Comments on Michigan Senate Bill
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

New Member Pictorial Directory
NEW MEMBER PICTORIAL DIRECTORY PREPARED BY THE COMMITTEE ON HOUSE ADMINISTRATION Candice S. Miller, Chairman | Robert A. Brady, Ranking Minority Member NEW MEMBER PICTORIAL DIRECTORY As of November 7, 2014, the Clerk of the House had not received certificates of election for any of the individuals listed in this directory. At the time this publication was sent to press, the following races had not been finally determined: Arizona 2nd California 7th California 9th California 16th California 17th California 26th California 52nd Louisiana 5th Louisiana 6th New York 25th Washington 4th Profiles of candidates from these districts begin on page 33. PREpaRED BY THE COMMITTEE ON HOUSE ADMINISTRATION Candice S. Miller, Chairman | Robert A. Brady, Ranking Minority Member TABLE OF CONTENTS Adams, Alma .........................23 Katko, John...........................21 Abraham, Ralph .......................36 Khanna, Ro...........................35 Aguilar, Pete ...........................4 Knight, Steve ..........................4 Allen, Rick ............................9 Lawrence, Brenda......................15 Amador, Tony.........................34 Lieu, Ted..............................5 Ashford, Brad .........................17 Loudermilk, Barry ......................9 Assini, Mark ..........................38 Love, Mia ............................26 Babin, Brian ..........................26 MacArthur, Tom.......................19 Beyer, Don ........................... 27 Mayo, Jamie ..........................37 Bishop, Mike .........................14 -

Prayer Practices
Floor Action 5-145 Prayer Practices Legislatures operate with a certain element of pomp, ceremony and procedure that flavor the institution with a unique air of tradition and theatre. The mystique of the opening ceremonies and rituals help to bring order and dignity to the proceedings. One of these opening ceremonies is the offering of a prayer. Use of legislative prayer. The practice of opening legislative sessions with prayer is long- standing. The custom draws its roots from both houses of the British Parliament, which, according to noted parliamentarian Luther Cushing, from time ”immemorial” began each day with a “reading of the prayers.” In the United States, this custom has continued without interruption at the federal level since the first Congress under the Constitution (1789) and for more than a century in many states. Almost all state legislatures still use an opening prayer as part of their tradition and procedure (see table 02-5.50). In the Massachusetts Senate, a prayer is offered at the beginning of floor sessions for special occasions. Although the use of an opening prayer is standard practice, the timing of when the prayer occurs varies (see table 02-5.51). In the majority of legislative bodies, the prayer is offered after the floor session is called to order, but before the opening roll call is taken. Prayers sometimes are given before floor sessions are officially called to order; this is true in the Colorado House, Nebraska Senate and Ohio House. Many chambers vary on who delivers the prayer. Forty-seven chambers allow people other than the designated legislative chaplain or a visiting chaplain to offer the opening prayer (see table 02-5.52). -

Washtenaw County: Contact Your Legislators Guide 2021-2022
Washtenaw County: Contact Your Legislators Guide 2021-2022 Members of Congress, the Michigan Legislature, and County Boards of Commissioners are elected to represent their constituents. Michigan Citizens must play an important role in the lawmaking process by informing their elected officials of their opinions on issues. There are several ways to communicate with your elected officials: By Visit Legislators are eager to meet their constituents and will try to accommodate your request for a personal meeting. Please make an appointment in advance, and understand if the legislator is called away for an unscheduled committee meeting or session. You may meet with a staff member who will be welcoming and attentive to your concerns. Legislators also meet with their constituents at coffee hours or towns hall meetings in their districts. **During the COVID-19 pandemic face to face meetings may be limited. Virtual meetings may take the place of in-person meetings. By Phone A phone call is a quick and easy way to contact your legislator. Direct phone numbers are provided in the pages that follow. You may also contact the state Capitol switchboard and they will direct your call. Senators: (517) 373-2400 Representatives: (517) 373-0135 By Letter Include your full name and address when sending mail to your legislator so staff can confirm you are a constituent and provide a response. For MI State Legislators address letters as indicated below: The Honorable (Full Name) The Honorable (Full Name) State Senator State Representative State Capitol State Capitol P.O. Box 30036 P.O. Box 30014 Lansing, MI 48909-7536 Lansing, MI 48909-7514 By Email Email addresses are provided on the pages that follow. -

