Investigation of Urine
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Catalase Test: Lab-3380
Standard Operating Procedure Subject Catalase Test Index Number Lab-3380 Section Laboratory Subsection Microbiology Category Departmental Contact Sarah Stoner Last Revised 9/18/2019 References Required document for Laboratory Accreditation by the College of American Pathologists (CAP), Centers for Medicare and Medicaid Services (CMS) and/or COLA. Applicable To Employees of Gundersen Health System Laboratory, Gundersen Tri-County, Gundersen St. Joseph, Gundersen Boscobel Hospital, and Gundersen Palmer Lutheran Hospital Laboratories. Detail PRINCIPLE: The breakdown of hydrogen peroxide into oxygen and water is mediated by the enzyme catalase. When a small amount of an organism that produces catalase is introduced into hydrogen peroxide, rapid elaboration of bubbles of oxygen, the gaseous product of the enzyme’s activity, is produced. CLINICAL SIGNIFICANCE: This test is used as an aid in distinguishing between Staphylococci and Streptococci. All members of the genus Staphylococcus are catalase (+), where as members of the genus Streptococcus are catalase (-). Listeria monocytogenes {catalase (+)} can be distinguished from beta-hemolytic streptococcus {catalase (-)}. Most Neisseria sp. are catalase (+). Catalase can also help distinguish Bacillus sp. {catalase (+)} from Clostridum sp. {mostly catalase (-)}. SPECIMEN: Isolates preferably grown on non-blood containing media not older than 24 hours old. REAGENTS AND MATERIALS: 1. 3% hydrogen peroxide (from stock bottle). Store 2o – 25o C. Do not freeze or overheat. Light sensitive, store in brown bottle. 2. Clean microscope slide or glass test tube 3. Wooden applicator stick EQUIPMENT/INSTRUMENTATION: N/A QUALITY CONTROL: Each new lot and shipment or once a month, perform QC on reagent with stock organisms of S aureus (positive) and Beta strep group A (negative). -
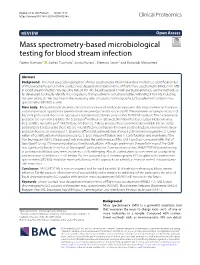
Mass Spectrometry-Based Microbiological Testing for Blood
Nomura et al. Clin Proteom (2020) 17:14 https://doi.org/10.1186/s12014-020-09278-7 Clinical Proteomics REVIEW Open Access Mass spectrometry-based microbiological testing for blood stream infection Fumio Nomura1* , Sachio Tsuchida1, Syota Murata2, Mamoru Satoh1 and Kazuyuki Matsushita2 Abstract Background: The most successful application of mass spectrometry (MS) in laboratory medicine is identifcation (ID) of microorganisms using matrix-assisted laser desorption ionization–time of fight mass spectrometry (MALDI-TOF MS) in blood stream infection. We describe MALDI-TOF MS-based bacterial ID with particular emphasis on the methods so far developed to directly identify microorganisms from positive blood culture bottles with MALDI-TOF MS including our own protocols. We touch upon the increasing roles of Liquid chromatography (LC) coupled with tandem mass spectrometry (MS/MS) as well. Main body: Because blood culture bottles contain a variety of nonbacterial proteins that may interfere with analysis and interpretation, appropriate pretreatments are prerequisites for successful ID. Pretreatments include purifcation of bacterial pellets and short-term subcultures to form microcolonies prior to MALDI-TOF MS analysis. Three commercial protocols are currently available: the Sepsityper® kit (Bruker Daltonics), the Vitek MS blood culture kit (bioMerieux, Inc.), and the rapid BACpro® II kit (Nittobo Medical Co., Tokyo). Because these commercially available kits are costly and bacterial ID rates using these kits are not satisfactory, particularly for Gram-positive bacteria, various home-brew protocols have been developed: 1. Stepwise diferential sedimentation of blood cells and microorganisms, 2. Combi- nation of centrifugation and lysis procedures, 3. Lysis-vacuum fltration, and 4. Centrifugation and membrane fltra- tion technique (CMFT). -

