Postgraduate Examination Skills: Clubbing
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Identifying COPD by Crackle Characteristics
BMJ Open Resp Res: first published as 10.1136/bmjresp-2020-000852 on 5 March 2021. Downloaded from Respiratory epidemiology Inspiratory crackles—early and late— revisited: identifying COPD by crackle characteristics Hasse Melbye ,1 Juan Carlos Aviles Solis,1 Cristina Jácome,2 Hans Pasterkamp3 To cite: Melbye H, Aviles ABSTRACT Key messages Solis JC, Jácome C, et al. Background The significance of pulmonary crackles, Inspiratory crackles— by their timing during inspiration, was described by Nath early and late—revisited: and Capel in 1974, with early crackles associated with What is the key question? identifying COPD by bronchial obstruction and late crackles with restrictive ► In the diagnosis of chronic obstructive pulmonary crackle characteristics. defects. Crackles are also described as ‘fine’ or disease (COPD), is it more useful to focus on the tim- BMJ Open Resp Res ‘coarse’. We aimed to evaluate the usefulness of crackle ing of crackles than on the crackle type? 2021;8:e000852. doi:10.1136/ bmjresp-2020-000852 characteristics in the diagnosis of chronic obstructive What is the bottom line? pulmonary disease (COPD). ► Pulmonary crackles are divided into two types, ‘fine’ Methods In a population-based study, lung sounds Received 2 December 2020 and ‘coarse’ and coarse inspiratory crackles are re- Revised 2 February 2021 were recorded at six auscultation sites and classified in garded to be typical of COPD. In bronchial obstruc- Accepted 5 February 2021 participants aged 40 years or older. Inspiratory crackles tion crackles tend to appear early in inspiration, and were classified as ‘early’ or ‘late and into the types’ this characteristic of the crackle might be easier for ‘coarse’ and ‘fine’ by two observers. -

Approach to Cyanosis in a Neonate.Pdf
PedsCases Podcast Scripts This podcast can be accessed at www.pedscases.com, Apple Podcasting, Spotify, or your favourite podcasting app. Approach to Cyanosis in a Neonate Developed by Michelle Fric and Dr. Georgeta Apostol for PedsCases.com. June 29, 2020 Introduction Hello, and welcome to this pedscases podcast on an approach to cyanosis in a neonate. My name is Michelle Fric and I am a fourth-year medical student at the University of Alberta. This podcast was made in collaboration with Dr. Georgeta Apostol, a general pediatrician at the Royal Alexandra Hospital Pediatrics Clinic in Edmonton, Alberta. Cyanosis refers to a bluish discoloration of the skin or mucous membranes and is a common finding in newborns. It is a clinical manifestation of the desaturation of arterial or capillary blood and may indicate serious hemodynamic instability. It is important to have an approach to cyanosis, as it can be your only sign of a life-threatening illness. The goal of this podcast is to develop this approach to a cyanotic newborn with a focus on these can’t miss diagnoses. After listening to this podcast, the learner should be able to: 1. Define cyanosis 2. Assess and recognize a cyanotic infant 3. Develop a differential diagnosis 4. Identify immediate investigations and management for a cyanotic infant Background Cyanosis can be further broken down into peripheral and central cyanosis. It is important to distinguish these as it can help you to formulate a differential diagnosis and identify cases that are life-threatening. Peripheral cyanosis affects the distal extremities resulting in blue color of the hands and feet, while the rest of the body remains pinkish and well perfused. -

