Foreign Body Aspiration
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Chapter 32 FOREIGN BODIES of the HEAD, NECK, and SKULL BASE
Foreign Bodies of the Head, Neck, and Skull Base Chapter 32 FOREIGN BODIES OF THE HEAD, NECK, AND SKULL BASE RICHARD J. BARNETT, MD* INTRODUCTION PENETRATING NECK TRAUMA Anatomy Emergency Management Clinical Examination Investigations OPERATIVE VERSUS NONOPERATIVE MANAGEMENT Factors in the Deployed Setting Operative Management Postoperative Care PEDIATRIC INJURIES ORBITAL FOREIGN BODIES SUMMARY CASE PRESENTATIONS Case Study 32-1 Case Study 32-2 Case Study 32-3 Case Study 32-4 Case Study 32-5 Case Study 32-6 *Lieutenant Colonel, Medical Corps, US Air Force; Chief of Facial Plastic Surgery/Otolaryngology, Eglin Air Force Base Department of ENT, 307 Boatner Road, Suite 114, Eglin Air Force Base, Florida 32542-9998 423 Otolaryngology/Head and Neck Combat Casualty Care INTRODUCTION The mechanism and extent of war injuries are sig- other military conflicts. In a study done in Croatia with nificantly different from civilian trauma. Many of the 117 patients who sustained penetrating neck injuries, wounds encountered are unique and not experienced about a quarter of the wounds were from gunshots even at Role 1 trauma centers throughout the United while the rest were from shell or bomb shrapnel.1 The States. Deployed head and neck surgeons must be injury patterns resulting from these mechanisms can skilled at performing an array of evaluations and op- vary widely, and treating each injury requires thought- erations that in many cases they have not performed in ful planning to achieve a successful outcome. a prior setting. During a 6-month tour in Afghanistan, This chapter will address penetrating neck injuries all subspecialties of otolaryngology were encountered: in general, followed specifically by foreign body inju- head and neck (15%), facial plastic/reconstructive ries of the head, face, neck, and skull base. -

Pediatric Airway Foreign Body Retrieval: Surgical and Anesthetic Perspectives
Pediatric Anesthesia 2009 19 (Suppl. 1): 109–117 doi:10.1111/j.1460-9592.2009.03006.x Review article Pediatric airway foreign body retrieval: surgical and anesthetic perspectives KAREN B. ZUR MD* AND RONALD S. LITMAN DO† Departments of *Otolaryngology: Head & Neck Surgery and †Anesthesiology & Critical Care Medicine, University of Pennsylvania School of Medicine, The Children’s Hospital of Philadelphia, Philadelphia, PA, USA Summary Airway foreign body aspiration most commonly occurs in young children and is associated with a high rate of airway distress, morbidity, and mortality. The presenting symptoms of foreign body aspiration range from none to severe airway obstruction, and may often be innocuous and nonspecific. In the absence of a choking or aspiration event, the diagnosis may be delayed for weeks to months and contribute to worsening lung disease. Radiography and high resolution CT scan may contribute to the eventual diagnosis. Bron- choscopy is used to confirm the diagnosis and retrieve the object. The safest method of removing an airway foreign body is by utilizing general anesthesia. Communication between anesthesiologist and surgeon is essential for optimal outcome. The choice between maintenance of spontaneous and controlled ventilation is often based on personal preference and does not appear to affect the outcome of the procedure. Complications are related to the actual obstruction and to the retrieval of the impacted object. The localized inflammation and irritation that result from the impacted object can lead to bronchitis, -

Bruises- Wounds
