Catalog No. Contents ADP (Adenosine-5'-Diphosphate) Aggrecetin® 1.0-1.5Mg/Ml (Includes 2.0Ml Diluent) Aggrecetin® 100Mg
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Laboratory Testing for Von Willebrand Disease
75 Laboratory Testing for von Willebrand Disease: The Past, Present, and Future State of Play for von Willebrand Factor Assays that Measure Platelet Binding Activity, with or without Ristocetin Sarah Just, B App Sc. MLS, MAIMS1 1 Department of Haematology, South Eastern Area Laboratory Service Address for correspondence SarahJust,BAppSc.MLS,MAIMS, (SEALS), Prince of Wales Hospital, Sydney, New South Wales, Department of Haematology, South Eastern Area Laboratory Service Australia (SEALS), Prince of Wales Hospital, Sydney, NSW 2031, Australia (e-mail: [email protected]). Semin Thromb Hemost 2017;43:75–91. Abstract von Willebrand disease (VWD) was first described nearly a century ago in 1924 by Erik Adolf von Willebrand. Diagnostic testing at the time was very limited and it was not until the mid to late 1900s that more tests became available to assist with the diagnosis and Keywords classification of VWD. Two of these tests are based on ristocetin, one being ristocetin- ► ristocetin cofactor induced platelet aggregation (RIPA) and the other the von Willebrand factor (VWF) ► ristocetin induced ristocetin cofactor assay (VWF:RCo). The VWF:RCo assay provides functional assessment platelet aggregation of in vitro VWF binding to the platelet glycoprotein (Gp) complex, GPIb-IX-V. Despite ► von Willebrand some advancements and newer technologies utilizing the principles of the original disease VWF:RCo assay, the original assay is still referred to as the gold standard for measure- ► laboratory testing ment of VWF activity. This article will review the history of VWD diagnostic assays, ► von Willebrand factor including RIPA and VWF:RCo over the past 40 years, as well as the newer assays that ► von Willebrand factor measure platelet binding with or without ristocetin, and which have been developed activity with the aim to potentially replace platelet-based ristocetin-dependent assays. -

Diagnosis of Hemophilia and Other Bleeding Disorders
Diagnosis of Hemophilia and Other Bleeding Disorders A LABORATORY MANUAL Second Edition Steve Kitchen Angus McCraw Marión Echenagucia Published by the World Federation of Hemophilia (WFH) © World Federation of Hemophilia, 2010 The WFH encourages redistribution of its publications for educational purposes by not-for-profit hemophilia organizations. For permission to reproduce or translate this document, please contact the Communications Department at the address below. This publication is accessible from the World Federation of Hemophilia’s website at www.wfh.org. Additional copies are also available from the WFH at: World Federation of Hemophilia 1425 René Lévesque Boulevard West, Suite 1010 Montréal, Québec H3G 1T7 CANADA Tel.: (514) 875-7944 Fax: (514) 875-8916 E-mail: [email protected] Internet: www.wfh.org Diagnosis of Hemophilia and Other Bleeding Disorders A LABORATORY MANUAL Second Edition (2010) Steve Kitchen Angus McCraw Marión Echenagucia WFH Laboratory WFH Laboratory (co-author, Automation) Training Specialist Training Specialist Banco Municipal Sheffield Haemophilia Katharine Dormandy de Sangre del D.C. and Thrombosis Centre Haemophilia Centre Universidad Central Royal Hallamshire and Thrombosis Unit de Venezuela Hospital The Royal Free Hospital Caracas, Venezuela Sheffield, U.K. London, U.K. on behalf of The WFH Laboratory Sciences Committee Chair (2010): Steve Kitchen, Sheffield, U.K. Deputy Chair: Sukesh Nair, Vellore, India This edition was reviewed by the following, who at the time of writing were members of the World Federation of Hemophilia Laboratory Sciences Committee: Mansoor Ahmed Clarence Lam Norma de Bosch Sukesh Nair Ampaiwan Chuansumrit Alison Street Marión Echenagucia Alok Srivastava Andreas Hillarp Some sections were also reviewed by members of the World Federation of Hemophilia von Willebrand Disease and Rare Bleeding Disorders Committee. -

