Cornea and External Disease Robert Cykiert, M.D
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Ocular Leishmaniasis Presenting As Chronic
perim Ex en l & ta a l ic O p in l h t C h f Journal of Clinical & Experimental a o l m l a o n l r o g u Ayele et al., J Clin Exp Ophthalmol 2015, 6:1 y o J Ophthalmology ISSN: 2155-9570 DOI: 10.4172/2155-9570.1000395 Case Report Open Access Ocular Leishmaniasis Presenting as Chronic Ulcerative Blepharoconjunctivitis: A Case Report Fisseha Admassu Ayele*, Yared Assefa Wolde, Tesfalem Hagos and Ermias Diro University of Gondar, Gondar, Amhara, Ethiopia *Corresponding author: Fisseha Admassu Ayele MD, University of Gondar, Gondar, Amhara 196, Ethiopia, Tel: 251911197786; E-mail: [email protected] Received date: Dec 01, 2014, Accepted date: Feb 02, 2015, Published date: Feb 05, 2015 Copyright: © 2015 Ayele FH, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Abstract Leishmaniasis is caused by unicellular eukaryotic obligate intracellular protozoa of the genus Leishmania that is endemic in over 98 countries in the world-most of which are developing countries including Ethiopia. It is transmitted by phlebotomine sandflies. The eye may be affected in cutaneous, mucocutaneous and Post Kala-Azar Dermal Leishmaniasis. We report a case of ocular leishmaniasis with eyelid and conjunctival involvement that had simulated ulcerative blepharoconjunctivitis not responding to conventional antibiotics. The patient was diagnosed by microscopy of a sample obtained via direct smear from the lesions. He was treated with systemic sodium stibogluconate (20 mg/kg/day) for 45 days and was clinically cured with this treatment. -

Case Report Descemet Stripping Endothelial Keratoplasty in a Patient with Keratoglobus and Chronic Hydrops Secondary to a Spontaneous Descemet Membrane Tear
Hindawi Publishing Corporation Case Reports in Ophthalmological Medicine Volume 2013, Article ID 697403, 5 pages http://dx.doi.org/10.1155/2013/697403 Case Report Descemet Stripping Endothelial Keratoplasty in a Patient with Keratoglobus and Chronic Hydrops Secondary to a Spontaneous Descemet Membrane Tear Anton M. Kolomeyer1 and David S. Chu1,2 1 The Institute of Ophthalmology and Visual Science, New Jersey Medical School, University of Medicine and Dentistry of New Jersey, Newark,NJ07103,USA 2 Metropolitan Eye Research and Surgery Institute, 540 Bergen Boulevard, Suite D, Palisades Park, NJ 07650, USA Correspondence should be addressed to David S. Chu; [email protected] Received 4 March 2013; Accepted 7 April 2013 Academic Editors: S. M. Johnson and S. Machida Copyright © 2013 A. M. Kolomeyer and D. S. Chu. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Purpose. To report the use of Descemet stripping endothelial keratoplasty (DSEK) in a patient with keratoglobus and chronic hydrops. Case Report. We describe a case of a 28-year-old man with bilateral keratoglobus and chronic hydrops in the right eye secondary to spontaneous Descemet membrane tear. The patient presented with finger counting (CF) vision, itching, foreign body sensation, and severe photophobia in the right eye. Peripheral corneal thinning with central corneal protrusion and Descemet mem- brane tear spanning from 4 to 7 o’clock was noted on slit lamp examination. The right eye cornea was 15 mm in the horizontal diam- eter. -

Glossary for Narrative Writing
Periodontal Assessment and Treatment Planning Gingival description Color: o pink o erythematous o cyanotic o racial pigmentation o metallic pigmentation o uniformity Contour: o recession o clefts o enlarged papillae o cratered papillae o blunted papillae o highly rolled o bulbous o knife-edged o scalloped o stippled Consistency: o firm o edematous o hyperplastic o fibrotic Band of gingiva: o amount o quality o location o treatability Bleeding tendency: o sulcus base, lining o gingival margins Suppuration Sinus tract formation Pocket depths Pseudopockets Frena Pain Other pathology Dental Description Defective restorations: o overhangs o open contacts o poor contours Fractured cusps 1 ww.links2success.biz [email protected] 914-303-6464 Caries Deposits: o Type . plaque . calculus . stain . matera alba o Location . supragingival . subgingival o Severity . mild . moderate . severe Wear facets Percussion sensitivity Tooth vitality Attrition, erosion, abrasion Occlusal plane level Occlusion findings Furcations Mobility Fremitus Radiographic findings Film dates Crown:root ratio Amount of bone loss o horizontal; vertical o localized; generalized Root length and shape Overhangs Bulbous crowns Fenestrations Dehiscences Tooth resorption Retained root tips Impacted teeth Root proximities Tilted teeth Radiolucencies/opacities Etiologic factors Local: o plaque o calculus o overhangs 2 ww.links2success.biz [email protected] 914-303-6464 o orthodontic apparatus o open margins o open contacts o improper -