Michigan MISSION STATEMENT
IDF Virtual State Advocacy Workshop Michigan MISSION STATEMENT The Immune Deficiency Foundation improves the diagnosis, treatment, and quality of life of people affected by primary immunodeficiency through fostering a community empowered by advocacy, education, and research. Influencing Policy in Your State Michigan State Legislature . Bicameral body consisting of two houses: Senate and House of Representatives . 110 members serve in the Michigan House of Representatives . 38 members serve in the Michigan Senate . Michigan Legislature is full-time . The Legislature convenes for two-year terms and this term is split into two annual sessions. The Legislature must convene each session by the second Wednesday in January. 2021 session began on January 13, 2021, and is scheduled to adjourn on December 31, 2021 . The 101st Legislature ends December 31, 2022 The Legislative Process in Michigan Bill referred to a Committee Considers Bill – General Orders or Bill Introduced & Standing Committee May Entail Public Hearings Second Reading in Title Reading for Review on the Bill Chamber of Origin Resolution of Three Reading Process is Third Reading and Bill Referred to Other Differences, If Repeated in Other Vote in Chamber of Chamber Necessary Chamber Origin Bill Goes to Governor Bill Becomes a Law Governor Gretchen Whitmer (D) . The governor is the head of the executive branch in Michigan. All bills passed by the Michigan State Legislature go to the governor, who can sign the bill into law, allow it to become law without their signature, or veto it. Speaker of the House Jason Wentworth (R) . The Speaker is the highest ranking officer of the House of Representatives, and is elected by the House Members. -

Motion to Intervene by Michigan Senate
Case 2:17-cv-14148-ELC-DPH-GJQECFNo.208filed01/24/19PageID.7771Page1of DYKEMA GOSSETTA PROFESSIONAL LIMITED LIABILITY COMPANYCAPITOL VIEW, 201 TOWNSEND STREET, SUITE 900LANSING, MICHIGAN 48933 Secretary of State, Secretary as Michigan Capacity in official her BENSON, JOCELYN v. TLAIB, H. RASHIDA and RIVERA LORENZO LONG, W. RICHARD “DICK” LASALLE, G. JON “JACK” L.KETOLA, DIANA L. ROSA HOLLIDAY, GRASHA, J. “BILL” WILLIAM FARRIS, E. DONNA ELLIS, E. JACK JR., DURHAL, C. FREDERICK J.BRDAK, ROGER MICHIGAN, OF VOTERS OF WOMEN LEAGUE Defendant. Defendant. Plaintiffs, EASTERN DISTRICT OF MICHIGAN MICHIGAN OF DISTRICT EASTERN UNITED STATES DISTRICT COURT COURT DISTRICT STATES UNITED SOUTHERN DIVISION DIVISION SOUTHERN 32 1 MOTION TO INTERVENE INTERVENE TO MOTION SENATE’S THE MICHIGAN J.Quist Hon.Gordon Hood Page Hon.Denise Clay Hon.EricL. 2:17-cv-14148 CaseNo. Case 2:17-cv-14148-ELC-DPH-GJQECFNo.208filed01/24/19PageID.7772Page2of DYKEMA GOSSETTA PROFESSIONAL LIMITED LIABILITY COMPANYCAPITOL VIEW, 201 TOWNSEND STREET, SUITE 900LANSING, MICHIGAN 48933 Motion and allow it to intervene as Defendant in this matter. matter. this in Defendant as intervene to it allow Motionand relief sought. of this Motion to Plaintiffs and but requested, were their denied, concurrence in the this Motion was filed. Prior to filing this Motion, the Senate explained the nature Defendants’ concurrence but did not obtain Defendants’ concurrence by the time 1. Exhibit as attached whichis Declaratory and Injunctive Relief pursuant to Fed. R. Civ. P. 24(c), a copy Support. The -