Henry Shih OD, MD Medical Director Austin Emergency Center- Anderson Mill 13435 US Highway 183 North Suite 311 Austin, TX 78750 512-614-1200 BRUISES- http://austiner.com/ What are bruises? — Bruises happen when blood vessels under the skin break, but the skin isn’t cut. Blood leaks into the tissues under the skin. Bruises start off red in color, and then turn blue or purple. As they heal, bruises can turn green and yellow. Most bruises heal in 1 to 2 weeks, but some take longer. How are bruises treated? — A bruise will get better on its own. But to feel better and help your bruise heal, you can: o Put a cold gel pack, bag of ice, or bag of frozen vegetables on the injured area every 1 to 2 hours, for 15 minutes each time. Put a thin towel between the ice (or other cold object) and your skin. Use the ice (or other cold object) for at least 6 hours after your injury. Some people find it helpful to ice longer, even up to 2 days after their injury. o Raise the area, if possible – Raising the area above the level of your heart helps to reduce swelling. o Take medicine to reduce the pain and swelling – To treat pain, you can take Tylenol. To treat pain and swelling, you can take ibuprofen (sample brand names: Advil, Motrin). But people who have certain conditions or take certain medicines should not take ibuprofen. If you are unsure, ask your doctor or nurse if you can take ibuprofen. -
Foreign Body Insertions: a Review
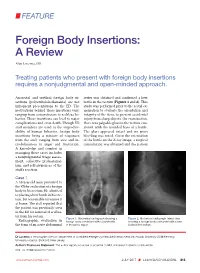
FEATURE Foreign Body Insertions: A Review Alan Lucerna, DO Treating patients who present with foreign body insertions requires a nonjudgmental and open-minded approach. Anorectal and urethral foreign body in- series was obtained and confirmed a beer sertions (polyembolokoilamania) are not bottle in the rectum (Figures 1 and 2). This infrequent presentations to the ED. The study was performed prior to the rectal ex- motivations behind these insertions vary, amination to evaluate the orientation and ranging from autoeroticism to reckless be- integrity of the item, to prevent accidental havior. These insertions can lead to major injury from sharp objects. On examination, complications and even death. Though ED there was palpable glass in the rectum con- staff members are used to the unpredict- sistent with the rounded base of a bottle. ability of human behavior, foreign body The glass appeared intact and no gross insertions bring a mixture of responses bleeding was noted. Given the orientation from the staff, ranging from awe and in- of the bottle on the X-ray image, a surgical credulousness to anger and frustration. consultation was obtained and the patient A knowledge and comfort in managing these cases includes a nonjudgmental triage assess- ment, collective professional- ism, and self-awareness of the staff’s reaction. Case 1 A 58-year-old man presented to the ED for evaluation of a foreign body in his rectum. He admitted to placing a beer bottle in his rec- tum, but was unable to remove it at home. The staff reported that the patient was previously seen in the ED for removal of a vibra- tor from his rectum. -

Foreign Rectal Body – Systematic Review and Meta-Analysis
REVIEW 61 Foreign rectal body – Systematic review and meta-analysis M. Ploner1, A. Gardetto2, F. Ploner3, M. Scharl4, S. Shoap5, H. C. Bäcker5 (1) Department of Anesthesiology and Intensiver Care, Cantonal Spital Lucerne, Lucerne, Switzerland ; (2) Department of Plastic Surgery, Hospital Sterzing, Sterzing, South Tirol, Italy ; (3) Department of Anesthesiology and Emergency Medicine, Hospital Sterzing, South Tirol, Italy ; (4) Department of Gastroenterology and Hepatology, University Hospital Zurich, University of Zurich, Swetzerland ; (5) Department of Orthopaedic Surgery, Columbia University Medical Center, New York, USA. Abstract instrumentation (7). The most common complication is a rectal injury, which can result from a variety of agents and Background : Self-inserted foreign rectal bodies are an objects (8). Often, nonsurgical removal of foreign bodies infrequent occurrence, however they present a serious dilemma to the surgeon, due to the variety of objects, and the difficulty of has been described to be successful – in 11% to 65% – extraction. The purpose of this study is to give a comprehensive (9), however, in many situations, a surgical treatment review of the literature regarding the epidemiology, diagnostic may be essential. There have been a variety of algorithms tools and therapeutic approaches of foreign rectal body insertion. Methods : A comprehensive systematic literature review on introduced for the management of extraction, however, Pubmed/ Medline and Google for ‘foreign bodies’ was performed because of the diversity of foreign bodies, improvisation, on January 14th 2018. A meta-analysis was carried out to evaluate as well creativity of the treating emergency physician the epidemiology, diagnostics and therapeutic techniques. 1,551 abstracts were identified, of which 54 articles were included. -