Platelet Function Disorders
TREATMENT OF HEMOPHILIA APRIL 2008 • NO 19 PLATELET FUNCTION DISORDERS Second Edition Anjali A. Sharathkumar Amy Shapiro Indiana Hemophilia and Thrombosis Center Indianapolis, U.S.A. Published by the World Federation of Hemophilia (WFH), 1999; revised 2008. © World Federation of Hemophilia, 2008 The WFH encourages redistribution of its publications for educational purposes by not-for-profit hemophilia organizations. In order to obtain permission to reprint, redistribute, or translate this publication, please contact the Communications Department at the address below. This publication is accessible from the World Federation of Hemophilia’s website at www.wfh.org. Additional copies are also available from the WFH at: World Federation of Hemophilia 1425 René Lévesque Boulevard West, Suite 1010 Montréal, Québec H3G 1T7 CANADA Tel. : (514) 875-7944 Fax : (514) 875-8916 E-mail: [email protected] Internet: www.wfh.org The Treatment of Hemophilia series is intended to provide general information on the treatment and management of hemophilia. The World Federation of Hemophilia does not engage in the practice of medicine and under no circumstances recommends particular treatment for specific individuals. Dose schedules and other treatment regimes are continually revised and new side effects recognized. WFH makes no representation, express or implied, that drug doses or other treatment recommendations in this publication are correct. For these reasons it is strongly recommended that individuals seek the advice of a medical adviser and/or consult printed instructions provided by the pharmaceutical company before administering any of the drugs referred to in this monograph. Statements and opinions expressed here do not necessarily represent the opinions, policies, or recommendations of the World Federation of Hemophilia, its Executive Committee, or its staff. -

Diagnostic: Von Willebrand Disease Screening Assay
Diagnostic: von Willebrand Disease Screening Assay In Brief Improved and simplified diagnostic assay for von Willebrand Disease (VWD) screening. No need for ristocetin, aggregometer, or platelet reagents, reducing assay costs and false positives, while improving reproducibility. Description von Willebrand Disease (VWD) is the most commonly diagnosed bleeding disorder, affecting up to 1% of the general population. This improved assay for detection of VWD uses a flexible ELISA format and is amenable to FACS analysis or bead‐based assays for higher throughput. The assay, called VWF:IbCo, employs mutants of the platelet protein GPIb without the need for ristocetin as an agonist for binding functionally relevant von Willebrand factor (VWF). This improved method offers several advantages over the most commonly used ristocetin cofactor assay, VWF:RCo, including reduced costs, reduced false positive rates, and simplified laboratory interpretations. The VWF:RCo assay relies on the interaction of the antibiotic ristocetin with VWF resulting in the agglutination of platelets. It also uses a turbidometric or aggregometer readout and has been difficult to standardize. A study comparing results of the VWF:RCo method and this improved VWF:IbCo assay showed better reproducibility and lower false positive rates with VWF:IbCo, especially in individuals with VWF polymorphisms that affect the binding of ristocetin to VWF but are not associated with loss of VWF function. Benefits Standard instrument platform (no specialized aggregometer needed) Platelets/ristocetin -