Differentiate Red Eye Disorders
Introduction DIFFERENTIATE RED EYE DISORDERS • Needs immediate treatment • Needs treatment within a few days • Does not require treatment Introduction SUBJECTIVE EYE COMPLAINTS • Decreased vision • Pain • Redness Characterize the complaint through history and exam. Introduction TYPES OF RED EYE DISORDERS • Mechanical trauma • Chemical trauma • Inflammation/infection Introduction ETIOLOGIES OF RED EYE 1. Chemical injury 2. Angle-closure glaucoma 3. Ocular foreign body 4. Corneal abrasion 5. Uveitis 6. Conjunctivitis 7. Ocular surface disease 8. Subconjunctival hemorrhage Evaluation RED EYE: POSSIBLE CAUSES • Trauma • Chemicals • Infection • Allergy • Systemic conditions Evaluation RED EYE: CAUSE AND EFFECT Symptom Cause Itching Allergy Burning Lid disorders, dry eye Foreign body sensation Foreign body, corneal abrasion Localized lid tenderness Hordeolum, chalazion Evaluation RED EYE: CAUSE AND EFFECT (Continued) Symptom Cause Deep, intense pain Corneal abrasions, scleritis, iritis, acute glaucoma, sinusitis, etc. Photophobia Corneal abrasions, iritis, acute glaucoma Halo vision Corneal edema (acute glaucoma, uveitis) Evaluation Equipment needed to evaluate red eye Evaluation Refer red eye with vision loss to ophthalmologist for evaluation Evaluation RED EYE DISORDERS: AN ANATOMIC APPROACH • Face • Adnexa – Orbital area – Lids – Ocular movements • Globe – Conjunctiva, sclera – Anterior chamber (using slit lamp if possible) – Intraocular pressure Disorders of the Ocular Adnexa Disorders of the Ocular Adnexa Hordeolum Disorders of the Ocular -

Understanding Corneal Blindness
Understanding Corneal Blindness The cornea copes very well with minor injuries or abrasions. If the highly sensitive cornea is scratched, healthy cells slide over quickly and patch the injury before infection occurs and vision is affected. If the scratch penetrates the cornea more deeply, however, the healing process will take longer, at times resulting in greater pain, blurred vision, tearing, redness, and extreme sensitivity to light. These symptoms require professional treatment. Deeper scratches can also cause corneal scarring, resulting in a haze on the cornea that can greatly impair vision. In this case, a corneal transplant may be needed. Corneal Diseases and Disorders that May Require a Transplant Corneal Infections. Sometimes the cornea is damaged after a foreign object has penetrated the tissue, such as from a poke in the eye. At other times, bacteria or fungi from a contaminated contact lens can pass into the cornea. Situations like these can cause painful inflammation and corneal infections called keratitis. These infections can reduce visual clarity, produce corneal discharges, and perhaps erode the cornea. Corneal infections can also lead to corneal scarring, which can impair vision and may require a corneal transplant. Fuchs' Dystrophy. Fuchs' Dystrophy occurs when endothelial cells gradually deteriorate without any apparent reason. As more endothelial cells are lost over the years, the endothelium becomes less efficient at pumping water out of the stroma (the middle layers of the cornea). This causes the cornea to swell and distort vision. Eventually, the epithelium also takes on water, resulting in pain and severe visual impairment. Epithelial swelling damages vision by changing the cornea's normal curvature, and causing a sightimpairing haze to appear in the tissue. -
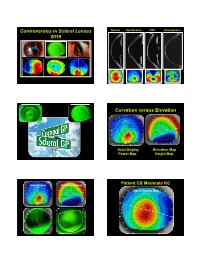
Controversies in Scleral Lenses 2019 Curvature Versus Elevation
Controversies in Scleral Lenses Normal Keratoconus PMD Keratoglobus 2019 Curvature versus Elevation Axial Display Elevation Map Power Map Height Map Axial Display Elevation Display Patient CB Moderate KC Axial Display Map +180um +180 +379 +379um Elevation Display -110 - 276 Elevation Map 655 Above the 290 microns Micron Sphere Height -276um Differential Depression Below the -110um Sphere N = 87 Patients 127 CL Fits Less than 350um Greater than 350um Patients with 350um or less of corneal elevation difference (along the greatest meridian of change) have an 88.2% chance of success with a corneal GP lens. The Re-Birth of Scleral Lenses Glass Scleral Lenses 1887 Molding Glass Scleral Lenses Average 8.5 High DK Scleral Materials Traditional Corneal / Scleral • Menicon Z Dk = 163 Shape • B & L, Boston XO2 DK = 141 • Contamac, Optimum Extreme DK = 125 • B & L, Boston XO DK = 100 • Paragon HDS 100 DK = 100 • Contamac, Optimum Extra DK = 100 • Lagado, Tyro -97 DK = 97 Scleral Shape Cone Angle Circa 1948 Klaus Pfortner New Understandings Argentina Scleral Lens Fitting Objectives Anatomy of a Scleral Lens 1. Central Vault Zone (250 to 400 microns) 2. Peripheral Lift Zone 4 3 2 1 2 3 4 3. Limbal Lift Zone 4. Scleral Landing Zone Ocular Surface Disease Scleral Lens Indications Scleral Irregular Astigmatism Lens • Keratoconus Indications • Pellucid Marginal Degeneration • Post Corneal Trauma • Post keratoplasty • Post K-Pro • Post Refractive Surgery RK, PRK and LASIK • Post HSV and HZV • Athletes • GP stability (rocking) issues Corneal Irregularity -