Age-Related Pulmonary Crackles (Rales) in Asymptomatic Cardiovascular Patients
Age-Related Pulmonary Crackles (Rales) in Asymptomatic Cardiovascular Patients 1 Hajime Kataoka, MD ABSTRACT 2 Osamu Matsuno, MD PURPOSE The presence of age-related pulmonary crackles (rales) might interfere 1Division of Internal Medicine, with a physician’s clinical management of patients with suspected heart failure. Nishida Hospital, Oita, Japan We examined the characteristics of pulmonary crackles among patients with stage A cardiovascular disease (American College of Cardiology/American Heart 2Division of Respiratory Disease, Oita University Hospital, Oita, Japan Association heart failure staging criteria), stratifi ed by decade, because little is known about these issues in such patients at high risk for congestive heart failure who have no structural heart disease or acute heart failure symptoms. METHODS After exclusion of comorbid pulmonary and other critical diseases, 274 participants, in whom the heart was structurally (based on Doppler echocar- diography) and functionally (B-type natriuretic peptide <80 pg/mL) normal and the lung (X-ray evaluation) was normal, were eligible for the analysis. RESULTS There was a signifi cant difference in the prevalence of crackles among patients in the low (45-64 years; n = 97; 11%; 95% CI, 5%-18%), medium (65-79 years; n = 121; 34%; 95% CI, 27%-40%), and high (80-95 years; n = 56; 70%; 95% CI, 58%-82%) age-groups (P <.001). The risk for audible crackles increased approximately threefold every 10 years after 45 years of age. During a mean fol- low-up of 11 ± 2.3 months (n = 255), the short-term (≤3 months) reproducibility of crackles was 87%. The occurrence of cardiopulmonary disease during follow-up included cardiovascular disease in 5 patients and pulmonary disease in 6. -

September-Sunshine-Line-2021
The Sunshine 186 Main St STE 2 * Brookville, PA 15825 Phone:(814) 849-3096 1-800-852-8036 Line www.jcaaa.org Find us on Facebook: @JeffersonCountyAAA Want to receive our newsletter by email? Volume 7 Issue 9 September 2021 Register on our website or call us! FREE Community Workshop Presentation: Get Ready for Medicare: The Basics for People Who are Joining Already r Enrolled Jefferson County Area Agency on Aging Medicare Education and Decision Insight Program September 8th 6:00pm-7:00pm Brookville Heritage House September 16th 10:00am-11:00am Punxy Area Senior Center September 17th 11:00am-12:00pm Reynoldsville Foundry Senior Center September 22nd 11:00am-12:00pm Brockway Depot Senior Center Call Mindy at 814-849-3096 Ext 232 to sign up What is Medicare Education and Decision Insight (PA-MEDI) Medicare Education and Decision Insight (PA MEDI) is the State Health Insurance Assistance Program in Pennsylvania. We provide free, unbiased insurance counseling to people on Medicare. PA MEDI counselors are specifically trained to answer any questions about your coverage.We provide you with clear, easy to understand information about your Medicare options and can assist in comparing plans. We will also screen you to see if you qualify for any financial assistance programs to get help paying for your prescription drugs or Part B premium. You will have a better understanding of: • Medicare • Part A, B and C • An Advantage Plan • Savings programs • How to avoid penalties • And much more 2 September 2021 Pennsylvania 211: Get Connected. Get Help. ™ If you need to connect with resources in your community, but don’t know where to look, PA 211 is a great place to start. -

Dermatologic Findings in 16 Patients with Cockayne Syndrome and Cerebro-Oculo-Facial-Skeletal Syndrome
Research Case Report/Case Series Dermatologic Findings in 16 Patients With Cockayne Syndrome and Cerebro-Oculo-Facial-Skeletal Syndrome Eric Frouin, MD; Vincent Laugel, MD, PhD; Myriam Durand, MSc; Hélène Dollfus, MD, PhD; Dan Lipsker, MD, PhD Supplemental content at IMPORTANCE Cockayne syndrome (CS) and cerebro-oculo-facial-skeletal (COFS) syndrome jamadermatology.com are autosomal recessive diseases that belong to the family of nucleotide excision repair disorders. Our aim was to describe the cutaneous phenotype of patients with these rare diseases. OBSERVATIONS A systematic dermatologic examination of 16 patients included in a European study of CS was performed. The patients were aged 1 to 28 years. Six patients (38%) had mutations in the Cockayne syndrome A (CSA) gene, and the remaining had Cockayne syndrome B (CSB) gene mutations. Fourteen patients were classified clinically as having CS and 2 as having COFS syndrome. Photosensitivity was present in 75% of the patients and was characterized by sunburn after brief sun exposure. Six patients developed symptoms after short sun exposure through a windshield. Six patients had pigmented macules on sun-exposed skin, but none developed a skin neoplasm. Twelve patients (75%) displayed cyanotic acral edema of the extremities. Eight patients had nail dystrophies and 7 had hair anomalies. CONCLUSIONS AND RELEVANCE The dermatologic findings of 16 cases of CS and COFS Author Affiliations: Author syndrome highlight the high prevalence of photosensitivity and hair and nail disorders. affiliations are listed at the end of this Cyanotic acral edema was present in 75% of our patients, a finding not previously reported article. in CS. Corresponding Author: Eric Frouin, MD, Service d’Anatomie et Cytologie Pathologiques, Université de JAMA Dermatol. -

