Heparin Sensitivity and Resistance: Management During Cardiopulmonary Bypass
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Identification of an Alpha-1 Antitrypsin Variant with Enhanced Specificity For
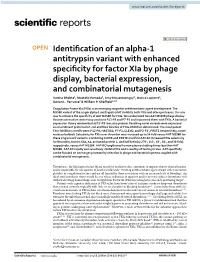
www.nature.com/scientificreports OPEN Identifcation of an alpha‑1 antitrypsin variant with enhanced specifcity for factor XIa by phage display, bacterial expression, and combinatorial mutagenesis Varsha Bhakta1, Mostafa Hamada2, Amy Nouanesengsy2, Jessica Lapierre2, Darian L. Perruzza2 & William P. Shefeld1,2* Coagulation Factor XIa (FXIa) is an emerging target for antithrombotic agent development. The M358R variant of the serpin alpha‑1 antitrypsin (AAT) inhibits both FXIa and other proteases. Our aim was to enhance the specifcity of AAT M358R for FXIa. We randomized two AAT M358R phage display libraries at reactive centre loop positions P13‑P8 and P7‑P3 and biopanned them with FXIa. A bacterial expression library randomized at P2′‑P3′ was also probed. Resulting novel variants were expressed as recombinant proteins in E. coli and their kinetics of FXIa inhibition determined. The most potent FXIa‑inhibitory motifs were: P13‑P8, HASTGQ; P7‑P3, CLEVE; and P2‑P3′, PRSTE (respectively, novel residues bolded). Selectivity for FXIa over thrombin was increased up to 34‑fold versus AAT M358R for these single motif variants. Combining CLEVE and PRSTE motifs in AAT‑RC increased FXIa selectivity for thrombin, factors XIIa, Xa, activated protein C, and kallikrein by 279‑, 143‑, 63‑, 58‑, and 36‑fold, respectively, versus AAT M358R. AAT‑RC lengthened human plasma clotting times less than AAT M358R. AAT‑RC rapidly and selectively inhibits FXIa and is worthy of testing in vivo. AAT specifcity can be focused on one target protease by selection in phage and bacterial systems coupled with combinatorial mutagenesis. Trombosis, the blockage of intact blood vessels by occlusive clots, continues to impose a heavy clinical burden, and is responsible for one quarter of deaths world-wide1. -

Normal Fibronectin Levels As a Function of Age in the Pediatric Population
Pediatr. Res. 17: 482-485 (1983) Normal Fibronectin Levels as a Function of Age in the Pediatric Population MICHAEL H. MCCAFFERTY,'~"MARTHA LEPOW, THOMAS M. SABA,'21' ESHIN CHO, HILAIRE MEUWISSEN, JOHN WHITE, AND SHARON F. ZUCKERBROD Departments of Physiology and Pediatrics, Albany Medical College of Union University, Albany, New York, USA Summary pediatric population with age has not been reported. This may be important in terms of appropriate interpretation of prevailing Fibronectin is an important non-immune opsonic protein influ- levels in children with various disease states, because normal encing phagocytic clearance of blood-borne nonbacterial particu- concentrations in children may be different from normal levels in lates which may arise in association with septic shock, tissue adults. This study was designed to measure fibronectin levels in a injury, and intravascular coagulation. In the present study, serum large group (n = 114) of normal children in order to define its fibronectin was measured by both electroimmunoassay as well as normal concentration as a function of age. rapid immunoturbidimetric assay in healthy children (n = 114) ranging in age from 1 month to 15 years in order to delineate the temporal alterations in fibronectin with age. Normal adult serum MATERIALS AND METHODS fibronectin concentrations are typically 220 pg/ml + 20 pg/ml. Serum concentration is 3540% lower than normal plasma con- Healthy children (n = 114) ranging in age from 1 month to 15 centration due to the binding of fibronectin to fibrin during clot years were seen as outpatients or as inpatients for minor surgical formation. Children between 1-12 months of age had significantly procedures. -