The Aptamer BT200 Blocks Von Willebrand Factor and Platelet Function in Blood of Stroke Patients Katarina D
www.nature.com/scientificreports OPEN The aptamer BT200 blocks von Willebrand factor and platelet function in blood of stroke patients Katarina D. Kovacevic1*, Stefan Greisenegger2, Agnes Langer2, Georg Gelbenegger1, Nina Buchtele3, Ingrid Pabinger4, Karin Petroczi1, Shuhao Zhu5, James C. Gilbert5 & Bernd Jilma1 The efect of conventional anti-platelet agents is limited in secondary stroke prevention, and their efects are blunted under high shear stress in the presence of increased levels of circulating von Willebrand factor (VWF). VWF is critically involved in thrombus formation at sites of stenotic extracranial/intracranial arteries. A third generation anti-VWF aptamer (BT200) has been generated which could be useful for secondary stroke prevention. To characterize the efects of BT200 in blood of patients with large artery atherosclerosis stroke (LAA). Blood samples were obtained from 33 patients with acute stroke or transient ischemic attack to measure inhibition of VWF activity and VWF-dependent platelet function. Patients who received clopidogrel or dual antiplatelet therapy did not difer in VWF dependent platelet function tests from aspirin treated patients. Of 18 patients receiving clopidogrel with or without aspirin, only 3 had a prolonged collagen adenosine diphosphate closure time, and none of the patients had ristocetin induced aggregation in the target range. BT200 concentration-dependently reduced median VWF activity from 178 to < 3%, ristocetin induced platelet aggregation from 40U to < 10U and prolonged collagen adenosine diphosphate closure times from 93 s to > 300 s. Baseline VWF activity correlated (r = 0.86, p < 0.001) with concentrations needed to reduce VWF activity to < 20% of normal, indicating that BT200 acts in a target concentration- dependent manner. -

Multiplate® Analyzer Powerful Analysis of Platelet Function Multiplate® Analyzer Addressing Unmet Medical Needs
Multiplate® analyzer Powerful analysis of platelet function Multiplate® analyzer Addressing unmet medical needs Milestone in analysis, major asset to therapy A potent force for platelet inhibition Roche’s stated aim is to combine true innovation Its best-in-class predictivity for thrombotic and with proven medical and diagnostic expertise. bleeding risk is a potent force in anti-platelet therapy. Multiplate® marks a milestone success in this It enables doctors to tailor treatment to the patient’s ambitious endeavor. need and stratify patients who are at risk of bleeding. The Multiplate® system addresses a significant Underpinned by highly standardized testing technology, unmet medical need by improving assessments Multiplate® is making powerful medical momentum in of patients’ platelet function. It provides invaluable this important field of patient care. Here today, it is the support for clinical decision-making in cardiology, analyzer destined to set tomorrow’s standards. surgery and intensive care. And that makes this analyzer a key asset for cardiologists, anesthetists and hematologists. Predictive power Best predictivity – Best predictivity – for tailored anti-platelet therapy for stratification of bleeding risk • Approx. one in five patients responds • Patients on dual anti-platelet therapy inadequately to clopidogrel with impaired platelet function are at • Risk of ischemic complications five greater risk of intra- and postopera- to ten times greater in patients tive bleeding and transfusions who respond poorly to clopidogrel. • Patients stratified as high-responders • Other more potent drugs act more to clopidogrel are at 2.6-times higher consistently but increase bleeding risk of major bleeding and cost up to 15 times as much as • Multiplate® helps improve hemostatic generic clopidogrel management in the bleeding patient • Success with tailored, Multiplate®- after surgery, thereby contributing to assisted APT reported by several a better outcome and lower costs. -