Non-Syndromic Occurrence of True Generalized Microdontia with Mandibular Mesiodens - a Rare Case Seema D Bargale* and Shital DP Kiran
Bargale and Kiran Head & Face Medicine 2011, 7:19 http://www.head-face-med.com/content/7/1/19 HEAD & FACE MEDICINE CASEREPORT Open Access Non-syndromic occurrence of true generalized microdontia with mandibular mesiodens - a rare case Seema D Bargale* and Shital DP Kiran Abstract Abnormalities in size of teeth and number of teeth are occasionally recorded in clinical cases. True generalized microdontia is rare case in which all the teeth are smaller than normal. Mesiodens is commonly located in maxilary central incisor region and uncommon in the mandible. In the present case a 12 year-old boy was healthy; normal in appearance and the medical history was noncontributory. The patient was examined and found to have permanent teeth that were smaller than those of the average adult teeth. The true generalized microdontia was accompanied by mandibular mesiodens. This is a unique case report of non-syndromic association of mandibular hyperdontia with true generalized microdontia. Keywords: Generalised microdontia, Hyperdontia, Permanent dentition, Mandibular supernumerary tooth Introduction [Ullrich-Turner syndrome], Chromosome 13[trisomy 13], Microdontia is a rare phenomenon. The term microdontia Rothmund-Thomson syndrome, Hallermann-Streiff, Oro- (microdentism, microdontism) is defined as the condition faciodigital syndrome (type 3), Oculo-mandibulo-facial of having abnormally small teeth [1]. According to Boyle, syndrome, Tricho-Rhino-Phalangeal, type1 Branchio- “in general microdontia, the teeth are small, the crowns oculo-facial syndrome. short, and normal contact areas between the teeth are fre- Supernumerary teeth are defined as any supplementary quently missing” [2] Shafer, Hine, and Levy [3] divided tooth or tooth substance in addition to usual configuration microdontia into three types: (1) Microdontia involving of twenty deciduous and thirty two permanent teeth [7]. -