Mary Bartlett Bunge 40
EDITORIAL ADVISORY COMMITTEE Marina Bentivoglio Larry F. Cahill Stanley Finger Duane E. Haines Louise H. Marshall Thomas A. Woolsey Larry R. Squire (Chairperson) The History of Neuroscience in Autobiography VOLUME 4 Edited by Larry R. Squire ELSEVIER ACADEMIC PRESS Amsterdam Boston Heidelberg London New York Oxford Paris San Diego San Francisco Singapore Sydney Tokyo This book is printed on acid-free paper. (~ Copyright 9 byThe Society for Neuroscience All Rights Reserved. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopy, recording, or any information storage and retrieval system, without permission in writing from the publisher. Permissions may be sought directly from Elsevier's Science & Technology Rights Department in Oxford, UK: phone: (+44) 1865 843830, fax: (+44) 1865 853333, e-mail: [email protected]. You may also complete your request on-line via the Elsevier homepage (http://elsevier.com), by selecting "Customer Support" and then "Obtaining Permissions." Academic Press An imprint of Elsevier 525 B Street, Suite 1900, San Diego, California 92101-4495, USA http ://www.academicpress.com Academic Press 84 Theobald's Road, London WC 1X 8RR, UK http://www.academicpress.com Library of Congress Catalog Card Number: 2003 111249 International Standard Book Number: 0-12-660246-8 PRINTED IN THE UNITED STATES OF AMERICA 04 05 06 07 08 9 8 7 6 5 4 3 2 1 Contents Per Andersen 2 Mary Bartlett Bunge 40 Jan Bures 74 Jean Pierre G. Changeux 116 William Maxwell (Max) Cowan 144 John E. Dowling 210 Oleh Hornykiewicz 240 Andrew F. -

The Two Faces of Thrombosis: Coagulation Cascade and Platelet Aggregation. Are Platelets the Main Therapeutic Target
Thrombosis and Circulation Open Access Cimmino et al., J Thrombo Cir 2017, 3:1 Review Article Open Access The Two Faces of Thrombosis: Coagulation Cascade and Platelet Aggregation. Are Platelets the Main Therapeutic Target? Giovanni Cimmino*, Salvatore Fischetti and Paolo Golino Department of Cardio-Thoracic and Respiratory Sciences, Section of Cardiology, University of Campania “Luigi Vanvitelli”, Naples, Italy *Corresponding author: Giovanni Cimmino, MD, PhD, Department of Cardio-Thoracic and Respiratory Sciences, Section of Cardiology, University of Campania “Luigi Vanvitelli”, via Leonardo Bianchi, 180131 Naples, Italy. Tel: +39-081-7064175, Fax: +39-081-7064234; E-mail: [email protected] Received date: Dec 28, 2016, Accepted date: Jan 27, 2017, Published date: Jan 31, 2017 Copyright: © 2017 Giovanni C, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Abstract Acute thrombus formation is the pathophysiological substrate underlying several clinical conditions, such as acute coronary syndrome (ACS) and stroke. Activation of coagulation cascade is a key step of the thrombotic process: vessel injury results in exposure of the glycoprotein tissue factor (TF) to the flowing blood. Once exposed, TF binds factor VII/VIIa (FVII/FVIIa) and in presence of calcium ions, it forms a tertiary complex able to activate FX to FXa, FIX to FIXa, and FVIIa itself. The final step is thrombin formation at the site of vessel injury with subsequent platelet activation, fibrinogen to fibrin conversion and ultimately thrombus formation. Platelets are the key cells in primary hemostasis. -
Diagnostic Methods in Hematology II
DiagnosticDiagnostic methodsmethods inin hematologyhematology IIII Jan Zivny Department of Pathophysiology 1. LF UK OutlineOutline Specialized hematology tests • Evaluation of anemia – Anemia basics • Anemia caused by excessive erythrocyte loss • Anemia caused by deficient erythropoiesis • Diagnostic methods used in leukemia/lymphoma ANEMIAANEMIA • WHO criteria: Hb < 125 g/L in adults • US criteria: –M: Hb < 135 g/L –F: Hb < 125 g/L •• AnemiaAnemia isis clinicalclinical signsign CausesCauses ofof anemiaanemia • Insufficient RBC production – deficient erythropoiesis • Excessive RBC loss – Hemolysis (shortened lifespan of erythrocytes) – Acute bleeding (chronic bleeding leads to iron depletion and results in iron loss and deficient erythropoiesis) AnemiaAnemia causedcaused byby deficientdeficient erythropoiesiserythropoiesis Causes of insufficient erythropoiesis? AnemiaAnemia causedcaused byby deficientdeficient erythropoiesiserythropoiesis • Iron metabolism related (microcytic) – Iron deficiency – Chronic diseases • Vitamin B12 or folate deficiency (macrocytic) • Insuficient EPO production and marrow failure (normocytic) – kidney failure – aplastic anemia – myelodysplasia – leukemia DiagnosticDiagnostic aproachesaproaches toto ironiron metabolismmetabolism relatedrelated anemiaanemia IronIron deficiencydeficiency ChronicChronic diseasesdiseases IronIron deficiencydeficiency • microcytic anemia and/or anisocytosis • ↓ blood reticulocytes • hypoproliferative BM • Blood loss in excess of 10 to 20 mL of blood per day (> 5-10 mg of iron) or -
Tests for the Evaluation of Preterm Labor and Premature Rupture of Membranes
Medical Coverage Policy Effective Date ............................................. 7/15/2021 Next Review Date ....................................... 7/15/2022 Coverage Policy Number .................................. 0099 Tests for the Evaluation of Preterm Labor and Premature Rupture of Membranes Table of Contents Related Coverage Resources Overview .............................................................. 1 Recurrent Pregnancy Loss: Diagnosis and Treatment Coverage Policy ................................................... 1 Ultrasound in Pregnancy (including 3D, 4D and 5D General Background ............................................ 2 Ultrasound) Medicare Coverage Determinations .................. 13 Coding/Billing Information .................................. 13 References ........................................................ 15 INSTRUCTIONS FOR USE The following Coverage Policy applies to health benefit plans administered by Cigna Companies. Certain Cigna Companies and/or lines of business only provide utilization review services to clients and do not make coverage determinations. References to standard benefit plan language and coverage determinations do not apply to those clients. Coverage Policies are intended to provide guidance in interpreting certain standard benefit plans administered by Cigna Companies. Please note, the terms of a customer’s particular benefit plan document [Group Service Agreement, Evidence of Coverage, Certificate of Coverage, Summary Plan Description (SPD) or similar plan document] may differ -

