Effects of Ready-To-Eat-Cereals on Key Nutritional and Health Outcomes: a Systematic Review
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Pop-Up Grocery Stores Hospital Implementation Guide Concept Overview
Pop-Up Grocery Stores Hospital Implementation Guide Concept Overview Context: • Many hospitals are limiting or closing their communal cafeteria offerings as protocol to face coronavirus • Doctors, nurses and other hospital staff may find their supermarkets are out of basic necessities when they are able to shop for their families after their hospital shifts • Hospitals still have access to a wide range of items from their foodservice distributors Solution: • Hospitals can convert their unused cafeteria space into temporary, pop-up grocery stores for staff • Stock the shelves with the products you already buy and make simple adjustments to tailor the offering to a grocery setting • See our General Mills category management recommendation in the following slides to bring this concept to life in your hospital, using the products you have on hand to serve the caregivers throughout your hospital Category Management Best Practices • Prioritize “Everyday Essentials” • Milk, Eggs, Cheese, Produce, Paper Products, Meat, Cereal, Bread/Baked Goods Category Reach (Based on Household Penetration & Purchase Frequency) • Consider “Family Entertainment” Options: Targeted Essentials Occasional Essentials Everyday Essentials Diapers Butter/Margarine Milk RTE Cereal • Microwave popcorn, baking mixes, frosting/icing Wine/Beer Coffee Eggs Bread Baby Food Flour Cheese Sugar/Sweeteners Paper Products Laundry Supplies Fresh Produce HH Cleaners Fresh Meat • As shelf/cooler space allows, bring in additional individually saleable foodservice Targeted Staples Occasional -

The Brands They Love for Cacfp
the brands they love for cacfp More than 70 eligible products for the Child and Adult Care Food Program all with no artificial flavors, no colors from artificial sources, and no high fructose corn syrup! UPC PRODUCT DESCRIPTION UPC PRODUCT DESCRIPTION ON-THE-GO POUCH CEREAL GOLD MEDALTM MIX 100-16000-31529-4 Whole Grain Variety Mun Mix 100-16000-14401-6 25% Less Sugar Cinnamon Toast Crunch™ Cereal On-The-Go Pouch NEW! 100-16000-31527-0 Whole Grain Complete Pancake Mix BOWLPAK CEREAL YOPLAIT PORTABLE YOGURT 100-16000-32262-9 Cheerios™ 100-70470-49295-4 Simply Go-Gurt Strawberry 2 oz 100-16000-38387-3 Cinnamon Chex™ 100-70470-14914-8 Go Big™ Blueberry 4 oz NEW! 100-16000-29444-5 25% Less Sugar Cinnamon Toast Crunch™ 100-70470-47402-8 Go Big™ Strawberry 4 oz 100-16000-33213-0 Corn Chex™ YOPLAIT YOGURT 4OZ 100-16000-11942-7 Kix™ 000-70470-17725-0 Trix™ Raspberry Rainbow 100-16000-32263-6 Multi Grain Cheerios™ 000-70470-17726-7 Trix™ Strawberry Banana Bash 100-16000-31921-6 Rice Chex™ 100-70470-31077-7 Trix™ Triple Cherry CUP CEREAL 000-70470-17729-8 Yoplait Original Strawberry/Strawberry Banana 25% Less Sugar Cinnamon Toast Crunch™ 000-70470-17728-1 Yoplait Original Red Raspberry/Harvest Peach 100-16000-14886-1 2oz Eq. Grain Cereal NEW! YOPLAIT ORIGINAL YOGURT 6OZ 100-16000-14883-0 Cinnamon Chex™ 2oz Eq. Grain Cereal NEW! 100-70470-00302-0 Original Mountain Blueberry BULK CEREAL 100-70470-00303-7 Original Cherry Orchard 100-16000-11977-9 Cheerios™ 100-70470-00323-5 Original French Vanilla 100-16000-13326-3 Corn Chex™ 100-70470-00306-8 Original -