Diagnostic Code Descriptions (ICD9)
INFECTIONS AND PARASITIC DISEASES INTESTINAL AND INFECTIOUS DISEASES (001 – 009.3) 001 CHOLERA 001.0 DUE TO VIBRIO CHOLERAE 001.1 DUE TO VIBRIO CHOLERAE EL TOR 001.9 UNSPECIFIED 002 TYPHOID AND PARATYPHOID FEVERS 002.0 TYPHOID FEVER 002.1 PARATYPHOID FEVER 'A' 002.2 PARATYPHOID FEVER 'B' 002.3 PARATYPHOID FEVER 'C' 002.9 PARATYPHOID FEVER, UNSPECIFIED 003 OTHER SALMONELLA INFECTIONS 003.0 SALMONELLA GASTROENTERITIS 003.1 SALMONELLA SEPTICAEMIA 003.2 LOCALIZED SALMONELLA INFECTIONS 003.8 OTHER 003.9 UNSPECIFIED 004 SHIGELLOSIS 004.0 SHIGELLA DYSENTERIAE 004.1 SHIGELLA FLEXNERI 004.2 SHIGELLA BOYDII 004.3 SHIGELLA SONNEI 004.8 OTHER 004.9 UNSPECIFIED 005 OTHER FOOD POISONING (BACTERIAL) 005.0 STAPHYLOCOCCAL FOOD POISONING 005.1 BOTULISM 005.2 FOOD POISONING DUE TO CLOSTRIDIUM PERFRINGENS (CL.WELCHII) 005.3 FOOD POISONING DUE TO OTHER CLOSTRIDIA 005.4 FOOD POISONING DUE TO VIBRIO PARAHAEMOLYTICUS 005.8 OTHER BACTERIAL FOOD POISONING 005.9 FOOD POISONING, UNSPECIFIED 006 AMOEBIASIS 006.0 ACUTE AMOEBIC DYSENTERY WITHOUT MENTION OF ABSCESS 006.1 CHRONIC INTESTINAL AMOEBIASIS WITHOUT MENTION OF ABSCESS 006.2 AMOEBIC NONDYSENTERIC COLITIS 006.3 AMOEBIC LIVER ABSCESS 006.4 AMOEBIC LUNG ABSCESS 006.5 AMOEBIC BRAIN ABSCESS 006.6 AMOEBIC SKIN ULCERATION 006.8 AMOEBIC INFECTION OF OTHER SITES 006.9 AMOEBIASIS, UNSPECIFIED 007 OTHER PROTOZOAL INTESTINAL DISEASES 007.0 BALANTIDIASIS 007.1 GIARDIASIS 007.2 COCCIDIOSIS 007.3 INTESTINAL TRICHOMONIASIS 007.8 OTHER PROTOZOAL INTESTINAL DISEASES 007.9 UNSPECIFIED 008 INTESTINAL INFECTIONS DUE TO OTHER ORGANISMS -

Corneal Ectasia
Corneal Ectasia Secretary for Quality of Care Anne L. Coleman, MD, PhD Academy Staff Nicholas P. Emptage, MAE Nancy Collins, RN, MPH Doris Mizuiri Jessica Ravetto Flora C. Lum, MD Medical Editor: Susan Garratt Design: Socorro Soberano Approved by: Board of Trustees September 21, 2013 Copyright © 2013 American Academy of Ophthalmology® All rights reserved AMERICAN ACADEMY OF OPHTHALMOLOGY and PREFERRED PRACTICE PATTERN are registered trademarks of the American Academy of Ophthalmology. All other trademarks are the property of their respective owners. This document should be cited as follows: American Academy of Ophthalmology Cornea/External Disease Panel. Preferred Practice Pattern® Guidelines. Corneal Ectasia. San Francisco, CA: American Academy of Ophthalmology; 2013. Available at: www.aao.org/ppp. Preferred Practice Pattern® guidelines are developed by the Academy’s H. Dunbar Hoskins Jr., MD Center for Quality Eye Care without any external financial support. Authors and reviewers of the guidelines are volunteers and do not receive any financial compensation for their contributions to the documents. The guidelines are externally reviewed by experts and stakeholders before publication. Corneal Ectasia PPP CORNEA/EXTERNAL DISEASE PREFERRED PRACTICE PATTERN DEVELOPMENT PROCESS AND PARTICIPANTS The Cornea/External Disease Preferred Practice Pattern® Panel members wrote the Corneal Ectasia Preferred Practice Pattern® guidelines (“PPP”). The PPP Panel members discussed and reviewed successive drafts of the document, meeting in person twice and conducting other review by e-mail discussion, to develop a consensus over the final version of the document. Cornea/External Disease Preferred Practice Pattern Panel 2012–2013 Robert S. Feder, MD, Co-chair Stephen D. McLeod, MD, Co-chair Esen K. -