NEISS Coding Manual January 2018
NNEEIISSSS CCooddiinngg MMaannuuaall JJaannuuaarryy 22001188 NEISS – National Electronic Injury Surveillance System January 2018 Table of Contents Introduction ................................................................................................................................................. 1 General Instructions ................................................................................................................................... 1 General NEISS Reporting Rule .................................................................................................................. 1 Do Report .................................................................................................................................................. 1 Definitions .............................................................................................................................................. 2 Do Not Report ........................................................................................................................................... 3 Specific Coding Instructions ..................................................................................................................... 4 Medical Information Codes ........................................................................................................................ 4 Date of Treatment ..................................................................................................................................... 4 (8 spaces)................................................................................................................................................. -

Foreign Body Aspiration in Hong Kong Chinese Children
ORIGINAL Foreign body aspiration in Hong Kong Chinese ARTICLE children CME KK Chik 戚嘉琪 TY Miu 繆定逸 Objectives To describe and compare the demographic, clinical, radiological, CW Chan 陳振榮 and bronchoscopy features and outcomes of children with foreign body aspiration in early- and late-diagnosis groups, to report the reasons for delay in diagnoses, and to determine what objects are commonly aspirated. Design Retrospective study. Setting Department of Paediatrics, Queen Elizabeth Hospital, Hong Kong. Patients All children younger than the age of 18 years with foreign body aspiration admitted to the study hospital from 1 January 1993 to 31 May 2006. Results Sixteen (59%) of the patients were categorised into the early- diagnosis group (correctly diagnosed foreign body aspiration <7 days of symptom onset) and 11 (41%) into the late-diagnosis group (correctly diagnosed ≥7 days after symptom onset). The common clinical manifestations of foreign body aspiration were persistent cough (100%) and history of choking (74%). Most children (82%) in the late-diagnosis group and 25% in early- diagnosis group (P=0.004) were misdiagnosed as respiratory infections and asthma. Intrabronchial granulation was more common in the late-diagnosis group (13% vs 55%, P=0.033). Peanuts and watermelon seeds accounted for 85% of the aspirations; 63% of the foreign body aspirations occurred around the Chinese New Year festival. Conclusion Foreign body aspiration is difficult to diagnose in children. Misdiagnosis as asthma and respiratory infection can delay treatment and result in intrabronchial granuloma. We therefore suggest early bronchoscopy in suspicious cases. Parents should be cautious when giving peanuts and watermelon seeds to their children. -

Injury Description Codes Nature of Injury