Participating Products ™
powered by For My School PARTICIPATING PRODUCTS ™ ANNIE’S® Minions Cereal Vanilla Vibe REFRIGERATED & DAIRY Nature Valley™ Oatmeal Baking Mix Nature Valley™ Baked Oat LAND O’LAKES® Butter Squares Cereal Bites Oui® by Yoplait® (4-6oz) Nature Valley™ Biscuits Cheesy Rice Nature Valley™ Granola Pillsbury™ Crescents Nature Valley™ Granola Cups Cookies Crunch Pillsbury™ Grands Protein One™ Bars Crackers Nature Valley™ Oat Clusters Pillsbury™ Cookies Nature Valley™ Snack Mix Fruit Snacks Nature Valley™ Protein Pillsbury™ Pizza and Nature Valley™ Wafers Granola Bars Crunchy Granola Pie Crust Nature Valley™ Packed Bars Graham Snacks Nature Valley™ Protein Yoplait® Go-GURT® and Pillsbury™ Soft Baked Bars Soft Baked ® Mac & Cheese Simply Go-GURT Yogurt Nature Valley™ Toasted ® Pasta Quinoa Rice Yoplait Go-gurt Dunkers WHOLESOME PANTRY Oats Muesli ® Pizza Bagels Yoplait Light & Original Wholesome Pantry Organic Oatmeal Crisp™ Pizza Poppers Fridge Packs (8ct) Peanut Butter Peanut Butter Chocolate ® Popcorn Yoplait Kids Yogurt Wholesome Pantry Organic Blasted Shreds™ Multipack Refrigerated Baked Goods Frozen Fruit Raisin Nut Bran Yoplait® Trix™ Yogurt Wholesome Pantry Organic Rice Pasta Chowder ® Reese’s Puffs Multipack Maple Syrup Rice Shell Pasta Rice Chex™ Yoplait® (4-6oz) Wholesome Pantry Almond Snack Mix Strawberry Toast Crunch™ Yoplait® Smoothie Milk Soup Total™ YQ® by Yoplait® Yogurt Trix™ Wheaties™ SHOPRITE BRAND BAKING ShopRite Frozen Appetizers Betty Crocker™ Baking Mixes FROZEN ShopRite Flexible Straws Betty Crocker™ Frosting Green Giant™ -

Fiscal 2018 Annual Report
FISCAL 2018 ANNUAL REPORT Fiscal 2018 Financial Highlights Change In millions, except per share and 52 weeks ended 52 weeks ended on a constant- profit margin data May 27, 2018 May 28, 2017 Change currency basis* Net Sales $ 15,740 $ 15,620 1% Organic Net Sales* Flat Operating Profit $ 2,509 $ 2,566 (2%) Total Segment Operating Profit* $ 2,792 $ 2,953 (5%) (6%) Operating Profit Margin 15.9% 16.4% -50 basis points Adjusted Operating Profit Margin* 17.2% 18.1% -90 basis points Net Earnings Attributable to General Mills $ 2,131 $ 1,658 29% Diluted Earnings per Share (EPS) $ 3.64 $ 2.77 31% Adjusted Diluted EPS, Excluding Certain $ 3.11 $ 3.08 1% Flat Items Affecting Comparability* Average Diluted Shares Outstanding 586 598 (2%) Dividends per Share $ 1.96 $ 1.92 2% Net Sales Total Segment Adjusted Diluted Free Cash Flow* Dollars in millions Operating Profit* Earnings per Share* Dollars in millions Dollars in millions Dollars $3.11 $3,154 $17,910 $2,218 $17,630 $3,035 $3,000 $3.08 $2,953 $16,563 $2,035 $2,792 $1,959 $15,740 $15,620 $1,936 $1,731 $2.92 $2.86 $2.82 2014 2015 2016 2017 2018 2014 2015 2016 2017 2018 2014 2015 2016 2017 2018 2014 2015 2016 2017 2018 *See page 45 of form 10-K herein for discussion of non-GAAP measures. Fiscal 2018 Net Sales $15.7 Billion Total Company Net Sales by Product Platform Total Company Net Sales by Reporting Segment Our portfolio is focused on five global growth In fiscal 2018, we reported net sales in four platforms. -
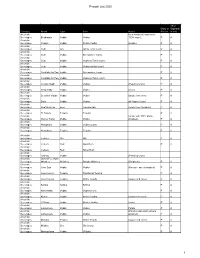
Pesach List 2020 1