Intrinsic Factor
ENZYMES INTRINSIC FACTOR EINECS Number 232-711-9 Alternative Names Vitamin B12-binding protein, Factor VII, Intrinsic Factor protein Assay Principle Intrinsic Factor binds specifically to Vitamin B12. The coating of a Vitamin B12-BSA (IF Content) conjugate to the ELISA plate allows for the extent of Intrinsic Factor binding to be investigated. A Mouse monoclonal Anti-Intrinsic Factor antibody is used to identify the concentration of Intrinsic Factor bound to the Vitamin B12. The Antibody bound to the Intrinsic Factor on the plate is identified by use of an Anti Mouse AP conjugate. PNPP substrate is used to develop signals, read at an absorbance of 405nm on a plate reader. What is pernicious anaemia? Key Benefits Intrinsic Factor is primarily used in the diagnosis of pernicious anaemia, a condition caused by a vitamin B12 deficiency. Prevalence in the general + SUPPLY SECURITY population varies from around 3% - 5%, and increases dramatically to Fully manufactured by BBI 5% - 20% among people older than 65 years. Solutions at our Crumlin site, ensuring control over manufacturing processes and supply chain + HIGH PURITY Intrinsic Factor has a purity of >95% ensuring optimal performance in your assay + PROVEN PERFORMANCE Porcine Intrinsic Factor works in a range of immunoassay formats The role of Intrinsic Factor in diagnosis + HIGH QUALITY Intrinsic Factor has a high affinity and specificity to vitamin B12, which Manufactured under a makes it ideal for use in immunoassays. Most commercial assays utilise Quality System compliant a competitive binding technique generating a chemiluminescent signal. with ISO 13485:2016 with Commercial assays can usually detect to a level of ~50 pg/ml vitamin B12. -

In Vitro Modelling of the Mucosa of the Oesophagus and Upper Digestive Tract
21 Review Article Page 1 of 21 In vitro modelling of the mucosa of the oesophagus and upper digestive tract Kyle Stanforth1, Peter Chater1, Iain Brownlee2, Matthew Wilcox1, Chris Ward1, Jeffrey Pearson1 1NUBI, Newcastle University, Newcastle upon Tyne, UK; 2Applied Sciences (Department), Northumbria University, Newcastle upon Tyne, UK Contributions: (I) Conception and design: All Authors; (II) Administrative support: All Authors; (III) Provision of study materials or patients: All Authors; (IV) Collection and assembly of data: All Authors; (V) Data analysis and interpretation: All Authors; (VI) Manuscript writing: All authors; (VII) Final approval of manuscript: All authors. Correspondence to: Kyle Stanforth. NUBI, Medical School, Framlington Place, Newcastle University, NE2 4HH, Newcastle upon Tyne, UK. Email: [email protected]. Abstract: This review discusses the utility and limitations of model gut systems in accurately modelling the mucosa of the digestive tract from both an anatomical and functional perspective, with a particular focus on the oesophagus and the upper digestive tract, and what this means for effective in vitro modelling of oesophageal pathology. Disorders of the oesophagus include heartburn, dysphagia, eosinophilic oesophagitis, achalasia, oesophageal spasm and gastroesophageal reflux disease. 3D in vitro models of the oesophagus, such as organotypic 3D culture and spheroid culture, have been shown to be effective tools for investigating oesophageal pathology. However, these models are not integrated with modelling of the upper digestive tract—presenting an opportunity for future development. Reflux of upper gastrointestinal contents is a major contributor to oesophageal pathologies like gastroesophageal reflux disease and Barratt’s oesophagus, and in vitro models are essential for understanding their mechanisms and developing solutions. -