Von Willebrand Disease Genetic Subtyping, Type 2 and Platelet Type
Von Willebrand Disease Genetic Subtyping, Type 2 and Platelet Type Von Willebrand disease (VWD) is the most common inherited bleeding disorder and is classied into three major types, type 1, type 2, and type 3. 1 After diagnosis, subtyping may be indicated. Analysis of von Willebrand factor (VWF) multimers using a qualitative assay Tests to Consider may help determine the type, but additional molecular genetic testing may be required to distinguish among certain types and subtypes. These genetic tests may be used to evaluate von Willebrand Disease, Type 2A (VWF) family members of individuals with known variants or conrm a phenotypic diagnosis of Sequencing Exon 28 with Reex to 9 Exons (Temporary Referral as of 02/10/21) VWD types 2A, 2B, 2M, 2N, or platelet type, helping to distinguish type 2N from mild 2005480 hemophilia A, and type 2B from platelet type VWD [PT-VWD]. An accurate phenotypic Method: Polymerase Chain Reaction/Sequencing diagnosis helps guide therapeutic decision-making. Molecular test to conrm a phenotypic diagnosis of VWD type 2A Disease Overview von Willebrand Disease, Type 2B (VWF) Sequencing (Temporary Referral as of 02/10/21) 2005486 Incidence Method: Polymerase Chain Reaction/Sequencing VWD type 2: 1-5/10,000 2 Molecular test to distinguish VWD type 2B from Platelet-type VWD: <1/1,000,000 3 PT-VWD von Willebrand Disease, Type 2M (VWF) Symptoms Sequencing (Temporary Referral as of 02/10/21) 2005490 Patients with VWD may demonstrate the following 4: Method: Polymerase Chain Reaction/Sequencing Mucocutaneous bleeding after brushing or ossing teeth Molecular test to conrm a phenotypic diagnosis Unexplained bruising of VWD type 2M Prolonged repeated nosebleeds von Willebrand Disease, Type 2N (VWF) Menorrhagia Sequencing (Temporary Referral as of Prolonged bleeding following childbirth, trauma, or surgery 02/10/21) 2005494 Method: Polymerase Chain Reaction/Sequencing For clinical characteristics of subtypes, see table. -
WO 2014/025685 A2 13 February 2014 (13.02.2014) P O P C T
(12) INTERNATIONAL APPLICATION PUBLISHED UNDER THE PATENT COOPERATION TREATY (PCT) (19) World Intellectual Property Organization International Bureau (10) International Publication Number (43) International Publication Date WO 2014/025685 A2 13 February 2014 (13.02.2014) P O P C T (51) International Patent Classification: (81) Designated States (unless otherwise indicated, for every C12Q 1/56 (2006.01) kind of national protection available): AE, AG, AL, AM, AO, AT, AU, AZ, BA, BB, BG, BH, BN, BR, BW, BY, (21) International Application Number: BZ, CA, CH, CL, CN, CO, CR, CU, CZ, DE, DK, DM, PCT/US2013/053612 DO, DZ, EC, EE, EG, ES, FI, GB, GD, GE, GH, GM, GT, (22) International Filing Date: HN, HR, HU, ID, IL, IN, IS, JP, KE, KG, KN, KP, KR, 5 August 2013 (05.08.2013) KZ, LA, LC, LK, LR, LS, LT, LU, LY, MA, MD, ME, MG, MK, MN, MW, MX, MY, MZ, NA, NG, NI, NO, NZ, (25) Filing Language: English OM, PA, PE, PG, PH, PL, PT, QA, RO, RS, RU, RW, SA, (26) Publication Language: English SC, SD, SE, SG, SK, SL, SM, ST, SV, SY, TH, TJ, TM, TN, TR, TT, TZ, UA, UG, US, UZ, VC, VN, ZA, ZM, (30) Priority Data: zw. 61/680,1 11 6 August 2012 (06.08.2012) US 61/681,485 9 August 2012 (09.08.2012) US (84) Designated States (unless otherwise indicated, for every PCT/S2200 1/0/0494 5 July 2013 (05.07.2013) US kind of regional protection available): ARIPO (BW, GH, GM, KE, LR, LS, MW, MZ, NA, RW, SD, SL, SZ, TZ, (71) Applicant: JNC CORPORATION [JP/JP]; 2-1, Otemachi UG, ZM, ZW), Eurasian (AM, AZ, BY, KG, KZ, RU, TJ, 2-Chome, Chiyoda-ku, Chiyoda-ku, Tokyo, 100-8105 (JP). -