Pesach List 2020 All or Dairy or Sephardi Category Brand Type Item Notes Pareve m only Alcoholic from Australia (made from Beverages Bushman's Vodka Vodka 100% cane). P A Alcoholic Beverages Chopin Vodka Potato Vodka (potato). P A Alcoholic Beverages Club Gin Gin & Tonic (corn). P A Alcoholic Beverages Club Vodka Screwdriver (corn). P A Alcoholic Beverages Club Vodka Vodka & Tonic (corn). P A Alcoholic Beverages Club Vodka Vodka Gimlet (corn). P A Alcoholic Beverages Cocktails for Two Vodka Screwdriver (corn). P A Alcoholic Beverages Cocktails for Two Vodka Vodka & Tonic (corn). P A Alcoholic Beverages Crystal Head Vodka Vodka (Peach & Corn) P A Alcoholic Beverages Deep Eddy Vodka Vodka (corn) P A Alcoholic Beverages Devotion Vodka Vodka Vodka (made from corn) P A Alcoholic Beverages Dixie Vodka Vodka all 4 types (corn) P A Alcoholic Beverages Dogfish Head Beer Tweason'ale (made from Sorghum) P A Alcoholic Beverages El Tosoro. Tequila Tequila P A Alcoholic (made with 100% Idaho Beverages Glacier Teton Vodka Vodka potatoes). P A Alcoholic Beverages Hampton's Vodka Vodka (Corn) P A Alcoholic Beverages Herradura. Tequila Tequila P A Alcoholic Beverages Iceberg Gin Gin P A Alcoholic Beverages Iceberg Rum Gold Rum P A Alcoholic Beverages Iceberg Rum Silver Rum Alcoholic Beverages Iceberg Vodka (Peach & Corn) Alcoholic James F.C. Hyde Beverages Whiskey Whiskey Sorgho Whiskey (Sorghum) P A Alcoholic Beverages Jinro Soju Vodka Vodka (Korean - sweet potatoes) P A Alcoholic Beverages Jose Cuervo Tequila Traditional Tequila P A Alcoholic Beverages Jose Cuervo Tequila White Tequila (agave and cane). P A Alcoholic Beverages Kahlua Kahlua Kahlua P A Alcoholic Beverages Kamchatka Vodka Vodka (corn). -
Wic Approved Food Guide
MASSACHUSETTS WIC APPROVED FOOD GUIDE GOOD FOOD and A WHOLE LOT MORE! June 2021 Shopping with your WIC Card • Buy what you need. You do not have to buy all your foods at one time! • Have your card ready at check out. • Before scanning any of your foods, tell the cashier you are using a WIC Card. • When the cashier tells you, slide your WIC Card in the Point of Sale (POS) machine or hand your WIC Card to the cashier. • Enter your PIN and press the enter button on the keypad. • The cashier will scan your foods. • The amount of approved food items and dollar amount of fruits and vegetables you purchase will be deducted from your WIC account. • The cashier will give you a receipt which shows your remaining benefit balance and the date benefits expire. Save this receipt for future reference. • It’s important to swipe your WIC Card before any other forms of payment. Any remaining balance can be paid with either cash, EBT, SNAP, or other form of payment accepted by the store. Table of Contents Fruits and Vegetables 1-2 Whole Grains 3-7 Whole Wheat Pasta Bread Tortillas Brown Rice Oatmeal Dairy 8-12 Milk Cheese Tofu Yogurt Eggs Soymilk Peanut Butter and Beans 13-14 Peanut Butter Dried Beans, Lentils, and Peas Canned Beans Cereal 15-20 Hot Cereal Cold Cereal Juice 21-24 Bottled Juice - Shelf Stable Frozen Juice Infant Foods 25-27 Infant Fruits and Vegetables Infant Cereal Infant Formula For Fully Breastfeeding Moms and Babies Only (Infant Meats, Canned Fish) 1 Fruits and Vegetables Fruits and Vegetables Fresh WIC-Approved • Any size • Organic allowed • Whole, cut, bagged or packaged Do not buy • Added sugars, fats and oils • Salad kits or party trays • Salad bar items with added food items (dip, dressing, nuts, etc.) • Dried fruits or vegetables • Fruit baskets • Herbs or spices Any size Any brand • Any fruit or vegetable Shopping tip The availability of fresh produce varies by season. -
