Prevalence, Risk Factors, and Medical Costs of Chlamydia Trachomatis
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Mineral Industry of China in 2016
2016 Minerals Yearbook CHINA [ADVANCE RELEASE] U.S. Department of the Interior December 2018 U.S. Geological Survey The Mineral Industry of China By Sean Xun In China, unprecedented economic growth since the late of the country’s total nonagricultural employment. In 2016, 20th century had resulted in large increases in the country’s the total investment in fixed assets (excluding that by rural production of and demand for mineral commodities. These households; see reference at the end of the paragraph for a changes were dominating factors in the development of the detailed definition) was $8.78 trillion, of which $2.72 trillion global mineral industry during the past two decades. In more was invested in the manufacturing sector and $149 billion was recent years, owing to the country’s economic slowdown invested in the mining sector (National Bureau of Statistics of and to stricter environmental regulations in place by the China, 2017b, sec. 3–1, 3–3, 3–6, 4–5, 10–6). Government since late 2012, the mineral industry in China had In 2016, the foreign direct investment (FDI) actually used faced some challenges, such as underutilization of production in China was $126 billion, which was the same as in 2015. capacity, slow demand growth, and low profitability. To In 2016, about 0.08% of the FDI was directed to the mining address these challenges, the Government had implemented sector compared with 0.2% in 2015, and 27% was directed to policies of capacity control (to restrict the addition of new the manufacturing sector compared with 31% in 2015. -

Spatial Optimization and Mode Analysis of Primary Industry Structure in Yellow River Delta Ping Yang, Yujian Yang
Spatial Optimization and Mode Analysis of Primary Industry Structure in Yellow River Delta Ping Yang, Yujian Yang To cite this version: Ping Yang, Yujian Yang. Spatial Optimization and Mode Analysis of Primary Industry Structure in Yellow River Delta. 6th Computer and Computing Technologies in Agriculture (CCTA), Oct 2012, Zhangjiajie, China. pp.150-160, 10.1007/978-3-642-36137-1_19. hal-01348227 HAL Id: hal-01348227 https://hal.inria.fr/hal-01348227 Submitted on 22 Jul 2016 HAL is a multi-disciplinary open access L’archive ouverte pluridisciplinaire HAL, est archive for the deposit and dissemination of sci- destinée au dépôt et à la diffusion de documents entific research documents, whether they are pub- scientifiques de niveau recherche, publiés ou non, lished or not. The documents may come from émanant des établissements d’enseignement et de teaching and research institutions in France or recherche français ou étrangers, des laboratoires abroad, or from public or private research centers. publics ou privés. Distributed under a Creative Commons Attribution| 4.0 International License Spatial Optimization and Mode Analysis of Primary Industry Structure in Yellow River Delta Ping Yang, Yujian Yang* 1 The institute of sustainable development of Shandong Agricultural Science Academy 2S & T Information Engineering Technology Center of Shandong Academy of Agricultural Science, Information center of agronomy College of Shandong University *Corresponding author, Address: S&T Information Engineering Research Center, Number 202 Gongye North Road, -

2019年第3季度在韩国注册的中国水产企业名单the List of Chinese