Injury Description Codes Nature of Injury Code Narrative Description I. Specific Injury * 01. No Physical Injury i.e., Glasses, contact lenses, artificial appliance, replacement of artificial appliance 02. Amputation Cut off extremity, digit, protruding part of body, usually by surgery, i.e. leg, arm 03. Angina Pectoris Chest pain 04. Burn (Heat) Burns or scald. The effect of contact with hot substances. (Chemical) burns. tissue damage resulting from the corrosive action chemicals, fume, etc., (acids, alkalies) 07. Concussion Brain, cerebral 10. Contusion Bruise - intact skin surface hematoma 13. Crushing To grind, pound or break into small bits 16. Dislocation Pinched nerve, slipped/ruptured disc, herniated disc, sciatica, complete tear, HNP subluxtion, MD dislocation 19. Electric Shock Electrocution 22. Enucleation Removal of organ or tumor 25. Foreign Body * 28. Fracture Breaking of a bone or cartilage 30. Freezing Frostbite and other effects of exposure to low temperature 31. Hearing Loss or Impairment Traumatic only. A separate injury, not the sequelae of another injury 32. Heat Prostration Heat stroke, sun stroke, heat exhaustion, heat cramps and other effects of environmental heat. does not include sunburn 34. Hernia The abnormal protrusion of an organ or part through the containing wall of its cavity 36. Infection The invasion of a host by organisms such as bacteria, fungi, viruses, mold, protozoa or insects, with or without manifest disease. 37. Inflammation The reaction of tissue to injury characterized clinically by heat, swelling, redness and pain *Description intentionally left blank. May 25, 2021 Injury Description Codes Nature of Injury 38. Adverse reaction to a vaccination or * inoculation 40. -

Foreign Body Imaging-Experience with 6 Cases of Retained Foreign Bodies in the Emergency
Arch Clin Med Case Rep 2020; 4 (5): 952-968 DOI: 10.26502/acmcr.96550285 Case Series Foreign Body Imaging-Experience with 6 Cases of Retained Foreign Bodies in the Emergency Radiology Unit Muniraju Maralakunte MD1, Uma Debi MD1*, Lokesh Singh MD1, Himanshu Pruthi MD1, Vikas Bhatia MD, DNB DM1, Gita Devi MD1, Sandhu MS MD1 2Department of Radio diagnosis, PGIMER, Chandigarh, India *Corresponding Author: Dr. Uma Debi, Radiodiagnosis and Imaging, PGIMER, Chandigarh, India, Tel: 0091- 172-2756381; Fax: 0091-172-2745768; E-mail: [email protected] Received: 22 June 2020; Accepted: 14 August 2020; Published: 21 September 2020 Abstract Introduction: Retained foreign bodies are the external objects lying within the body, which are placed with voluntary or involuntary intentions. The involuntarily or accidentally, and complicated cases with the retained foreign body may come to the emergency services, which may require rapid and adequate imaging assessment. Materials and methods: We share our experience with six different cases with retained foreign bodies, who visited emergency radiological services with acute presentation of symptoms. The choice of radiological investigation considered based on the clinical presentation of the subjects with a retained foreign body. Conclusion: Patients with the retained foreign body may present acute symptoms to the emergency medical or surgical services, radiologists play a central role in rapid imaging evaluation. Radiological investigation plays a crucial role in identification, localization, characterization, and reporting the complication of the retained foreign bodies, and in many scenarios, radiological investigations may expose the unsuspected or concealed foreign bodies in the human body. Ultimately radiological services are useful rapid assessment tools that aid in triage and guide in the medical or surgical management of patients with a retained foreign body. -

Early Recognition of Foreign Body Aspiration As the Cause of Cardiac Arrest
Hindawi Publishing Corporation Case Reports in Critical Care Volume 2016, Article ID 1329234, 4 pages http://dx.doi.org/10.1155/2016/1329234 Case Report Early Recognition of Foreign Body Aspiration as the Cause of Cardiac Arrest Muhammad Kashif, Hafiz Rizwan Talib Hashmi, and Misbahuddin Khaja Division of Pulmonary and Critical Care Medicine, Department of Medicine, Bronx Lebanon Hospital Center, Bronx, NY 10457, USA Correspondence should be addressed to Muhammad Kashif; [email protected] Received 20 December 2015; Revised 28 January 2016; Accepted 3 February 2016 Academic Editor: Ricardo Oliveira Copyright © 2016 Muhammad Kashif et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Foreign body aspiration (FBA) is uncommon in