GENERAL MILLS, INC. (Exact Name of Registrant As Specified in Its Charter)
UNITED STATES SECURITIES AND EXCHANGE COMMISSION Washington, D.C. 20549 FORM 10-K ⌧ ANNUAL REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 FOR THE FISCAL YEAR ENDED May 30, 2010 TRANSITION REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 FOR THE TRANSITION PERIOD FROM TO Commission file number: 001-01185 GENERAL MILLS, INC. (Exact name of registrant as specified in its charter) Delaware 41-0274440 (State or other jurisdiction of (I.R.S. Employer incorporation or organization) Identification No.) Number One General Mills Boulevard 55426 Minneapolis, Minnesota (Zip Code) (Address of principal executive offices) (763) 764-7600 (Registrant’s telephone number, including area code) Securities registered pursuant to Section 12(b) of the Act: Name of each exchange Title of each class on which registered Common Stock, $.10 par value New York Stock Exchange Securities registered pursuant to Section 12(g) of the Act: None Indicate by check mark if the registrant is a well-known seasoned issuer, as defined in Rule 405 of the Securities Act. Yes ⌧ No Indicate by check mark if the registrant is not required to file reports pursuant to Section 13 or Section 15(d) of the Act. Yes No ⌧ Indicate by check mark whether the registrant (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the preceding 12 months (or for such shorter period that the registrant was required to file such reports), and (2) has been subject to such filing requirements for the past 90 days. -

Palm Oil Shopping Guide: Current Best Choices
FOOD Brand Names of FOOD Brand Names of FOOD Brand Names of FOOD Brand Names of FOOD Brand Names of Make a Difference RSPO Members RSPO Members RSPO Members RSPO Members RSPO Members for Wild 3 Musketeers Cinnamon Toast Crunch Honey Maid Grahams Mothers Cookies Splenda Orangutans Act II Coffee Mate Hot Pockets Mountain High Yogurt Starburst Adam's PB Country Crock Hungry Jack Muffin Mam Pastries Stouffers Almond Joy Country Time Hunt's Muir Glen Trident Gum BOYCOTTING PALM Altoids Crisco International Delight Nabisco Sun Chips OIL IS NOT THE Arnott's Biscuits Crunch and Munch Jenny Craig Meals Nature Valley SuperMoist Cake Mixes SOLUTION… Aunt Jemima Foods Dean's Dips Jeno's Pizza Near East Sweet Rewards Bars Austin Brand Crackers Doritos Jif PB Nerds Sweet Tarts Supporting Baby Ruth Dove Chocolates Jiffy Pop Nesquik Swiss Miss companies that are Bac Os Dreyer's Jolly Ranchers Nestle Products Tombstone Pizza members of the Baker's Chocolate Edy's Justin's NutButter Nutter Butter Cookies Tostitos RSPO (Roundtable on Balance Bars Egg Beaters Justin's PB Cups Old El Paso Total Cereal Sustainable Palm Oil) Banquet Meals Endangered Species Choc. Keebler Cookies Oreo Cookies Totino's Pizza is the most Barilla Famous Amos Cookies Keebler Crackers Orville Redenbacher's Trix Cereal responsible solution. BelVita Fiber One Products Kellogg's Products Pam Tuna Helper Ben & Jerry's Ice Cream Fleischmann's Kid Cuisine Parent's Choice Twix Bertolli Frito Lay Kit Kat Parkay Twizzlers For more information Betty Crocker products Folgers Kix Cereal Pasta -

CHAPTER 5 Competitor Analysis and Intelligence