2019年第3季度在韩国注册的中国水产企业名单 The List of Chinese Registered Fishery Processing Establishments Export to Korea (Total 1347 , the third quarter of 2019,updated on 25 June, 2019) No. Est.No. 企业名称(中文) Est.Name 企业地址(中文) Est.Address 产品(Products) 北京市朝阳区崔各庄乡 The 23rd floor Sanyuan Property Jingmi Road 北京中洋环球金枪鱼有 1 1100/02010 Beijing Zhongyang Global Tuna Co.,Ltd 东辛店村京密路三元物 Dongxindian Village Cuigezhuang TownChaoyang Fishery Products 限公司 业院内23号楼 District Beijng 五洋海产(天津)有限 天津市塘沽区东江路 2 1200/02004 Ocean Products (Tian.Jin) Co., Ltd Dongjiang Road No.3849 Tanggu Tianjin Fishery Products 公司 3849号 欧盛实业(天津)有限 天津经济技术开发区渤 No.5, Bohai Road, Tianjin Economic & Technological 3 1200/02019 Ocean (Tianjin) Corporation Ltd. Fishery Products 公司 海路5号 Development Area, Tianjin 天津市颖明海湾食品有 天津市滨海新区中心渔 No.221 Yuehai RD., Binhai New Area Of The City 4 1200/02028 Tianjin Smart Gulf Foodstuffs Co.,Ltd. Fishery Products 限公司 港经济区悦海路221号 Center Fishing Port Economic Zone, Tianjin, China 天津市塘沽区海华水产 Tianjin Tanggu District Haihua Fishery Products Food 天津市塘沽区北塘镇水 No. 9, Shuichan Road, Beitang Town, Tanggu District, 5 1200/02048 Fishery Products 食品有限公司 Co., Ltd. 产路9号 Tianjin 天津百迅达进出口贸易 天津市津南区双桥河镇 South Dongnigu Village, Shuangqiaohe Town, Jinnan 6 1200/02063 Tianjin baixunda import and export trade Co., Ltd Fishery Products 有限公司 东泥沽村南 District, Tianjin, China 昌黎县筑鑫实业有限公 秦皇岛市昌黎县新开口 Economic Development Zone Xinkaikou Changli 7 1300/02228 Changli Zhuxin Enterprises Co., Ltd. Fishery Products 司 经济开发区 County Qinhuangdao 抚宁县渤远水产品有限 秦皇岛市抚宁县台营镇 Yegezhuang village taiying town funing county 8 1300/02229 Funing county boyuan aquatic products co.,ltd Fishery Products 公司 埜各庄村 Qinhuangdao city Hebei province 秦皇岛市江鑫水产冷冻 河北省秦皇岛北戴河新 Nandaihe Second District,Beidaihe New 9 1300/02236 Qinhuangdao Jiangxin Aquatic Food Products Co., Ltd. -

Fiscal Reform and Land Public Finance: Zouping County In
Fiscal Reform and Land Public 7 Finance: Zouping County in National Context h SUSAN H. WHITING and has become a key source of fi scal revenue for local governments in China. LAs the value of land has increased with urbanization and economic development, local governments have sought to exploit their control over land in order to gener- ate both on- and off - budget revenue. Scholars and policy makers have come to refer to this phenomenon as “land public fi nance.” Th is chapter argues that land public fi nance is in large part an outgrowth of trends in central- local fi scal relations. During the course of China’s transition from a planned to a market economy, central- local fi scal relations have undergone a series of fundamental reforms. Cur- rent challenges grow out of a number of features of the Chinese po liti cal economy, the most important of which is the mismatch between the allocation of revenues and the assignment of expenditure responsibilities across levels of government. Local governments— county governments in particular— oft en lack adequate rev- enues within the formal fi scal system to fi nance the wide range of public goods and ser vices they are mandated by higher levels to provide. Th e mismatch between revenues and expenditure responsibilities leads to heavy reliance on intergovern- mental fi scal transfers that, nonetheless, have not yet eff ectively redressed revenue inadequacy or the high levels of in e qual ity that have emerged in the context of economic reform. Th is fi scal gap drives additional problems, including the growth of hidden government debts and off - budget funds at the local level. -

Cereal Series/Protein Series Jiangxi Cowin Food Co., Ltd. Huangjindui