How Partisan Gerrymandering Limits Voting Rights by Alex Tausanovitch and Danielle Root July 8, 2020
How Partisan Gerrymandering Limits Voting Rights By Alex Tausanovitch and Danielle Root July 8, 2020 Every 10 years, each U.S. state redraws its electoral districts—lines on a map that have serious real-world consequences. If districts are drawn fairly, then the public can elect representatives who reflect the views of the population as a whole. But if the district lines are manipulated through partisan gerrymandering, then the legislature will be untethered from the popular will. The Center for American Progress has published a series of reports that analyze how partisan gerrymandering affects issues from gun violence prevention to access to health insurance to policies that are important to children and families.1 This issue brief explores how gerrymandering affects voting rights. In recent years, gerrymandered legislatures have pioneered other tools to stay in power, including making it harder for voters who oppose them to cast a ballot. It is a power grab on top of a power grab. Fortunately, both of these interrelated problems—gerrymandering and limits on the right to vote—are fixable. Indeed, citizens across the country seem to be fired up about reform.2 This could be the political moment to solve these problems and get American democracy back on track. This issue brief examines the only four states where, after the 2018 elections, the party that won a majority of state legislative seats received only a minority of the total statewide vote: North Carolina, Michigan, Pennsylvania, and Wisconsin. Because of gerrymandering, these four states dramatically failed a basic test of democracy—votes did not translate into political power. -

115Th Congress 135
MICHIGAN 115th Congress 135 MICHIGAN (Population 2010, 9,883,640) SENATORS DEBBIE STABENOW, Democrat, of Lansing, MI; born in Gladwin, MI, April 29, 1950; education: Clare High School; B.A., Michigan State University, 1972; M.SW., Michigan State University, 1975; public service: Ingham County, MI, Commissioner, 1975–78, chairperson for two years; Michigan State House of Representatives, 1979–90; Michigan State Senate, 1991– 94; religion: Methodist; children: Todd and Michelle; committees: ranking member, Agriculture, Nutrition, and Forestry; Budget; Energy and Natural Resources; Finance; Joint Committee on Taxation; elected to the U.S. House of Representatives in 1996 and 1998; elected to the U.S. Senate on November 7, 2000; reelected to each succeeding Senate term. Office Listings http://stabenow.senate.gov twitter: @SenStabenow 731 Hart Senate Office Building, Washington, DC 20510 ....................................................... (202) 224–4822 Chief of Staff.—Matt VanKuiken. FAX: 228–0325 Legislative Director.—Emily Carwell. Scheduler.—Anne Stanski. 221 West Lake Lansing Road, Suite 100, East Lansing, MI 48823 ......................................... (517) 203–1760 719 Griswold Street, Suite 700, Detroit, MI 48226 .................................................................. (313) 961–4330 432 North Saginaw, Suite 301, Flint, MI 48502 ....................................................................... (810) 720–4172 3335 South Airport Road West, Suite 6B, Traverse City, MI 49684 ...................................... -
MISD Directory
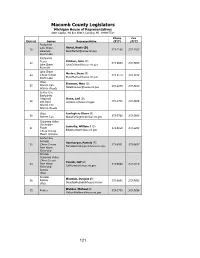
Macomb County Legislators Michigan House of Representatives State Capitol, PO Box 30014, Lansing, MI 48909-7514 Phone Fax District Serves Representative (517) (517) Eastpointe Lake Shore Hertel, Kevin (D) 18 373-1180 373-1103 Lakeview [email protected] South Lake Eastpointe Fraser Chirkun, John (D) 22 373-0854 373-5934 Lake Shore [email protected] Roseville Lake Shore Marino, Steve (R) 24 L’Anse Creuse 373-0113 373-5912 South Lake [email protected] Utica Shannon, Nate (D) 25 Warren Con. 373-2275 373-5910 Warren Woods [email protected] Center Line Eastpointe Fitzgerald Stone, Lori (D) 28 Van Dyke [email protected] 373-1772 373-5906 Warren Con. Warren Woods Utica Farrington, Diana (R) 30 Warren Con. [email protected] 373-7768 373-5903 Chippewa Valley Clintondale Sowerby, William J (D) 31 Fraser 373-0159 373-5893 L’Anse Creuse [email protected] Mount Clemens Anchor Bay Armada Hornberger, Pamela (R) 32 L’Anse Creuse 373-8931 373-8637 [email protected] New Haven Richmond Armada Chippewa Valley L’Anse Creuse Yaroch, Jeff (R) 33 New Haven 373-0820 373-5974 Richmond [email protected] Romeo Utica Armada Wozniak, Douglas (R) 36 Romeo 373-0843 373-5892 Utica [email protected] Webber, Michael (R) 45 Romeo 373-1773 373-5838 [email protected] 121 Macomb County Legislators Michigan Senate State Capitol, PO Box 30036, Lansing, MI 48909-7536 Phone Fax District Serves Senator (517) (517) Center Line Eastpointe Fitzgerald Fraser Wojno, Paul (D) 9 Lake Shore SenPWojno@ 373-8360 373-9230 South Lake senate.michigan.gov Van Dyke Warren Con. -