M05_HOLL6830_02_SE_C05.QXD 16/1/10 1:24 pm Page 155 CHAPTER 5 Competitor analysis and intelligence LEARNING OBJECTIVES After studying this chapter you should be able to: integrate competition into an environmental analysis discuss competition and competitors at different levels: — budget competition — core benefit competition — product class competition — brand competition specify the levels in competitor awareness describe how to design a competitor intelligence (CI) system evaluate the information sources for CI specify the contents of a competitor audit evaluate the strengths and weaknesses of competitors assess current strategies of main competitors give examples of how to evaluate the strengths and weaknesses of competitors assess current strategies of main competitors outline possible response patterns of main competitors M05_HOLL6830_02_SE_C05.QXD 16/1/10 1:24 pm Page 156 156 PART II ASSESSING THE EXTERNAL MARKETING SITUATION 5.1 INTRODUCTION Competitive Most often competitive intelligence is used to mean the action of gathering analysing and intelligence distributing information about products, customers, competitors and any aspect of the envir- Gathering, analysing and onment needed to support executives and managers in making strategic marketing decisions distributing information about products, cus- for an organisation. Competitor intelligence (CI) is a more narrow term, as it only focuses tomers, competitors and on the competitor aspect. any aspect of the envi- Except for a minor section dealing with interaction between competitors (section 5.3) this ronment needed to sup- port executives and chapter is mainly about how to analyse competitors, their behaviour and their strategies. A managers in making more comprehensive analysis of competitor relationships is given in Chapter 6 (section 6.6). -

WV WIC Program Approved Food List Effective October 1, 2018 Revised 12/3/18 Page 1 of 16 BRAND SPECIFIC WIC ITEMS UPC APPENDIX
WV WIC Program Approved Food List Effective October 1, 2018 BRAND SPECIFIC WIC ITEMS UPC APPENDIX ➢ BREAKFAST CEREAL Prod_Name UPC_PLU Best Choice Best Choice Maple Brown Sugar Shredded Wheat 15.5oz 070038606925 Best Choice Strawberry Frosted Shredded Wheat 15.5 oz 070038622383 Best Yet Best Yet Strawberry Frosted Shredded Wheat 15.5 oz 042187428734 Essential Essential Everyday Strwbrry Frosted Shred Wheat 18 oz 041303046357 Everyday Essential Everyday Strwbrry Frosted Shred Wht 16.3 oz 041303001653 Food Club Food Club Frosted Shredded Wheat Strwbry Crm 18 oz 036800292086 Food Lion Food Lion Strawberry Frosted Shredded Wheat 18 oz 035826099136 General Mills General Mills Cheerios 016000666108 General Mills Cheerios 016000666603 General Mills Cheerios 12 oz 016000487727 General Mills Cheerios 14 oz 016000275645 General Mills Cheerios 18 oz 016000275287 General Mills Cheerios 36 oz 016000176829 General Mills Cheerios 18 oz 2 pk (36 oz) 016000264243 General Mills Cheerios 20 oz 016000125414 General Mills Cheerios 21 oz 016000476080 General Mills Cheerios 28 oz 016000160125 General Mills Cheerios Multi Grain 016000275621 General Mills Cheerios Multi Grain 016000687905 General Mills Cheerios Value Pack 21.6 oz 016000433274 General Mills Multi Grain Cheerios 16.2 oz 016000423442 General Mills MultiGrain Cheerios 12 oz 016000487697 General Mills MultiGrain Cheerios 18 oz 016000487710 General Mills Multigrain Cheerios 18.75 oz 016000401051 General Mills MultiGrain Cheerios 25.6 oz 016000160118 General Mills MultiGrain Cheerios 36 oz 016000442894 -