Digital Clubbing
Review Article Digital clubbing Malay Sarkar, D. M. Mahesh1, Irappa Madabhavi2 Department of Pulmonary Medicine, Indira Gandhi Medical College, Shimla, 1Department of Endocrinology, Jawaharlal Institute of Postgraduate Medical Education and Research, Pondicherry, 2Post Graduate Student (Medicine), Indira Gandhi Medical College, Shimla, India ABSTRACT Digital clubbing is an ancient and important clinical signs in medicine. Although clubbed fingers are mostly asymptomatic, it often predicts the presence of some dreaded underlying diseases. Its exact pathogenesis is not known, but platelet‑derived growth factor and vascular endothelial growth factor are recently incriminated in its causation. The association of digital clubbing with various disease processes and its clinical implications are discussed in this review. KEY WORDS: Cancer, digital clubbing, hypertrophic osteoarthropathy, megakaryocytes, vascular endothelial growth factor Address for correspondence: Dr. Malay Sarkar, Department of Pulmonary Medicine, Indira Gandhi Medical College, Shimla ‑ 171 001, India. E‑mail: [email protected] INTRODUCTION long bones and occasional painful joint enlargement. It was initially known as hypertrophic pulmonary Digital clubbing is characterized by a focal bulbous osteoarthropathy (HPOA) based on the fact that majority enlargement of the terminal segments of the fingers of cases of HOA are due to malignant thoracic tumors. and/or toes due to proliferation of connective tissue The term “pulmonary” was later abandoned as it was between nail matrix and the distal phalanx. It results in realized that the skeletal syndrome may occur in several increase in both anteroposterior and lateral diameter of non‑pulmonary diseases and even may occur without the nails.[1] Clubbed fingers are also known as watch‑glass any underlying illness. -

Assessing and Managing Lung Disease and Sleep Disordered Breathing in Children with Cerebral Palsy Paediatric Respiratory Review
Paediatric Respiratory Reviews 10 (2009) 18–24 Contents lists available at ScienceDirect Paediatric Respiratory Reviews CME Article Assessing and managing lung disease and sleep disordered breathing in children with cerebral palsy Dominic A. Fitzgerald 1,3,*, Jennifer Follett 2, Peter P. Van Asperen 1,3 1 Department of Respiratory Medicine, University of Sydney, Sydney, New South Wales, Australia 2 Department of Physiotherapy, The Children’s Hospital at Westmead, University of Sydney, Sydney, New South Wales, Australia 3 The Children’s Hospital at Westmead Clinical School, Discipline of Paediatrics & Child Health, University of Sydney, Sydney, New South Wales, Australia EDUCATIONAL AIMS To appreciate the insidious evolution of suppurative lung disease in children with cerebral palsy (CP). To be familiar with the management of excessive oral secretions in children with CP. To understand the range of sleep problems that are more commonly seen in children with CP. To gain an understanding of the use of non-invasive respiratory support for the management of airway clearance and sleep disordered breathing in children with CP. ARTICLE INFO SUMMARY Keywords: The major morbidity and mortality associated with cerebral palsy (CP) relates to respiratory compromise. Cerebral palsy This manifests through repeated pulmonary aspiration, airway colonization with pathogenic bacteria, Pulmonary aspiration the evolution of bronchiectasis and sleep disordered breathing. An accurate assessment involving a Suppurative lung disease multidisciplinary approach and relatively simple interventions for these conditions can lead to Physiotherapy significant improvements in the quality of life of children with CP as well as their parents and carers. This Airway clearance techniques Obstructive sleep apnoea review highlights the more common problems and potential therapies with regard to suppurative lung Sleep disordered breathing disease and sleep disordered breathing in children with CP. -