Onchocerciasis
11 ONCHOCERCIASIS ADRIAN HOPKINS AND BOAKYE A. BOATIN 11.1 INTRODUCTION the infection is actually much reduced and elimination of transmission in some areas has been achieved. Differences Onchocerciasis (or river blindness) is a parasitic disease in the vectors in different regions of Africa, and differences in cause by the filarial worm, Onchocerca volvulus. Man is the the parasite between its savannah and forest forms led to only known animal reservoir. The vector is a small black fly different presentations of the disease in different areas. of the Simulium species. The black fly breeds in well- It is probable that the disease in the Americas was brought oxygenated water and is therefore mostly associated with across from Africa by infected people during the slave trade rivers where there is fast-flowing water, broken up by catar- and found different Simulium flies, but ones still able to acts or vegetation. All populations are exposed if they live transmit the disease (3). Around 500,000 people were at risk near the breeding sites and the clinical signs of the disease in the Americas in 13 different foci, although the disease has are related to the amount of exposure and the length of time recently been eliminated from some of these foci, and there is the population is exposed. In areas of high prevalence first an ambitious target of eliminating the transmission of the signs are in the skin, with chronic itching leading to infection disease in the Americas by 2012. and chronic skin changes. Blindness begins slowly with Host factors may also play a major role in the severe skin increasingly impaired vision often leading to total loss of form of the disease called Sowda, which is found mostly in vision in young adults, in their early thirties, when they northern Sudan and in Yemen. -

The Simplified Trachoma Grading System, Amended Anthony W Solomon,A Amir B Kello,B Mathieu Bangert,A Sheila K West,C Hugh R Taylor,D Rabebe Tekeraoie & Allen Fosterf
PolicyPolicy & practice & practice The simplified trachoma grading system, amended Anthony W Solomon,a Amir B Kello,b Mathieu Bangert,a Sheila K West,c Hugh R Taylor,d Rabebe Tekeraoie & Allen Fosterf Abstract A simplified grading system for trachoma was published by the World Health Organization (WHO) in 1987. Intended for use by non-specialist personnel working at community level, the system includes five signs, each of which can be present or absent in any eye: (i) trachomatous trichiasis; (ii) corneal opacity; (iii) trachomatous inflammation—follicular; (iv) trachomatous inflammation—intense; and (v) trachomatous scarring. Though neither perfectly sensitive nor perfectly specific for trachoma, these signs have been essential tools for identifying populations that need interventions to eliminate trachoma as a public health problem. In 2018, at WHO’s 4th global scientific meeting on trachoma, the definition of one of the signs, trachomatous trichiasis, was amended to exclude trichiasis that affects only the lower eyelid. This paper presents the amended system, updates its presentation, offers notes on its use and identifies areas of ongoing debate. Introduction (ii) corneal opacity; (iii) trachomatous inflammation—fol- licular; (iv) trachomatous inflammation—intense; and (v) tra- Trachoma is the most important infectious cause of blindness.1 chomatous scarring.19 Trachomatous inflammation—follicular Repeated conjunctival infection2 with particular strains of and trachomatous inflammation—intense are signs of active Chlamydia trachomatis3–5 -

An Algorithm to Detect Kayser-Fleischer Ring in Human Eye for Diagnosing Wilson Disease
ISSN: 2319-8753 International Journal of Innovative Research in Science, Engineering and Technology (An ISO 3297: 2007 Certified Organization) Vol. 3, Issue 5, May 2014 An Algorithm to Detect Kayser-Fleischer Ring in Human Eye for Diagnosing Wilson Disease 1S.Tharageshwari, 2 D.Sasikala 1PG scholar, Department Of ECE, Vivekanandha College of Engineering For Women, Namakkal , Tamil nadu, India. 2Associate Professor, Department Of ECE, Vivekanandha College of Engineering For Women, Namakkal, Tamil nadu, India. ABSTRACT-An eye image is segmented by JSEG (J measure based segmentation) algorithm without the manual parameter adjustment and simplifies texture and color for detecting the Kayser-Fleischer ring in diagnosing Wilson Disease. Segmentation with this algorithm passes through two major stages, namely color quantization and spatial segmentation as first stage and region growing and region merging as secondary stage. The biometric measurement provides information on the percentage of the extent of the cornea tissue affected from the copper accumulation. This algorithm detects the presence of symptoms reducing occurrence of false-negative diagnoses and improves accuracy of actual methods used in practice like slit lamp method. The described techniques reduces possible interpretation errors and assists doctor to diagnose the pathology. INDEX TERMS – Wilson disease, Kayser-Fleischer Ring, segmentation, Biometric measurement. I. INTRODUCTION Wilson disease is an autosomal recessive genetic disorder that prevent the body from getting rid of extra copper. A small amount of copper obtained from food is needed to stay healthy, but too much copper is poisonous. When the copper storage capacity of the liver is surpassed, copper is passed into the bloodstream and travels to the other organs-including the brain, kidney, and eyes.