产品总称 委托方名称(英) 申请地址(英) Huangjindui Industrial Park, Shanggao County, Yichun City, Jiangxi Province, Cereal Series/Protein Series Jiangxi Cowin Food Co., Ltd. China Folic acid/D-calcium Pantothenate/Thiamine Mononitrate/Thiamine East of Huangdian Village (West of Tongxingfengan), Kenli Town, Kenli County, Hydrochloride/Riboflavin/Beta Alanine/Pyridoxine Xinfa Pharmaceutical Co., Ltd. Dongying City, Shandong Province, 257500, China Hydrochloride/Sucralose/Dexpanthenol LMZ Herbal Toothpaste Liuzhou LMZ Co.,Ltd. No.282 Donghuan Road,Liuzhou City,Guangxi,China Flavor/Seasoning Hubei Handyware Food Biotech Co.,Ltd. 6 Dongdi Road, Xiantao City, Hubei Province, China SODIUM CARBOXYMETHYL CELLULOSE(CMC) ANQIU EAGLE CELLULOSE CO., LTD Xinbingmaying Village, Linghe Town, Anqiu City, Weifang City, Shandong Province No. 569, Yingerle Road, Economic Development Zone, Qingyun County, Dezhou, biscuit Shandong Yingerle Hwa Tai Food Industry Co., Ltd Shandong, China (Mainland) Maltose, Malt Extract, Dry Malt Extract, Barley Extract Guangzhou Heliyuan Foodstuff Co.,LTD Mache Village, Shitan Town, Zengcheng, Guangzhou,Guangdong,China No.3, Xinxing Road, Wuqing Development Area, Tianjin Hi-tech Industrial Park, Non-Dairy Whip Topping\PREMIX Rich Bakery Products(Tianjin)Co.,Ltd. Tianjin, China. Edible oils and fats / Filling of foods/Milk Beverages TIANJIN YOSHIYOSHI FOOD CO., LTD. No. 52 Bohai Road, TEDA, Tianjin, China Solid beverage/Milk tea mate(Non dairy creamer)/Flavored 2nd phase of Diqiuhuanpo, Economic Development Zone, Deqing County, Huzhou Zhejiang Qiyiniao Biological Technology Co., Ltd. concentrated beverage/ Fruit jam/Bubble jam City, Zhejiang Province, P.R. China Solid beverage/Flavored concentrated beverage/Concentrated juice/ Hangzhou Jiahe Food Co.,Ltd No.5 Yaojia Road Gouzhuang Liangzhu Street Yuhang District Hangzhou Fruit Jam Production of Hydrolyzed Vegetable Protein Powder/Caramel Color/Red Fermented Rice Powder/Monascus Red Color/Monascus Yellow Shandong Zhonghui Biotechnology Co., Ltd. -

Table of Codes for Each Court of Each Level
Table of Codes for Each Court of Each Level Corresponding Type Chinese Court Region Court Name Administrative Name Code Code Area Supreme People’s Court 最高人民法院 最高法 Higher People's Court of 北京市高级人民 Beijing 京 110000 1 Beijing Municipality 法院 Municipality No. 1 Intermediate People's 北京市第一中级 京 01 2 Court of Beijing Municipality 人民法院 Shijingshan Shijingshan District People’s 北京市石景山区 京 0107 110107 District of Beijing 1 Court of Beijing Municipality 人民法院 Municipality Haidian District of Haidian District People’s 北京市海淀区人 京 0108 110108 Beijing 1 Court of Beijing Municipality 民法院 Municipality Mentougou Mentougou District People’s 北京市门头沟区 京 0109 110109 District of Beijing 1 Court of Beijing Municipality 人民法院 Municipality Changping Changping District People’s 北京市昌平区人 京 0114 110114 District of Beijing 1 Court of Beijing Municipality 民法院 Municipality Yanqing County People’s 延庆县人民法院 京 0229 110229 Yanqing County 1 Court No. 2 Intermediate People's 北京市第二中级 京 02 2 Court of Beijing Municipality 人民法院 Dongcheng Dongcheng District People’s 北京市东城区人 京 0101 110101 District of Beijing 1 Court of Beijing Municipality 民法院 Municipality Xicheng District Xicheng District People’s 北京市西城区人 京 0102 110102 of Beijing 1 Court of Beijing Municipality 民法院 Municipality Fengtai District of Fengtai District People’s 北京市丰台区人 京 0106 110106 Beijing 1 Court of Beijing Municipality 民法院 Municipality 1 Fangshan District Fangshan District People’s 北京市房山区人 京 0111 110111 of Beijing 1 Court of Beijing Municipality 民法院 Municipality Daxing District of Daxing District People’s 北京市大兴区人 京 0115 -

Download File