Members Senate
RICHARD J. ATTEN DONALD E. BISHOP 3oth D¡strid 8th D¡strici MEMBERS OF THE SENATE BASil. W. EROWN 3rd o¡srr;d tSlh D¡¡lr¡cl GARY BYKER ARIHUR cART\,vRlGHl 23rd Distrid 5lh Districi DANIEL S. COOPER GARY G. CORBIN ROBERT W. DAVIS AIVIN J. DeGROW t5th D¡slr¡cl 25lh D¡sir¡d 37lh Þ¡str¡d 28lh Distr¡cl HARRY A. De¡'tASO JAIIES DeSANA 20lh D¡slrid I lth Disrr¡d MEMBERS OF THE SE NATË ANTHONY A. DÊREZINSKI WITLIÀU FAUST 33rd Dirtrid t3rh Disrr¡d JAC K FAXON WII,I.IA'A B. FITZGERAI-D 7th D¡.lrid lst D¡stri€l R. ROBERI GEAKE THOMAS GUASTELLO JEROME T. HARI JOHN CHARLES HÊRTEI. l41h D¡3r.id 9th Disrricr 34rh D¡str¡d 2nd D¡str¡cl DAVID S. HOLMES, JR. BILI. S. HUFFMAN ,lth D¡.rricr lóth D¡slr¡cl MEMBERS OF THE SENATE KERRY KAA.IA.IER JOSEPH S. MACK t 7lh D¡slr¡.t 38th D¡slricr PATRICK H. McCOttOUGH ART MILTER, JR. lOrh Dirrr¡ct 27rh D¡shid EARL E, NEISON ¡AICHAEI. J. O'BRIEN JOHN R. OÍTERBACHER DAVID A. PIAWECKI 24lh D¡slr¡cl ólh Di6lri.t 32nd D¡str¡cl ì2lh District HAROI-D JOSEPH SCOTT JOSEPH TA. SNYDER 29th D¡.rrid 2&h D¡str¡d MEMBERS OF THE SENATE JOHN E. TOEPP ROBERT VANDER LAAN 3óth D¡.rrid 3l.t Dislr¡d a. JOHN A. WELBORN ROEERT D. YOUNG 2lrt D¡¡rrid 35lh D¡5lr¡cl a BIttIE S. FARNUM HAt- W, ZtEG[En CHARLES O. -