Neoplastic Transformation Inactivates Specific Trans-Acting Factor(S
Proc. Nati. Acad. Sci. USA Vol. 85, pp. 1744-1748, March 1988 Biochemistry Neoplastic transformation inactivates specific trans-acting factor(s) required for the expression of the thyroglobulin gene (differentiation/DNA-protein interaction/thyroglobufln) V. ENRICO AVVEDIMENTO*tt, ANNAMARIA MUSTI*, ALFREDO Fusco*, MARCO J. BONAPACE*, AND ROBERTO Di LAURO§¶ *Centro di Endocrinologia ed Oncologia Sperimentale del Consiglio Nazionale delle Ricerce, Dipartimento di Biologia e Patologia Molecolare, II Facolta di Medicina e Chirurgia, Universita di Napoli, Naples, Italy; and fLaboratory of Biochemistry, National Cancer Institute, National Institutes of Health, Bethesda, MD 20892 Communicated by Maxine F. Singer, October 5, 1987 (receivedfor review February 18, 1987) ABSTRACT The expression of rat thyroglobulin gene is sible for the block of the thyroglobulin expression in trans- repressed following the transformation ofrat thyroid cells with formed thyroid cells. Kirsten murine sarcoma virus. The expression of a reporter We report here data on the expression of the reporter gene gene fused to the thyroglobulin promoter is down-regulated in for chloramphenicol acetyl transferase fused to the Tg pro- transformed thyroid cells in transient or in stable transfection moter, designated Tg P-CAT gene, in transformed cells assays. DNase and exonuclease HI cleavage-protection analysis either in transient or in stable transfection assays. We show: reveals that a promoter binding activity located at -60 base (i) that this marker is down-regulated in transformed thyroid pairs from the transcription start site is substantially reduced cells; (ii) that a specific Tg promoter binding activity is in transformed thyroid cells. The repression in the trans- substantially reduced upon transformation; and (iii) that the formed cells of the reporter gene joined to the thyroglobulin Tg P-CAT gene in transformed cells can be reactivated by promoter can be reversed by fusion with normal differentiated fusion with a normal differentiated thyroid cell. -

Hereditary Intrinsic Factor Deficiency in China Caused by a Novel Mutation
Ruan et al. BMC Medical Genetics (2020) 21:221 https://doi.org/10.1186/s12881-020-01158-z CASE REPORT Open Access Hereditary intrinsic factor deficiency in China caused by a novel mutation in the intrinsic factor gene—a case report Jing Ruan, Bing Han* , Junling Zhuang, Miao Chen, Fangfei Chen, Yuzhou Huang and Wenzhe Zhou Abstract Background: Hereditary intrinsic factor deficiency is a rare disease characterized by cobalamin deficiency with the lack of gastric intrinsic factor because of gastric intrinsic factor (GIF) mutations. Patients usually present with cobalamin deficiency without gastroscopy abnormality and intrinsic factor antibodies. Case presentation: A Chinese patient presented with recurrent severe anemia since age 2 with low cobalamin level and a mild elevation of indirect bilirubin. The hemoglobin level normalized each time after intramuscular vitamin B12 injection. Gene test verified a c.776delA frame shift mutation in exon 6 combined with c.585C > A nonsense early terminationmutationinexon5ofGIF which result in the dysfunction of gastric intrinsic factor protein. The hereditary intrinsic factor deficiency in literature was further reviewed and the ancestry of different mutation sites were discussed. Conclusions: A novel compound heterozygous mutation of GIF in a Chinese patient of hereditary intrinsic factor deficiency was reported. It was the first identified mutation of GIF in East-Asia and may indicate a new ancestry. Keywords: Megaloblastic anemia, Cobalamin deficiency, Intrinsic factor Background IFD is caused by homozygous or compound heterozy- Vitamin B12 or cobalamin deficiency is characterized by gous mutation in the gene of gastric intrinsic factor on megaloblastic anemia with neurological problems and chromosome 11q12. It presents in early childhood with can be caused by numerous acquired and inherited dis- the lack of gastric intrinsic factor, while the gastric acid eases [1]. -