Diagnosis of Platelet-Type Von Willebrand Disease by Flow Cytometry
Brief Report Diagnosis of platelet-type von Willebrand disease by flow cytometry Silvia Giannini, Luca Cecchetti, Anna Maria Mezzasoma, and Paolo Gresele Division of Internal and Cardiovascular Medicine, Department of Internal Medicine, University of Perugia, Perugia, Italy ABSTRACT Platelet-type von Willebrand disease (PT-VWD) is a rare the GPIb α gene leading to a methionine to valine substitu - autosomal dominant bleeding disorder which is due to a tion (M239V). Flow cytometry represents a useful tool for mutation in the gene encoding for platelet glycoprotein Ib α the diagnosis of PT-VWD. (GPIb α) resulting in enhanced affinity for von Willebrand factor (VWF). PT-VWD is often mistakenly diagnosed as type Key words: von Willebrand disease, PT-VWD, GPIb α. 2B VWD for the similarities between these two conditions. We characterized a new case of PT-VWD and evaluated the Citation: Giannini S, Cecchetti L, Mezzasoma AM, and Gresele usefulness of a flow cytometric assay in the differential diag - P. Diagnosis of platelet-type von Willebrand disease by flow nosis between PT-VWD (n=1) and type 2B VWD (n=4). The cytometry. Haematologica 2010;95:1021-1024. flow cytometric assay was able to highlight the increased doi:10.3324/haematol.2009.015990 affinity of VWF for GPIb α as much as did RIPA and to differ - entiate the two diseases through mixing tests. Genetic analy - ©2010 Ferrata Storti Foundation. This is an open-access paper. sis revealed a heterozygous point mutation in codon 239 of Introduction cryoprecipitate challenge, which are rather cumbersome. The last method in particular often gives ambiguous results, Platelet-type von Willebrand disease (PT-VWD) is a rare because false positives can be found in some individuals with autosomal dominant bleeding disorder due to a mutation in type 2B VWD. -

Von Willebrand Disease Typical Lab Findings
VON WILLEBRAND DISEASE Type 1 Partial quantitative deficiency of vWF. Autosomal dominant disorder, but only a minority of persons with a nonfunctional vWF allele have bleeding symptoms. Type 2 Qualitative abnormalities of vWF. Type 2A Abnormal assembly of high-molecular-weight vWF multimers. Autosomal dominant. Type 2B An abnormal (increased) binding of vWF to platelets, causes depletion of high- molecular-weight vWF multimers and thrombocytopenia. Autosomal dominant. Type 2M Abnormal (decreased) binding of vWF to platelets, but with normal vWF multimer distribution. Autosomal dominant. Type 2N Abnormal (decreased) binding of vWF to factor VIII, causing low plasma factor VIII levels. Autosomal recessive. Type 3 Virtually complete deficiency of vWF. Autosomal recessive (but most carriers do not manifest the abnormalities of type 1 disease). Pseudo-von Willebrand disease (platelet-type vWD) Abnormal platelet GP Ib-IX-V with increased affinity for large vWF multimers. Phenotype indistinguishable from type 2B disease. TYPICAL LAB FINDINGS TYPICAL LABORATORY FINDINGS IN VWD VARIANTS Type vWF: Ag vWF: RCof F VIII RIPA Multimer pattern 1 All sizes present or uniformly 2A or NL Absence of large & intermediate forms 2B or NL ↑ Absence of large forms 2M or NL All sizes present 2N NL NL or NL All sizes present 3 N/A Absence of all vWF vWF = von Willebrand Factor FVIII = Factor VIII level Ag = antigen RCof = ristocetin cofactor activity RIPA = ristocetin-induced platelet agglutination. Concentration of ristocetin at which platelets aggregate. References: Federici AB and Mannucci PM. Ann Med 2007;39:346 - 58 and Kitchens. Consultative Hemostasis and Thrombosis. Second Edition; Saunders Publishing; 2007:103. -