On the Periphery of a Great “Empire”: Secondary Formation of States and Their Material Basis in the Shandong Peninsula during the Late Bronze Age, ca. 1000-500 B.C.E Minna Wu Submitted in partial fulfillment of the requirements for the degree of Doctor of Philosophy in the Graduate School of Arts and Sciences COLUMIBIA UNIVERSITY 2013 @2013 Minna Wu All rights reserved ABSTRACT On the Periphery of a Great “Empire”: Secondary Formation of States and Their Material Basis in the Shandong Peninsula during the Late Bronze-Age, ca. 1000-500 B.C.E. Minna Wu The Shandong region has been of considerable interest to the study of ancient China due to its location in the eastern periphery of the central culture. For the Western Zhou state, Shandong was the “Far East” and it was a vast region of diverse landscape and complex cultural traditions during the Late Bronze-Age (1000-500 BCE). In this research, the developmental trajectories of three different types of secondary states are examined. The first type is the regional states established by the Zhou court; the second type is the indigenous Non-Zhou states with Dong Yi origins; the third type is the states that may have been formerly Shang polities and accepted Zhou rule after the Zhou conquest of Shang. On the one hand, this dissertation examines the dynamic social and cultural process in the eastern periphery in relation to the expansion and colonization of the Western Zhou state; on the other hand, it emphasizes the agency of the periphery during the formation of secondary states by examining how the polities in the periphery responded to the advances of the Western Zhou state and how local traditions impacted the composition of the local material assemblage which lay the foundation for the future prosperity of the regional culture. -

View Our Factory List
List updated 16th June 2021 FACTORY LIST Country Road Group is committed to driving positive social and environmental change in our supply chain. We mandate safe, inclusive and respectful workplaces wherever our products are manufactured, and are committed to greater transparency of our manufacturing operations. In line with this commitment, Country Road Group has publicly disclosed this list of factories involved in the manufacture of Country Road Group-branded products. This list includes the names, addresses, product categories and worker statistics of sites engaged in the manufacture of our goods. All sites listed are included in our Approved Factory Program and our team works closely with all suppliers and factories to continuously implement improvements. By releasing this information, we aim to provide customers with greater insights into our supply chain. All sites listed are correct at the time of publishing, and due to the seasonal nature of the retail industry this list is subject to change. * Data Not Captured: we are working to close this data gap through updated audit reports and working back with our supply partners. % OF % OF TOTAL SITE NAME SITE ADDRESS PROVINCE COUNTRY PRODUCT CATEGORY FEMALE INTERNATIONAL WORKERS WORKERS MIGRANT WORKERS ABHI HOME PLOT NO. 45, SECTOR- 29, PART – 1, HUDA, PANIPAT HARYANA INDIA HOME 129 8% * ABRAHAM MOON AND SONS LTD NETHERFIELD MILLS, GUISELEY, LEEDS WEST YORKSHIRE UNITED KINGDOM FOOTWEAR & ACCESSORIES, HOME 232 34% * ACME INDUSTRIES CO., LTD 99 MOO 4, BANGNA-TRAD KM. 35 BANGPLEE-NOI, BANGBOR SAMUT PRAKAN THAILAND HOME 436 55% 33% ANHUI TENGYANG CLOTHING CO., LTD. BUILDING 3#, YILITENG INDUSTRIAL PARK, QINGHE ROAD LUYANG INDUSTRIAL PARK, LUYANG DISTRICT, HEFEI ANHUI CHINA APPAREL 246 60% * ANM INTERNATIONAL PLOT NO.-62, SECTOR-6 IMT MANESAR, GURGAON HARYANA INDIA FOOTWEAR & ACCESSORIES 88 8% 0% ANTSIRABE KNITWEAR SA PROPRIETE VOION TN 1458 AMBOHIMENA, ANTSIRABE VAKINANKARATRA MADAGASCAR APPAREL 1653 43% * ART WAY CO., LTD. -