Problems in Family Practice
problems in Family Practice Coughing in Childhood Hyman Sh ran d , M D Cambridge, M assachusetts Coughing in childhood is a common complaint involving a wide spectrum of underlying causes which require a thorough and rational approach by the physician. Most children who cough have relatively simple self-limiting viral infections, but some may have serious disease. A dry environment, allergic factors, cystic fibrosis, and other major illnesses must always be excluded. A simple clinical approach, and the sensible use of appropriate investigations, is most likely to succeed in finding the cause, which can allow precise management. The cough reflex as part of the defense mechanism of the respiratory tract is initiated by mucosal changes, secretions or foreign material in the pharynx, larynx, tracheobronchial Table 1. Persistent Cough — Causes in Childhood* tree, pleura, or ear. Acting as the “watchdog of the lungs,” the “good” cough prevents harmful agents from Common Uncommon Rare entering the respiratory tract; it also helps bring up irritant material from Environmental Overheating with low humidity the airway. The “bad” cough, on the Allergens other hand, serves no useful purpose Pollution Tobacco smoke and, if persistent, causes fatigue, keeps Upper Respiratory Tract the child (and parents) awake, inter Recurrent viral URI Pertussis Laryngeal stridor feres with feeding, and induces vomit Rhinitis, Pharyngitis Echo 12 Vocal cord palsy Allergic rhinitis Nasal polyp Vascular ring ing. It is best suppressed. Coughs and Prolonged use of nose drops Wax in ear colds constitute almost three quarters Sinusitis of all illness in young children. The Lower Respiratory Tract Asthma Cystic fibrosis Rt. -

Review of Systems
code: GF004 REVIEW OF SYSTEMS First Name Middle Name / MI Last Name Check the box if you are currently experiencing any of the following : General Skin Respiratory Arthritis/Rheumatism Abnormal Pigmentation Any Lung Troubles Back Pain (recurrent) Boils Asthma or Wheezing Bone Fracture Brittle Nails Bronchitis Cancer Dry Skin Chronic or Frequent Cough Diabetes Eczema Difficulty Breathing Foot Pain Frequent infections Pleurisy or Pneumonia Gout Hair/Nail changes Spitting up Blood Headaches/Migraines Hives Trouble Breathing Joint Injury Itching URI (Cold) Now Memory Loss Jaundice None Muscle Weakness Psoriasis Numbness/Tingling Rash Obesity Skin Disease Osteoporosis None Rheumatic Fever Weight Gain/Loss None Cardiovascular Gastrointestinal Eyes - Ears - Nose - Throat/Mouth Awakening in the night smothering Abdominal Pain Blurring Chest Pain or Angina Appetite Changes Double Vision Congestive Heart Failure Black Stools Eye Disease or Injury Cyanosis (blue skin) Bleeding with Bowel Movements Eye Pain/Discharge Difficulty walking two blocks Blood in Vomit Glasses Edema/Swelling of Hands, Feet or Ankles Chrohn’s Disease/Colitis Glaucoma Heart Attacks Constipation Itchy Eyes Heart Murmur Cramping or pain in the Abdomen Vision changes Heart Trouble Difficulty Swallowing Ear Disease High Blood Pressure Diverticulosis Ear Infections Irregular Heartbeat Frequent Diarrhea Ears ringing Pain in legs Gallbladder Disease Hearing problems Palpitations Gas/Bloating Impaired Hearing Poor Circulation Heartburn or Indigestion Chronic Sinus Trouble Shortness -
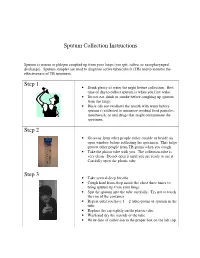
Sputum Collection Instructions Step 1 Step 2 Step 3
Sputum Collection Instructions Sputum is mucus or phlegm coughed up from your lungs (not spit, saliva, or nasopharyngeal discharge). Sputum samples are used to diagnose active tuberculosis (TB) and to monitor the effectiveness of TB treatment. Step 1 • Drink plenty of water the night before collection. Best time of day to collect sputum is when you first wake. • Do not eat, drink or smoke before coughing up sputum from the lungs. • Rinse (do not swallow) the mouth with water before sputum is collected to minimize residual food particles, mouthwash, or oral drugs that might contaminate the specimen. Step 2 • Go away from other people either outside or beside an open window before collecting the specimen. This helps protect other people from TB germs when you cough. • Take the plastic tube with you. The collection tube is very clean. Do not open it until you are ready to use it. Carefully open the plastic tube. Step 3 • Take several deep breaths. • Cough hard from deep inside the chest three times to bring sputum up from your lungs. • Spit the sputum into the tube carefully. Try not to touch the rim of the container. • Repeat until you have 1 – 2 tablespoons of sputum in the tube. • Replace the cap tightly on the plastic tube. • Wash and dry the outside of the tube. • Write date of collection in the proper box on the lab slip. Step 4 • Place the primary specimen container (usually a conical centrifuge tube) in the clear plastic baggie that has the biohazard symbol imprint. • Place the white absorbent sheet in the plastic baggie. -

