to Molungyimsen, 44.01 Khar, Changki, Mokokchung Mariani road, Estimated Sl. cost Name of the Projects No. (Rs. in crore) Mokokchung District 51 km 11 Widening & Improvement of approach road from 10.00 Alongchen, Impur to Khar via Mopungchuket, Mokokchung district – 15 km 12 Construction of road Kohima to Leikie road junction 10.00 to Tepuiki to Barak, Inter-district road-10 km (MDR) Ph-III 13 Construction of road from Lukhami BRO junction to 90.00 Seyochung Tizu bridge on Satoi road, Khuza, Phughe, Chozouba State Highway junction, Inter- district road- 90 km (ODR) 14 Improvement & Upgradation of road from 5.40 Border Road to Changlangshu, Mon District-19 km 15 Construction of road from Pang to Phokphur via 12.44 -

Kohima : Nagaland HIGH SCHOOL LEAVING CERTIFICATE
Kohima : Nagaland (Provisional ) 30000 25000 20000 15000 No. of Students 10000 5000 0 Enrolled Appeared Passed HIGH SCHOOL LEAVING CERTIFICATE EXAMINATION 2020 Email : [email protected] Website : www.nbsenagaland.com NAGALAND BOARD OF SCHOOL EDUCATION, KOHIMA HIGH SCHOOL LEAVING CERTIFICATE EXAMINATION 2020 CONTENTS Page No. 1. Notification No. 7/2020 1-2 2. Abstract of the Result 3 3. Grade statistics 4-8 4. Merit list 9-12 5. Subject toppers 13-16 6. Awards and scholarships 17-19 8. Performance of schools 21-41 9. Notification No8/2020 42-138 (i) Kohima District : 42-59 (a) Koh-1 (Rüzhükhrie G.H.S.S, Kohima) 42-43 (b) Koh-2 (Baptist High,Kohima) 43-45 (c) Koh-3 (Mezhür H.S.School,Kohima) 45-47 (d) Koh-4 (MHB H.S.School,Kohima) 47-48 (e) Koh-5 (Christ King H.S.School,Kohima) 49 (f) Koh-6 (Don Bosco H.S.School,Kohima) 49-51 (g) Koh-7 (Chandmari H.S.School,Kohima) 51-52 (h) Koh-8 (Mount Sinai H.S.School,Kohima) 53-54 (i) Koh-9 (Grace H.S.School,Kohima) 54-55 (j) Vis (John G.H.S, Viswema) 55-57 (k) Tse (G.H.S.S,Tseminyu) 57-58 (l) Sec (G.H.S, Sechü) 58-59 (ii) Mokokchung District : 59-67 (a) Mok-1 (Mayangnokcha G.H.S.S, Mokokchung) 59-61 (b) Mok-2 (Queen Mary H.S.School, Mokokchung) 61-62 (c) Mok-3 (G.H.S,Dilong) 62-64 (d) Man (G.H.S,Mangkolemba) 64-65 (e) Tul (G.H.S.S,Tuli) 65-66 (f) Cha (R.C.Chiten Jamir Mem.G.H.S,Changtongya) 67 (iii) Tuensang District : 67-73 (a) Tue-1 (G.H.S.S,Tuensang) 67-68 (b) Tue-2 (G.H.S.S,Thangjam) 69 (c) Tue-3 (Baptist Thangyen School, Tuensang) 70-71 (d) Sha (G.H.S.School, Shamator) 71-72 (e) Nok (G.H.S.S,Noklak) 72 (f) Lkm (G.H.S.S,Longkhim) 73 (iv) Mon District : 74-81 (a) Mon-1 (G.H.S.S, Mon) 74 Sub-centre (Little Flower School, Mon) 75 (b) Mon-2 (Konjong H.S. -

Assessment of Training Needs for Banana Growers in Tuli Block, Mokokchung, Nagaland
INTERNATIONAL JOURNAL FOR INNOVATIVE RESEARCH IN MULTIDISCIPLINARY FIELD ISSN: 2455-0620 Volume - 7, Issue - 5, May – 2021 Monthly, Peer-Reviewed, Refereed, Indexed Journal with IC Value: 86.87 Impact Factor: 6.719 Received Date: 15/05/2021 Acceptance Date: 30/05/2021 Publication Date: 31/05/2021 ASSESSMENT OF TRAINING NEEDS FOR BANANA GROWERS IN TULI BLOCK, MOKOKCHUNG, NAGALAND 1. Sentinungshi , 2. Dr. Mary N. Odyuo 1Research Scholar. Department of Rural Development and Planning. Nagaland University. School of Agricultural Sciences and Rural Development. Medziphema Campus. 797106. 2Assistant Professor, Department of Rural Development and Planning. Nagaland University. School of Agricultural Sciences and Rural Development. Medziphema Campus. 797106. Email - [email protected] [email protected] th Abstract: Nagaland is the 16 state of India and is popularly known as the Land of Festivals. The study deals with the Training need assessment of banana cultivators in Tuli block under Mokokchung district hailing from the state of Nagaland. Structured interview schedule was prepared to collect the primary data of the respondents. Nagaland is a state of agriculture and more than half of the population depends on agricultural activities for livelihood. In Nagaland, Banana is popularly grown due to its favourable climatic condition and soil suitability and also a good source of healthy nutrition and a stable means for high income generation. Majority of the respondents, (68.33 %) had ‘medium’ level training needs towards banana cultivation. Where as, based on an overall rank obtained, the ‘training need’ was found to be highest in respect of pest and diseases management (I) followed by irrigation schedule(II), land preparation(III), nutrient management (IV), spacing (V), post harvest management technique (VI), harvesting (VII), seed and sowing (VIII) and intercultural operation (IX). -