State Notes TOPICS of LEGISLATIVE INTEREST Spring 2020
State Notes TOPICS OF LEGISLATIVE INTEREST Spring 2020 An Overview of the 2020 Census and What It Means for Michigan By Stephen Jackson, Legislative Analyst Introduction Every 10 years, the United States Census Bureau conducts a census to count the number of people living in the US and to collect basic demographic, such as age, sex, race, and ethnicity, and housing information. The decennial census is mandated by Article I, Section 2 of the US Constitution, which provides that: "The actual Enumeration shall be made within three Years after the first Meeting of the Congress of the United States, and within every subsequent Term of ten Years, in such manner as they shall by Law direct". The decennial census provides a snapshot of the United States that determines how seats in the US House of Representatives are apportioned, how states redraw congressional and legislative districts, how Federal funding is distributed, and how businesses make decisions. This article provides a brief history of the decennial census and a general overview of how the census works, and also explores the implications the 2020 Census will have on Michigan over the next decade and some of the challenges facing the 2020 Census. Brief History of the Decennial Census The first census was conducted in 1790 under the direction of then-Secretary of State Thomas Jefferson.1 The decennial census was conducted under the authority of the Secretary of State until the Department of Interior assumed responsibility for it in 1849. Beginning in 1850, Congress established a temporary census office before each census to direct operations and organization. -

For the 101St Michigan Legislature
FOR THE 101ST MICHIGAN LEGISLATURE DECEMBER 2020 About MSU’s Legislative Leadership Program MSU’s Legislative Leadership Program invites new members of Michigan’s House of Representatives and Michigan Senate to engage in interactive sessions with content experts, including university faculty and practitioners, in the brief time between election and their first legislative sessions. At its 1994 inception, LLP was designed to create a forum and the resources to help newly elected legislators meet the challenges of serving in a state with term limits. The program was meant to help legislators forge links to university policy resources. Since that time, LLP has evolved into a broadened opportunity to gain insights into concepts that affect statewide constituencies, into evidence-based information on emerging issues and into the art and science of governing in divided times, such as under state House co-speakerships. At the same time, IPPSR has evolved as a hub for policy expertise, information and outreach, a center for survey research training and excellence, and an opportunity for training for those who seek leadership through elected office or public service. The program is built upon a series of specially designed events, including presenters, researchers and facilitated discussions. Sessions are focused on topics of compelling interest, from the state’s revenue stream, to its expenditures, K-12 education, demographics and innovations. IPPSR is proud that LLP has hosted a majority of newly elected legislators from each party and draws support from the Legislature’s highest officers. The program continues to build on MSU's long-standing tradition of providing leadership training to state and county officials, community leaders, and aspiring public officials. -

Lame Duck Study
League of Women Voters of Michigan Lame Duck Study A Look at the Procedures and Issues in Legislative Lame Duck Sessions Lame Duck Study Group 11-14-2020 Glenn Anderson – NW Wayne County Carla Barrows-Wiggins- Oakland Area Priscilla Burnham – Marquette County Jerry Demaire – Macomb County Joan Hunault – Leelanau County Marian Kromkowski- Leelanau County Beth Moore- Lansing Area Jim Treharne – Oakland Area Paula Bowman- LWVMI VP, Program Christina Schlitt – LWVMI President League of Women Voters of Michigan Lame Duck Study Table of Contents LAME DUCK STUDY ...................................................................................................... 3 IMPETUS FOR THE LAME DUCK STUDY ................................................................. 3 THE SCOPE THE LAME DUCK STUDY INCLUDES .................................................. 3 AN OVERVIEW OF THE LEGISLATIVE PROCESS MAY BE FOUND AT ................. 3 OVERVIEW OF A LAME DUCK SESSION ..................................................................... 5 Introduction .................................................................................................................. 5 Observations ................................................................................................................ 5 Summary of Findings ................................................................................................... 5 Data ............................................................................................................................. 6 Summary.....................................................................................................................