the adult population but can be a life-threatening condition. Clinical manifestations vary according to the degree of airway obstruction, and, in some cases, making the correct diagnosis requires a high level of clinical suspicion combined with a detailed history and exam. Sudden cardiac arrest after FBA may occur secondary to asphyxiation. We present a 48-year-old male with no history of cardiac disease brought to the emergency department after an out-of-hospital cardiac arrest (OHCA). The patient was resuscitated after 15 minutes of cardiac arrest. He was initially managed with therapeutic hypothermia (TH). Subsequent history suggested FBA as a possible etiology of the cardiac arrest, and fiberoptic bronchoscopy demonstrated a piece of meat and bone lodged in the left main stem bronchus. The foreign body was removed with the bronchoscope and the patient clinically improved with full neurological recovery. -
Using Injury Narrative with Tri-Code to Obtain Accurate Diagnosis Codes and Scoring
Injury Coding – Using Injury Narrative with Tri-Code to Obtain Accurate Diagnosis Codes and Scoring Injury Coding Webinar Series James Pou Product Strategy - Product Manager Digital Innovation - eso.com powered by Copyright © 2020 ESO Inc. All Rights Reserved. powered by Objectives • Search for and abstract the additional detail to support ICD10 Injury coding. • Enter narrative and code using Tri-Code to accurately assign ICD10-CM and AIS. © Copyright 2020 ESO Inc. All Rights Reserved. Tri-Code and Injury Coding in ICD10 powered by • Two methods of coding in Tri-Code • Code by narrative description of injury. Consists of the following: • One injury per line which includes: • Organ or body part • Description of injury • Extent of injury • Code by ICD10 injury code: • Enter each ICD10 Injury Diagnosis on a separate lines © Copyright 2020 ESO Inc. All Rights Reserved. Using Tri-Code powered by • Narrative Based Coding: • Complete set of Guidelines available –Tri-Code for ICD10 Guidelines – ICD10-CM with AIS 2005 Update 2008 • Includes detailed guidelines by AIS chapter. © Copyright 2020 ESO Inc. All Rights Reserved. powered by Narrative Development Guidelines • Cornerstone of accurate injury coding – Good abstraction of injuries from the medical record. • Abstraction Recommendations • Read entire patient chart – In particular focus on: • Radiological results • Operative reports (tells you what has been fixed that was injured) • Consult reports • Discharge abstracts • Autopsy reports (if can be obtained for deaths) © Copyright 2020 ESO Inc. -

Foreign Body Aspiration Presenting with Asthma-Like Symptoms
Himmelfarb Health Sciences Library, The George Washington University Health Sciences Research Commons Medicine Faculty Publications Medicine 2013 Foreign body aspiration presenting with asthma- like symptoms Jennifer C. Kam George Washington University Vikram Doriswamy Seton Hall University Javier F. Dieguez Seton Hall University Joan Dabu Seton Hall University Matthew holC ankeril Seton Hall University See next page for additional authors Follow this and additional works at: http://hsrc.himmelfarb.gwu.edu/smhs_medicine_facpubs Part of the Medicine and Health Sciences Commons Recommended Citation Kam, J.C., Doraiswamy, V., Dieguez, J.F., Dabu, J., Cholankeril, M., Govind, M., Miller, R., Adelman, M. (2013). Foreign body aspiration presenting with asthma-like symptoms. Case Reports in Medicine: 317104. This Journal Article is brought to you for free and open access by the Medicine at Health Sciences Research Commons. It has been accepted for inclusion in Medicine Faculty Publications by an authorized administrator of Health Sciences Research Commons. For more information, please contact [email protected]. Authors Jennifer C. Kam, Vikram Doriswamy, Javier F. Dieguez, Joan Dabu, Matthew Cholankeril, Mayur Govind, Richard Miller, and Marc Adelman This journal article is available at Health Sciences Research Commons: http://hsrc.himmelfarb.gwu.edu/smhs_medicine_facpubs/ 349 Hindawi Publishing Corporation Case Reports in Medicine Volume 2013, Article ID 317104, 4 pages http://dx.doi.org/10.1155/2013/317104 Case Report Foreign Body Aspiration Presenting