Helicobacter Pylori Infections: Culture from Stomach Biopsy, Rapid Urease Test (Cutest®), and Histologic Examination of Gastric Biopsy
Available online at www.annclinlabsci.org 148 Annals of Clinical & Laboratory Science, vol. 45, no. 2, 2015 An Efficiency Comparison between Three Invasive Methods for the Diagnosis of Helicobacter pylori Infections: Culture from Stomach Biopsy, Rapid Urease Test (CUTest®), and Histologic Examination of Gastric Biopsy Avi Peretz1, Avi On 2, Anna Koifman1, Diana Brodsky1, Natlya Isakovich1, Tatyana Glyatman1, and Maya Paritsky3 1Clinical Microbiology Laboratory, 2Pediatric Gastrointestinal Unit, and 3Gastrointestinal Unit, Baruch Padeh Medical Center, Poria, affiliated to the Faculty of Medicine, Bar Ilan University, Galille, Israel Abstract. Background. Helicobacter pylori is one of the most prevalent pathogenic bacteria in the world, and humans are its principal reservoir. There are several available methods to diagnose H. pylori infection. Disagreement exists as to the best and most efficient method for diagnosis. Methods. In this paper, we report the results of a comparison between three invasive methods for H. pylori diagnosis among 193 pa- tients: culture, biopsy for histologic examination, and rapid urease test (CUTest®). Results. We found that all three methods have a high sensitivity and specificity for the diagnosis of infections caused by H. pylori. However, the culture method, which is not used routinely, also showed high sensitivity, probably due to biopsies’ seeding within 30 minutes, using warm culture media, non-selective media, and longer incuba- tion. Conclusions. Although not a routine test, culture from biopsy can be meaningful in identification of antibiotic-resistant strains of H. pylori and should therefore be considered a useful diagnostic tool. Keywords: Helicobacter pylor, Culture, Urease test, Gastric biopsy. Introduction Helicobacter pylori is one of the most prevalent Recently, a close association was found between H. -
Gram Stain Workshop for the Laboratory Generalist
Gram Stain Workshop for the Laboratory Generalist Karen Stiles, SM(ASCP)CM State Training Coordinator Assistant Chemical Terrorism Coordinator Nebraska Public Health Laboratory 402-559-3590 [email protected] 1 GRAM STAIN OBJECTIVES: Upon completion, the participant will be able to: 1. Explain the principle of the Gram stain procedure, including what elements can affect staining results 2. Correlate the most common pathogens with positive Gram stains from blood cultures and direct specimen sterile body fluid smears 3. Perform and interpret Grams stains 2 Purpose of Gram Stain Classify bacteria based on form, size, cellular morphology, Gram reaction Assess quality of specimen Identify specific infectious agent from morphology and Gram reaction Correlation with culture growth Correlation with culture-independent methodologist Guide presumptive antibiotic therapy 3 Principle of Gram Stain Cell wall composition Gram positive – think peptidoglycan layer with teichoic acid Gram negative – high in lipid content Basic premise Crystal Violet – all cells take up primary stain Gram’s iodine – mordant to form complex Decolorizer – mixture of acetone and alcohol Dehydrate lipids in Gram negative cell walls, wash out complex Gram positive cells resistant, retain stain complex Safranin - counterstain 4 Gram negative cells take up counterstain Preparation of Samples Specimen Type Preparation CSF/sterile body fluids Cyto/Centrifuge Blood Culture Broth Drop to slide Tissue Touch prep Tissue homogenate Drop to slide Swabbed material Roll -

Diagnostic Microbiology 170-1 Provides an Overview of the Most Commonly Used Stains
PART Infectious Diseases XVII Section cells is used to judge the suitability of a specimen for culture. For 1 example, the presence of more than 10 epithelial cells per low-power field in a sputum specimen is highly suggestive of a specimen contami- General Considerations nated with oral secretions. In addition, a preliminary assessment of the etiologic agent can be made based upon the morphology (e.g., cocci vs rods) and stain reaction (e.g., Gram-positive isolates are purple; Gram- negative are red) of the microorganisms. However, a negative Gram stain does not rule out infection as 104 to 105 microorganisms per mL Chapter 170 in the specimen are required for detection by this method. In addition to the Gram stain, many other stains are used in micro- biology, both to detect organisms and to help infer their identity. Table Diagnostic Microbiology 170-1 provides an overview of the most commonly used stains. Carey-Ann D. Burnham and Isolation and Identification Gregory A. Storch The approach to isolation of microorganisms in a clinical specimen will vary depending on the body site and pathogen suspected. For body sites that are usually sterile, such as cerebrospinal fluid, nutrient-rich media such as sheep blood agar and chocolate agar are used to aid in Laboratory evidence to support the diagnosis of an infectious disease the recovery of fastidious pathogens. In contrast, stool specimens may be based on 1 or more of the following: direct examination of contain abundant amounts of commensal bacteria and thus to isolate specimens using microscopic or antigen detection techniques, isola- pathogens, selective and differential media must be used. -