The Mineral Industry of China in 2007
2007 Minerals Yearbook CHINA U.S. Department of the Interior December 2009 U.S. Geological Survey THE MINERAL INDUS T RY OF CHINA By Pui-Kwan Tse After three decades of economic development, China probably have some impact on the global commodity prices has become one of the leading economic and trade powers (Batson and King, 2008). in the world, one of the top destinations for foreign direct investment, and an export destination of choice. During the Minerals in the National Economy past several years, the Government’s economic policy was to prevent economic slowdown and fight inflation. In 2007, China is rich in mineral resources and was the world’s China’s economic growth rate was 11.9% and represented the leading producer of aluminum, antimony, barite, bismuth, coal, fifth consecutive year of double-digit expansion. Industrial fluorspar, gold, graphite, iron and steel, lead, phosphate rock, production increased by 18.5% compared with that of 2006. rare earths, talc, tin, tungsten, and zinc in 2007. It ranked among The consumer price index (a measurement of inflation) rose to the top three countries in the world in the production of many a decade high of 4.8%. To prevent economic “overheating,” the other mineral commodities. China was the leading exporter Government raised interest rates and the People’s Bank of China of antimony, barite, coal, fluorspar, graphite, rare earths, and (the central bank) required commercial banks to increase the tungsten in the world. The country’s demand for chromium, reserve-requirement ratio 11 times to 11.5% at yearend 2007. -

Everbright Greentech Secures Wendeng Biomass Electricity and Heat Cogeneration Project and Linshu Hazardous Waste Landfill Project
Press Release EVERBRIGHT GREENTECH SECURES WENDENG BIOMASS ELECTRICITY AND HEAT COGENERATION PROJECT AND LINSHU HAZARDOUS WASTE LANDFILL PROJECT Hong Kong, 26 June, 2017 - China Everbright Greentech Limited (“Everbright Greentech” or the “Company”) (HKSE: 01257) is pleased to announce that it has secured Wendeng Biomass Electricity and Heat Cogeneration Project (“Wendeng Project”) and Linshu Hazardous Waste Landfill Project (“Linshu Landfill Project”) in Shandong Province, the total investment of which will amount to approximately RMB479 million. According to the investment agreement signed by the Company and the People’s Government of Wendeng District in Weihai City of Shandong Province, Wendeng Project will be invested in and constructed on a BOO (Build-Operate-Own) model, and will command a total investment of approximately RMB330 million. The project is designed to have an annual biomass processing capacity of 300,000 tonnes, and is expected to generate around 180,000,000 kWh of green electricity annually. Meanwhile, the Company signed an investment agreement with the People’s Government of Linshu County in Shandong Province to invest in and construct Linshu Landfill Project in two phases. The project has a total designed storage capacity of 700,000 m3. Phase I of the project, with a total investment of approximately RMB149 million, will have a designed storage capacity of 300,000 m3 and a designed annual hazardous waste treatment capacity of 20,000 tonnes. Mr. Qian Xiaodong, CEO of Everbright Greentech, said, “Everbright Greentech has secured several new projects recently, which demonstrates our strong business development and efficient execution capabilities. Wendeng Project is the Company’s first biomass project in Shandong Province. -