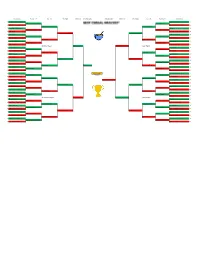
Cereal Bracket
Round of 64 Round of 32 Sweet 16 Elite Eight Final Four Championship Championship Final Four Elite Eight Sweet 16 Round of 32 Round of 64 1 Cinnamon Toast Crunch 51 Frosted Flakes 49 1 Cinnamon Toast Crunch 30 Frosted Flakes 40 16 Blueberry Cheerios 2 Dippin Dots Cereal 4 16 Cinnamon Toast Crunch 24 Frosted Flakes 24 8 Frosted Mini Wheats 42 Kix 34 8 Frosted Mini Wheats 16 Kix 6 9 Alpha-Bits 2 Chocolate Peanut Butter Cheerios 6 9 Cinnamon Toast Crunch 19 Frosted Flakes 33 5 Cheerios 47 Golden Grahams 47 5 Cheerios 23 Golden Grahams 24 12 Bran Flakes 6 Franken Berry 6 12 Cheerios 12 Golden Grahams 12 4 Cocoa Pebbles 35 Fruity Pebbles 39 4 Cocoa Pebbles 22 Fruity Pebbles 22 13 Honey Smacks 18 Kashi Go Lean 14 13 Cinnamon Region Froot Loops 31 Frosted Flakes 28 Sugar Region 6 Count Chocula 30 Corn Pops 41 6 Count Chocula 24 Corn Pops 18 11 Special K Red Berries 23 PB Chex 12 11 Count Chocula 3 Apple Jacks 21 3 Waffle Crisp 42 Apple Jacks 42 3 Waffle Crisp 21 Apple Jacks 27 14 Nilla Cereal 11 Krave 10 14 Froot Loops 27 Apple Jacks 13 7 Raisin Bran 37 Rice Crispy Treats 33 7 Raisin Bran 18 Rice Krispy Treats 26 10 Chocolate Chex 15 Captain Peanut Butter Crunch 20 10 Froot Loops 33 Froot Loops 24 Rice Krispy Treats 15 2 Froot Loops 50 Honey Comb 46 2 Froot Loops 28 Honey Combs 19 15 Twinkies Cereal 3 Donettes Cereal 7 15 1 Lucky Charms 49 Froot Loops Honey Nut Cheerios 48 1 Lucky Charms 37 Champion Honey Nut Cheerios 35 16 Sour Patch Kids Cereal 4 Grape-Nuts 5 16 Lucky Charms 34 Honey Nut Cheerios 23 8 Special K 25 Honey Nut Cheerios 22 Rice -

Providers Choice Approved Cereal List the Cereals Listed Below Meet the Child and Adult Care Food Program (CACFP) Meal Pattern Requirements
Providers Choice Approved Cereal List The cereals listed below meet the Child and Adult Care Food Program (CACFP) meal pattern requirements. Cereals must contain no more than 6 grams of sugar per dry ounce. Please contact Providers Choice with questions. Whole Grain-Rich General Mills General Mills General Mills General Mills General Mills General Mills General Mills General Mills General Mills General Mills Cheerios Cheerios Cheerios Chex Chex Chex Chex Chex Chex Kix Original Multi-Grain Ancient Grains Blueberry Cinnamon Corn Rice Vanilla Wheat Original General Mills General Mills General Mills General Mills General Mills General Mills Kellogg’s Kellogg’s Kellogg’s Kellogg’s Kix Kix Fiber One Fiber One Total Wheaties Frosted Mini Wheats Frosted Mini Wheats Frosted Mini Wheats Frosted Mini Wheats Honey Berry Berry Original Honey Clusters Whole Grain Original Original Blueberry Maple Brown Sugar Strawberry Kellogg’s Kellogg’s Kellogg’s Kellogg’s Kellogg’s Kellogg’s Kellogg’s Millville (Aldi) Millville (Aldi) Millville (Aldi) Frosted Mini Wheats Frosted Mini Wheats Frosted Mini Wheats All-Bran Special K Special K Special K Crispy Oats Crispy Oats Frosted Shredded Little Bites Little Bites Cinnamon Roll Original Protein Apple Raspberry Coconut Cranberry Original Multigrain Wheat Original Chocolate Original Almond Almond Original Post Post Post Post Post Post Post Post Post Quaker Bran Flakes Grape-Nuts Grape- Nuts Great Grains Great Grains Great Grains Honey Bunches of Honey Bunches of Honey Bunches of Life Original Original Flakes Banana