Identification and Antimicrobial Susceptibility Testing of Anaerobic
antibiotics Review Identification and Antimicrobial Susceptibility Testing of Anaerobic Bacteria: Rubik’s Cube of Clinical Microbiology? Márió Gajdács 1,*, Gabriella Spengler 1 and Edit Urbán 2 1 Department of Medical Microbiology and Immunobiology, Faculty of Medicine, University of Szeged, 6720 Szeged, Hungary; [email protected] 2 Institute of Clinical Microbiology, Faculty of Medicine, University of Szeged, 6725 Szeged, Hungary; [email protected] * Correspondence: [email protected]; Tel.: +36-62-342-843 Academic Editor: Leonard Amaral Received: 28 September 2017; Accepted: 3 November 2017; Published: 7 November 2017 Abstract: Anaerobic bacteria have pivotal roles in the microbiota of humans and they are significant infectious agents involved in many pathological processes, both in immunocompetent and immunocompromised individuals. Their isolation, cultivation and correct identification differs significantly from the workup of aerobic species, although the use of new technologies (e.g., matrix-assisted laser desorption/ionization time-of-flight mass spectrometry, whole genome sequencing) changed anaerobic diagnostics dramatically. In the past, antimicrobial susceptibility of these microorganisms showed predictable patterns and empirical therapy could be safely administered but recently a steady and clear increase in the resistance for several important drugs (β-lactams, clindamycin) has been observed worldwide. For this reason, antimicrobial susceptibility testing of anaerobic isolates for surveillance -

Use of Matrix-Assisted Laser Desorption/Ionisation-Time of Flight Mass Spectrometry Analyser in a Diagnostic Microbiology Laboratory in a Developing Country
African Journal of Laboratory Medicine ISSN: (Online) 2225-2010, (Print) 2225-2002 Page 1 of 6 Original Research Use of matrix-assisted laser desorption/ionisation-time of flight mass spectrometry analyser in a diagnostic microbiology laboratory in a developing country Authors: Background: Rapid and accurate identification of pathogens is of utmost importance for 1 Atang Bulane management of patients. Current identification relies on conventional phenotypic methods Anwar Hoosen1 which are time consuming. Matrix-assisted laser desorption/ionisation-time of flight mass Affiliations: spectrometry (MALDI-TOF MS) is based on proteomic profiling and allows for rapid 1Department of Medical identification of pathogens. Microbiology & Virology, University of the Free State, Objective: We compared MALDI-TOF MS against two commercial systems, MicroScan Bloemfontein, South Africa Walkaway and VITEK 2 MS. Corresponding author: Methods: Over a three-month period from July 2013 to September 2013, a total of 227 bacteria Atang Bulane, and yeasts were collected from an academic microbiology laboratory (N = 121; 87 Gram- [email protected] negatives, seven Gram-positives, 27 yeasts) and other laboratories (N = 106; 35 Gram-negatives, Dates: 34 Gram-positives, 37 yeasts). Sixty-five positive blood cultures were initially processed with Received: 07 Dec. 2016 Bruker Sepsityper kit for direct identification. Accepted: 30 June 2017 Published: 08 Dec. 2017 Results: From the 65 blood culture bottles, four grew more than one bacterial pathogen and MALDI-TOF MS identified only one isolate. The blood cultures yielded 21 Gram-negatives, 43 How to cite this article: Bulane A, Hoosen A. Use of Gram-positives and one Candida. There were 21 Escherirchia coli isolates which were reported matrix-assisted laser by the MALDI-TOF MS as E. -