Royal Holloway University of London
ROYAL HOLLOWAY UNIVERSITY OF LONDON DOCTORAL THESIS Numerical modelling of the craton destruction process, with a type-example from the North China Craton Author: Supervisors: Liang Liu Prof. Jason P. Morgan Prof. Martin A. Menzies Prof. Yigang Xu A thesis submitted in fulfilment of the requirements for the degree of Doctor of Philosophy April 10, 2018 Department of Earth Sciences Royal Holloway University of London Egham, United Kingdom iii Declaration of Authorship I, Liang Liu hereby declare that this thesis and the work presented in it is entirely my own. Where I have consulted the work of others, this is always clearly stated. Signed: Date: 2018/04/10 v Learning without thought is labor lost; thought without learning is perilous. ------ Confucius vii Abstract: The phenomenon of cratonic destruction has attracted attentions among numerical modelers. However, existing modelling work appears to lack enough constraints from geological and geophysical observations. To better combine the observations with the modelling approach, and to further understand the destruction of the North China Craton (NCC), I firstly reviewed current knowledge about the evolution of the North China Craton, and then outlined the strength and weakness associated with classic delamination and convective erosion models. By integrating new observational data and 2-D numerical modeling results, I put forward a two-stage model to account for the destruction of the NCC, that is, cratonic keel delamination followed by localized convective erosion and lithospheric extension. As revealed in the evolution of the NCC, its destruction appears to be accompanied by the inversion of a pre-existing North China Cratonic Basin (NCCB), which is partly preserved in southeastern Ordos. -
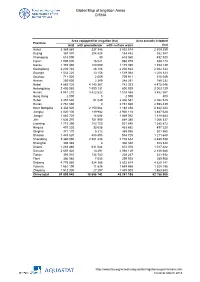
Global Map of Irrigation Areas CHINA
Global Map of Irrigation Areas CHINA Area equipped for irrigation (ha) Area actually irrigated Province total with groundwater with surface water (ha) Anhui 3 369 860 337 346 3 032 514 2 309 259 Beijing 367 870 204 428 163 442 352 387 Chongqing 618 090 30 618 060 432 520 Fujian 1 005 000 16 021 988 979 938 174 Gansu 1 355 480 180 090 1 175 390 1 153 139 Guangdong 2 230 740 28 106 2 202 634 2 042 344 Guangxi 1 532 220 13 156 1 519 064 1 208 323 Guizhou 711 920 2 009 709 911 515 049 Hainan 250 600 2 349 248 251 189 232 Hebei 4 885 720 4 143 367 742 353 4 475 046 Heilongjiang 2 400 060 1 599 131 800 929 2 003 129 Henan 4 941 210 3 422 622 1 518 588 3 862 567 Hong Kong 2 000 0 2 000 800 Hubei 2 457 630 51 049 2 406 581 2 082 525 Hunan 2 761 660 0 2 761 660 2 598 439 Inner Mongolia 3 332 520 2 150 064 1 182 456 2 842 223 Jiangsu 4 020 100 119 982 3 900 118 3 487 628 Jiangxi 1 883 720 14 688 1 869 032 1 818 684 Jilin 1 636 370 751 990 884 380 1 066 337 Liaoning 1 715 390 783 750 931 640 1 385 872 Ningxia 497 220 33 538 463 682 497 220 Qinghai 371 170 5 212 365 958 301 560 Shaanxi 1 443 620 488 895 954 725 1 211 648 Shandong 5 360 090 2 581 448 2 778 642 4 485 538 Shanghai 308 340 0 308 340 308 340 Shanxi 1 283 460 611 084 672 376 1 017 422 Sichuan 2 607 420 13 291 2 594 129 2 140 680 Tianjin 393 010 134 743 258 267 321 932 Tibet 306 980 7 055 299 925 289 908 Xinjiang 4 776 980 924 366 3 852 614 4 629 141 Yunnan 1 561 190 11 635 1 549 555 1 328 186 Zhejiang 1 512 300 27 297 1 485 003 1 463 653 China total 61 899 940 18 658 742 43 241 198 52