Intradiscal Injection of an Autologous Alpha-2-Macroglobulin (A2M) Concentrate Alleviates Back Pain in FAC-Positive Patients
Orthopedics and Rheumatology Open Access Journal ISSN: 2471-6804 Research Article Ortho & Rheum Open Access Volume 4 Issue 2 - January 2017 Copyright © All rights are reserved by Pasquale X Montesano MD DOI: 10.19080/OROAJ.2017.04.555634 Intradiscal Injection of an Autologous Alpha-2- Macroglobulin (A2M) Concentrate Alleviates Back Pain in FAC-Positive Patients Pasquale X Montesano MD, *Jason M Cuellar MD, PhD, Gaetano J Scuderi MD 1Spine Surgeon, Montesano Spine and Sport, USA 2Spine surgeon, Department of Orthopaedic Surgery, Cedars-Sinai Medical Center, USA 3Spine surgeon, USA Submission: December 14, 2016; Published: January 03, 2017 *Corresponding author: Tel: ; Email: Jason M. Cuéllar MD, PhD, 450 N. Roxbury Drive, 3rd floor, Beverly Hills, CA 90210, Abstract Objectives: A cartilage degradation product, the Fibronectin-Aggrecan complex (FAC), has been identified in patients with degenerative disc disease (DDD). Alpha-2-macroglobulin (A2M) can prevent the formation of the G3 domain of aggrecan, reducing the fibronectin-aggrecan G3 complex and therefore may be an efficacious treatment. The present study was designed to determine a.b. The ability of autologousFAC to predict concentrated the response A2M to tothis relieve biologic back therapy. pain in patients with LBP from DDD and Study design/setting: Prospective cohort Patients: Main Outcome 24 patients Measurements: with low back pain and MRI-concordant DDD Oswestry disability index (ODI) and visual analog scores (VAS) were noted at baseline and at 3- and 6-month follow-up.Methods: Primary outcome of clinical improvement was defined as patients with both a decrease in VAS of at least 3 points and ODI >20 points. -

Heparin/Heparan Sulfate Proteoglycans Glycomic Interactome in Angiogenesis: Biological Implications and Therapeutical Use
Molecules 2015, 20, 6342-6388; doi:10.3390/molecules20046342 OPEN ACCESS molecules ISSN 1420-3049 www.mdpi.com/journal/molecules Review Heparin/Heparan Sulfate Proteoglycans Glycomic Interactome in Angiogenesis: Biological Implications and Therapeutical Use Paola Chiodelli, Antonella Bugatti, Chiara Urbinati and Marco Rusnati * Section of Experimental Oncology and Immunology, Department of Molecular and Translational Medicine, University of Brescia, Brescia 25123, Italy; E-Mails: [email protected] (P.C.); [email protected] (A.B.); [email protected] (C.U.) * Author to whom correspondence should be addressed; E-Mail: [email protected]; Tel.: +39-030-371-7315; Fax: +39-030-371-7747. Academic Editor: Els Van Damme Received: 26 February 2015 / Accepted: 1 April 2015 / Published: 10 April 2015 Abstract: Angiogenesis, the process of formation of new blood vessel from pre-existing ones, is involved in various intertwined pathological processes including virus infection, inflammation and oncogenesis, making it a promising target for the development of novel strategies for various interventions. To induce angiogenesis, angiogenic growth factors (AGFs) must interact with pro-angiogenic receptors to induce proliferation, protease production and migration of endothelial cells (ECs). The action of AGFs is counteracted by antiangiogenic modulators whose main mechanism of action is to bind (thus sequestering or masking) AGFs or their receptors. Many sugars, either free or associated to proteins, are involved in these interactions, thus exerting a tight regulation of the neovascularization process. Heparin and heparan sulfate proteoglycans undoubtedly play a pivotal role in this context since they bind to almost all the known AGFs, to several pro-angiogenic receptors and even to angiogenic inhibitors, originating an intricate network of interaction, the so called “angiogenesis glycomic interactome”.