BBL MR-VP Broth
BBL™ MR-VP Broth ! L007474 • Rev. 06 • May 2006 QUALITY CONTROL PROCEDURES I INTRODUCTION MR-VP Broth is a medium which aids in the differentiation of bacteria by means of the methyl red and Voges-Proskauer reactions. II PERFORMANCE TEST PROCEDURE 1. Inoculate representative samples with the cultures listed below. a. Inoculate duplicate tubes using a 0.01 mL calibrated loop with 10-1 dilutions of 18- to 24-h Trypticase™ Soy Broth cultures. b. Incubate tubes with loosened caps at 35 ± 2°C in an aerobic atmosphere. 2. Examination of tubes for growth and determination of reactions. a. Voges-Proskauer Reaction—Read tubes after 18–24 h of incubation for growth and reaction. To perform the reaction proceed as follows (using one half of the duplicate tubes): 1) Add 0.6 mL of alpha-naphthol solution (see Barritt reagent, below) to each tube including uninoculated controls. 2) Add 0.2 mL potassium hydroxide solution to each tube including uninoculated controls. 3) Vortex each tube for several seconds. 4) Positive reactions occur at once or within 5 min. 5) Read for the development of a faint pink to deep red color. The appearance of a pink to red color indicates the presence of acetylmethylcarbinol. b. Methyl Red Reaction—Read the second half of the duplicate tubes after 5 days incubation for growth and reaction. Proceed as follows: 1) Add five drops of the methyl red indicator solution (see “Test Procedure”) to the test media (including the uninoculated controls). 2) Read the reactions immediately. The appearance of a distinct red color indicates the presence of a high degree of acidity and is regarded as a positive reaction. -

Best Practice No 167 the Laboratory Diagnosis of Urinary Tract Infection
J Clin Pathol 2001;54:911–919 911 Best Practice No 167 J Clin Pathol: first published as on 1 December 2001. Downloaded from The laboratory diagnosis of urinary tract infection J C Graham, A Galloway Abstract women develop a UTI during their lifetime; the Urinary tract infection is common, and it incidence increases at puberty and remains is not surprising that urine specimens high throughout adult life, only after the age of make up a large proportion of those sam- 50 years is a similar incidence seen in males. ples submitted to the routine diagnostic UTI accounts for approximately 23% of all laboratory. Many of these specimens will hospital acquired infections.2 Although the show no evidence of infection and several incidence of infection is high, most specimens methods can be used to screen out received will show no evidence of infection and negative samples. Those that grow bacte- several methods have been developed to screen ria need to be carefully assessed to out negative samples to minimise expense and quantify the degree of bacteriuria and improve turnaround times. These will also be hence clinical relevance. To influence reviewed. treatment, a final report should be pro- Most infections at all ages are the result of duced within 24 hours of specimen re- enteric bacteria, especially Escherichia coli, ceipt, with turnaround times continuously which colonise the perineum and then ascend monitored. Much work needs to be done to the urethra to multiply and infect the bladder, http://jcp.bmj.com/ determine the cost eVectiveness involved kidney, and adjacent structures.3 The most in processing urine specimens and the common site of infection is the bladder. -

BD BBL™ CIN Agar, Pkg
BBL™ CIN Agar L007366 • Rev. 07 • November 2015 QUALITY CONTROL PROCEDURES (Optional) I INTRODUCTION CIN (cefsulodin-Irgasan™-novobiocin) Agar is used for the selective isolation of Yersinia enterocolitica. II PERFORMANCE TEST PROCEDURE 1. Inoculate representative samples with the cultures listed below. a. Streak the plates for isolation using 5-h Trypticase™ Soy Broth cultures diluted to yield 103–104 CFU/plate. b. Incubate plates at 25 ± 2 °C in an aerobic atmosphere. c. Include Trypticase Soy Agar with 5% Sheep Blood (TSA II) plates as nonselective controls for all organisms. 2. Examine plates after 18–24 and 48 h for amount of growth, pigmentation, colony size, and selectivity. 3. Expected Results CLSI Organisms ATCC® Recovery *Yersinia enterocolitica 9610 Growth; deep red center, transparent border (bull’s-eye) *Escherichia coli 25922 Inhibition (partial to complete) *Pseudomonas aeruginosa 27853 Inhibition (partial to complete) *Enterococcus faecalis 29212 Inhibition (partial to complete) Additional Organisms Yersinia enterocolitica 49397 Fair to heavy growth. Colonies flat with confined deep-red center (bull’s-eye) surrounded by a transparent border. Proteus mirabilis 12453 Inhibition (partial to complete) *Recommended organism strain for User Quality Control. III ADDITIONAL QUALITY CONTROL 1. Examine plates as described under “Product Deterioration.” 2. Visually examine representative plates to assure that any existing physical defects will not interfere with use. 3. Determine the pH potentiometrically at room temperature for adherence to the specification of 7.4 ± 0.2. 4. Note the firmness of plates during the inoculation procedure. 5. Incubate uninoculated representative plates aerobically at 35 ± 2 °C for 72 h and examine for microbial contamination. -