Mouton Grammar Library a Grammar of Mongsen Ao
Mouton Grammar Library A Grammar of Mongsen Ao ≥ Mouton Grammar Library 39 Editors Georg Bossong Bernard Comrie Matthew Dryer Mouton de Gruyter Berlin · New York A Grammar of Mongsen Ao by A. R. Coupe Mouton de Gruyter Berlin · New York Mouton de Gruyter (formerly Mouton, The Hague) is a Division of Walter de Gruyter GmbH & Co. KG, Berlin. Țȍ Printed on acid-free paper which falls within the guidelines of the ANSI to ensure permanence and durability. Library of Congress Cataloging-in-Publication Data Coupe, A. R. (Alexander Robertson) A grammar of Mongsen Ao / by Alec Coupe. p. cm. Ϫ (Mouton grammar library ; 39) Includes bibliographical references and index. ISBN-13: 978-3-11-019088-5 (cloth : alk. paper) 1. Ao language Ϫ Grammar. I. Title. PL4001.A691C68 2007 4951.4Ϫdc22 2007024522 Bibliographic information published by the Deutsche Nationalbibliothek The Deutsche Nationalbibliothek lists this publication in the Deutsche Nationalbibliografie; detailed bibliographic data are available in the Internet at http://dnb.d-nb.de. ISBN 978-3-11-019088-5 ISSN 0933-7636 ” Copyright 2007 by Walter de Gruyter GmbH & Co. KG, D-10785 Berlin. All rights reserved, including those of translation into foreign languages. No part of this book may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopy, recording or any information storage and retrieval system, without permission in writing from the publisher. Printed in Germany. Acknowledgements This work was originally submitted at La Trobe University in December 2003 as a doctoral dissertation. Since then it has been through countless revisions and expansions as further insights into the structure of the grammar have been gained. -

Curriculum Vitae Dr
Curriculum Vitae Dr. Y. V. KRISHNAIAH, Ph.D. Associate Professor & Head, Department of Geography & Disaster Management, Tripura University (A Central University), (www.tripurauniv.ac.in) Suryamaninagar -799 022, Agartala, Tripura (West) TRIPURA STATE, INDIA. Mob. No. : 91-9436608205 Email : [email protected]; [email protected]; [email protected] Date of Birth : 01/06/1968 Nationality : Indian Marital Status : Married 1. Academic Qualification: M.Sc., Ph.D (Geography), M.Ed., M. Phil (Education) 2 (a). Total P.G. Teaching & Research Experience : 16 years (b). Academic and Administrative Experience in various levels attached. (c). Awards and Honours : 01 3. Total Number of Ph.D. Supervision a). Ph.D awarded : 03 b). Ph.D ongoing : 04 b). Ph.D Submitted : c). M.A/M.Sc (Geography) dissertations : 28 4. Total Number of Research Publications : 25 4a. Research paper published by Peer-Reviewed and UGC listed Journals : 20 4b. Book Chapters (published by National and International publishers) : 03 4c. Reference books (published by International Peer Reviewed publishers) : 02 5. Paper presentations in Seminars/Workshop etc., : 29 5a. Paper presentation at International level (within India) : 10 5b. Paper presentations at National level : 13 5c. Delivered Lecture at State/ Regional/University level : 06 6. National Seminar/Symposium/Workshops organized: 06 7. Participated in Trainings/Orientation/Refresher/Workshops: 09 8. Chaired Academic / Technical Sessions: 06 9. Academic works and Co-curricular activities: 20+ 10. Life Membership in various professional bodies and societies: 19 11. Reviewer : Elsevier Journals 1 1. Academic Qualifications Ph. D. in Geography, from Sri Krishnadevaraya University, Anantapuramu, Andhra Pradesh Title of the Ph.D thesis “Water Balance and Watershed Development of the Papagni River Basin, Andhra Pradesh, India Using Remote Sensing Technique” M. -

Segmentation, Unity, and a Church Divided: a Critical History of Churches in Nagaland, 1947-2017
Middlesex University Research Repository An open access repository of Middlesex University research http://eprints.mdx.ac.uk Jamir, Chongpongmeren (2019) Segmentation, unity, and a church divided: a critical history of churches in Nagaland, 1947-2017. PhD thesis, Middlesex University / Oxford Centre for Mission Studies. [Thesis] Final accepted version (with author’s formatting) This version is available at: https://eprints.mdx.ac.uk/27960/ Copyright: Middlesex University Research Repository makes the University’s research available electronically. Copyright and moral rights to this work are retained by the author and/or other copyright owners unless otherwise stated. The work is supplied on the understanding that any use for commercial gain is strictly forbidden. A copy may be downloaded for personal, non-commercial, research or study without prior permission and without charge. Works, including theses and research projects, may not be reproduced in any format or medium, or extensive quotations taken from them, or their content changed in any way, without first obtaining permission in writing from the copyright holder(s). They may not be sold or exploited commercially in any format or medium without the prior written permission of the copyright holder(s). Full bibliographic details must be given when referring to, or quoting from full items including the author’s name, the title of the work, publication details where relevant (place, publisher, date), pag- ination, and for theses or dissertations the awarding institution, the degree type awarded, and the date of the award. If you believe that any material held in the repository infringes copyright law, please contact the Repository Team at Middlesex University via the following email address: [email protected] The item will be removed from the repository while any claim is being investigated.