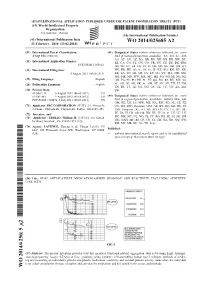
S41598-021-91165-8.Pdf
www.nature.com/scientificreports OPEN In vitro assessment and phase I randomized clinical trial of anfbatide a snake venom derived anti‑thrombotic agent targeting human platelet GPIbα Benjamin Xiaoyi Li1,2*, Xiangrong Dai1,2, Xiaohong Ruby Xu3,4,5, Reheman Adili3,4, Miguel Antonio Dias Neves3,4,5,6, Xi Lei3,4, Chuanbin Shen3,4,5, Guangheng Zhu3,4, Yiming Wang3,4,5,6, Hui Zhou3,4, Yan Hou3,4, Tifany Ni3,4,5, Yfe Pasman3,4,5,6, Zhongqiang Yang2, Fang Qian2, Yanan Zhao7, Yongxiang Gao8, Jing Liu8, Maikun Teng8, Alexandra H. Marshall3,4, Eric G. Cerenzia3,4,9, Mandy Lokyee Li1 & Heyu Ni3,4,5,6,9,10,11* The interaction of platelet GPIbα with von Willebrand factor (VWF) is essential to initiate platelet adhesion and thrombosis, particularly under high shear stress conditions. However, no drug targeting GPIbα has been developed for clinical practice. Here we characterized anfbatide, a GPIbα antagonist purifed from snake (Deinagkistrodon acutus) venom, and evaluated its interaction with GPIbα by surface plasmon resonance and in silico modeling. We demonstrated that anfbatide interferds with both VWF and thrombin binding, inhibited ristocetin/botrocetin‑ and low‑dose thrombin‑ induced human platelet aggregation, and decreased thrombus volume and stability in blood fowing over collagen. In a single‑center, randomized, and open‑label phase I clinical trial, anfbatide was administered intravenously to 94 healthy volunteers either as a single dose bolus, or a bolus followed by a constant rate infusion of anfbatide for 24 h. Anfbatide inhibited VWF‑mediated platelet aggregation without signifcantly altering bleeding time or coagulation. The inhibitory efects disappeared within 8 h after drug withdrawal. -

Studies on the Mechanism of Ristocetin-Induced Platelet Agglutination: EFFECTS of STRUCTURAL MODIFICATION of RISTOCETIN and VANCOMYCIN
Studies on the Mechanism of Ristocetin-Induced Platelet Agglutination: EFFECTS OF STRUCTURAL MODIFICATION OF RISTOCETIN AND VANCOMYCIN Barry S. Coller, Harvey R. Gralnick J Clin Invest. 1977;60(2):302-312. https://doi.org/10.1172/JCI108778. The mechanism by which ristocetin induces platelet agglutination in the presence of the von Willebrand factor was studied by chemically altering ristocetin and a similar antibiotic, vancomycin, by reaction with a water-soluble carbodiimide in the presence of glycine methyl ester at pH 4.75. Altering ristocetin's phenolic groups (which are thought to be important in its peptide-binding properties) resulted in a loss of both platelet-agglutinating and antibiotic activities. Restoring the phenolic groups with hydroxylamine restored both activities. Vancomycin has antibiotic and peptide-binding properties similar to ristocetin's, but differs structurally in having a free carboxyl group and thus a less positive charge at neutral pH. It does not induce platelet agglutination and actually inhibits ristocetin-induced agglutination. Reacting vancomycin with the water-soluble carbodiimide resulted in alteration of phenolic groups and permanent conversion of the carboxyl to a neutral derivative. Restoring the phenolic groups with hydroxylamine (but leaving the carboxyl neutralized) produced a compound with charge properties similar to ristocetin's which induced platelet agglutination as ristocetin does. These data suggest both a binding requirement (mediated through phenolic groups) and a strong positive charge requirement for ristocetin-induced agglutination. The data are consistent with a model wherein positively charged ristocetin binds, via its phenolic groups, to sites on the platelet surface and reduces the platelet's negative charge.