MALDI-TOF MS in the Clinical Microbiology Laboratory MALDI-TOF MS No Laboratório De Microbiologia Clínica
UPDATE papeR J Bras Patol Med Lab, v. 49, n. 4, p. 256-259, agosto 2013 MALDI-TOF MS in the clinical microbiology laboratory MALDI-TOF MS no laboratório de microbiologia clínica Marcelo Jenne Mimica1; Marines Dalla Valle Martino2; Jacyr Pasternak3 ABSTRACT Traditional methods for microbial identification are often very laborious and time consuming. A new mass spectrometry based technique, matrix-assisted laser desorption ionization-time of flight (MALDI-TOF), has been described as a rapid, practical and low-cost method for this purpose. In this article, primary and possible future applications of this tool are briefly discussed. Key words: MALDI-TOF; microbial diagnostics; microbial identification; mass spectrometry. INTRODUCTION Most studies with this method included strains that had previously been isolated in culture. Nevertheless, some reports Phenotypic methods for bacterial identification, including the admit the possibility of diagnosis directly from clinical specimens, Gram group, growth characteristics in culture and biochemical especially blood samples, which would represent a breakthrough tests, remain the tests of choice for performing microbiological in terms of even faster results(3). analysis in most clinical laboratories worldwide. Although these are traditional methods, they provide answers to the clinician METHOD that are often time consuming, reaching several days in the case of fastidious microorganisms(3), hence the need for faster and accurate diagnostic tools. Some molecular techniques such as There are two commercially available systems that have been real-time polymerase chain reaction (RT-PCR), sequencing and incorporated in the microbiology area by traditional companies. microarrays have been successfully deployed in identification, but The first one is MS Vitek (bioMerieux), formerly Shimadzu. -

Landscape of Diagnostics Against Antibacterial Resistance, Gaps And
LANDSCAPE OF DIAGNOSTICS AGAINST ANTIBACTERIAL RESISTANCE, GAPS AND PRIORITIES LANDSCAPE OF DIAGNOSTICS AGAINST ANTIBACTERIAL RESISTANCE, GAPS AND PRIORITIES Landscape of diagnostics against antibacterial resistance, gaps and priorities ISBN 978-92-4-151628-0 © World Health Organization 2019 Some rights reserved. This work is available under the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 IGO licence (CC BY‑NC‑SA 3.0 IGO; https://creativecommons.org/licenses/by-nc-sa/3.0/igo). Under the terms of this licence, you may copy, redistribute and adapt the work for non-commercial purposes, provided the work is appropriately cited, as indicated below. In any use of this work, there should be no suggestion that WHO endorses any specific organization, products or services. The use of the WHO logo is not permitted. If you adapt the work, then you must license your work under the same or equivalent Creative Commons licence. If you create a translation of this work, you should add the following disclaimer along with the suggested citation: “This translation was not created by the World Health Organization (WHO). WHO is not responsible for the content or accuracy of this translation. The original English edition shall be the binding and authentic edition”. Any mediation relating to disputes arising under the licence shall be conducted in accordance with the mediation rules of the World Intellectual Property Organization. Suggested citation. Landscape of diagnostics against antibacterial resistance, gaps and priorities. Geneva: World Health Organization; 2019. Licence: CC BY‑NC‑SA 3.0 IGO. Cataloguing-in-Publication (CIP) data. CIP data are available at http://apps.who.int/iris.