Perinatal/Neonatal Case Presentation
Perinatal/Neonatal Case Presentation &&&&&&&&&&&&&& Urinary Tract Infection With Trichomonas vaginalis in a Premature Newborn Infant and the Development of Chronic Lung Disease David J. Hoffman, MD vaginal bleeding with suspected abruption resulted in delivery of Gerard D. Brown, DO the infant by Cesarean section. The Apgar scores were 1, 5, and 9 Frederick H. Wirth, MD at 1, 5, and 10 minutes of life, respectively. Betsy S. Gebert, CRNP After delivery, the infant was managed with mechanical Cathy L. Bailey, MS, CRNP ventilation with pressure support and volume guarantee for Endla K. Anday, MD respiratory distress syndrome. She received exogenous surfactant We report a case of a low-birth-weight infant with an infection of the urinary tract with Trichomonas vaginalis, who later developed cystic chronic lung disease suggestive of Wilson-Mikity syndrome. Although she had mild respiratory distress syndrome at birth, the extent of the chronic lung disease was out of proportion to the initial illness. We speculate that maternal infection with this organism may have resulted in an inflammatory response that led to its development. Journal of Perinatology (2003) 23, 59 – 61 doi:10.1038/sj.jp.7210819 CASE PRESENTATION A 956-g, appropriate-for-gestational-age, African–American female was delivered by Cesarean section following 27 5/7 weeks of gestation in breech presentation after a period of advanced cervical dilatation and uterine contractions. Her mother was a 20-year-old gravida 5, para 2022 woman whose prenatal laboratory data were significant for vaginal colonization with Streptococcus agalactiae, treatment for Chlamydia trachomatis, and a history of cocaine and marijuana usage confirmed by urine toxicology. -

Chest Pain in a Patient with Cystic Fibrosis
Copyright ©ERS Journals Ltd 1998 Eur Respir J 1998; 12: 245–247 European Respiratory Journal DOI: 10.1183/09031936.98.12010245 ISSN 0903 - 1936 Printed in UK - all rights reserved CASE FOR DIAGNOSIS Chest pain in a patient with cystic fibrosis D.P. Dunagan*, S.L. Aquino+, M.S. Schechter**, B.K. Rubin**, J.W. Georgitis** Case history A 38 yr old female with a history of cystic fibrosis (CF) presented to an outside emergency department with dysp- noea and right-sided chest pain of approximately 12 h duration. Her history was significant for recurrent pneu- mothoraces and a recent respiratory exacerbation of CF requiring prolonged antibiotic therapy for Pseudomonas aeruginosa. She described the pain as relatively acute in onset, sharp, increased with deep inspiration, without out- ward radiation, and progressive in intensity. There was no history of travel, worsening cough, fever, chills or increase in her chronic expectoration of blood-streaked sputum. An outside chest radiograph was interpreted as demonstrating a "rounded" right lower lobe pneumonia and she was transferred to our institution for further evaluation. Fig. 2. – Computed tomography scan of the chest. Open arrow: multi- On examination, she was thin, afebrile and in minimal ple cysts; closed white arrow: 3.8×5 cm round mass, respiratory distress. There were decreased breath sounds throughout all lung fields, symmetric chest wall excursion with inspiration and bilateral basilar crackles. Subjective right lateral chest discomfort was reported with deep ins- piratory manoeuvres. The remaining physical examination was normal except for clubbing of the upper extremities. Laboratory data revealed an elevated white blood cell count of 19.2×109 cells·L-1 with a normal differential.