Pilot Study of a Self-Directed Web-Based Mindfulness
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Concept of Self-Liberation in Theravada Burmese Buddhism
ASIA-PACIFIC NAZARENE THEOLOGICAL SEMINARY THE CONCEPT OF SELF-LIBERATION IN THERAVADA BURMESE BUDDHISM A Thesis Presented to The Faculty of Asia-Pacific Nazarene Theological Seminary In Partial Fulfilment of the Degree Master of Science in Theology BY CING SIAN THAWN TAYTAY, RIZAL NOVEMBER 2020 ASIA-PACIFIC NAZARENE THEOLOGICAL SEMINARY WE HEREBY APPROVE THE THESIS SUBMITTED BY Cing Sian Thawn ENTITLED THE CONCEPT OF SELF-LIBERATION IN THERAVADA BURMESE BUDDHISTS AS PARTIAL FULFILLMENT OF THE REQUIREMENTS FOR THE DEGREE MASTER OF SCIENCE IN THEOLOGY (SYSTEMATIC THEOLOGY) Dr. Dick Eugenio _________ Dr. Phillip Davis __________ Thesis Adviser Date Program Director Date Dr. Eileen Ruger _________ Dr. Naw Yaw Yet ___________ Internal Reader Date External Reader Date Dr. Dick Eugenio _________ Dr. Larry Bollinger ___________ Academic Dean Date President Date ii ABSTRACT This thesis explores the self-liberation concept of Theravada Buddhism, with the hope that it can provide a foundation towards a dialogical exchange between Buddhists and Christians in Myanmar. To provide a better understanding of the context, the thesis offers a brief historical background of Buddhist-Christian relations in Myanmar. By mainly relying on the translation of the Pali Tipitaka, along with a number of secondary sources from prominent Buddhist scholars, the self-liberation concept of Theravada Buddhism is discussed, beginning with the personal experience of Gotama, the Buddha. The thesis is descriptive in nature. The research employs a basic qualitative method, integrated with the analytical and interpretive methods. Correlation and synthesis were done and are presented in the final chapter with an emphasis on implications for interfaith dialogue. The study produced some significant findings. -

Effect of Mindfull Breathing on Stressed Students Rohit Chobe*& Dr.L.N.Joshi**
International Journal of Yoga and Allied Sciences (ISSN: 2278 – 5159) Volume: 5, Issue: 2; July- Dec 2016 Effect of Mindfull Breathing on Stressed Students Rohit Chobe*& Dr.L.N.Joshi** *Research scholar, Dept. of yogic sciences, Uttarakhand Sanskrit University, Haridwar, Uttarakhand. **Assistant professor, Dept. of yogic sciences, Uttarakhand Sanskrit University, Haridwar, Uttarakhand. Abstract: Background: Stress is a major issue for college students as they cope with a variety of academic, social, and personal challenges.1 Stress is one of the main reasons for the development of various pathological conditions. These include psychological disorders such as depression and anxiety 33. Mindfulness is an open and non-judgmental attitude nourished by genuine interest and care for the situation given, rather than dwelling on rigid ideas and concepts about what should be and how it should be. It is the faculty of knowing what is happening in this particular moment and of feeling it as well, a precisely and softly as possible.34 When we start talking about mental well being, it is our prime duties to assess the efficacy of breathe meditation (Mindfulness on Breathing) on stress. Objective: -The aim of this study was to assess the effect of Breath meditation (Mindfulnss on breathing) on stress of college going students. Methods and procedures:- For this 40 female subjects were drawn from Dev sanskriti vishvavidyalaya, Gayatrikunj, Haridwar by using method of purposive sampling. Meditation was conducted for 25 days about 45 minute every day in evening. Pre-post data of Breath meditation is collected by using stress scale (Prepared by Dr M. Singh). -

Bridging Worlds: Buddhist Women's Voices Across Generations
BRIDGING WORLDS Buddhist Women’s Voices Across Generations EDITED BY Karma Lekshe Tsomo First Edition: Yuan Chuan Press 2004 Second Edition: Sakyadhita 2018 Copyright © 2018 Karma Lekshe Tsomo All rights reserved No part of this book may not be reproduced or utilized in any form or by any means, electronic or mechanical, or by any information storage or retreival system, without the prior written permission from the publisher, except in the case of brief quotations. Cover Illustration, "Woman on Bridge" © 1982 Shig Hiu Wan. All rights reserved. "Buddha" calligraphy ©1978 Il Ta Sunim. All rights reserved. Chapter Illustrations © 2012 Dr. Helen H. Hu. All rights reserved. Book design and layout by Lillian Barnes Bridging Worlds Buddhist Women’s Voices Across Generations EDITED BY Karma Lekshe Tsomo 7th Sakyadhita International Conference on Buddhist Women With a Message from His Holiness the XIVth Dalai Lama SAKYADHITA | HONOLULU, HAWAI‘I iv | Bridging Worlds Contents | v CONTENTS MESSAGE His Holiness the XIVth Dalai Lama xi ACKNOWLEDGMENTS xiii INTRODUCTION 1 Karma Lekshe Tsomo UNDERSTANDING BUDDHIST WOMEN AROUND THE WORLD Thus Have I Heard: The Emerging Female Voice in Buddhism Tenzin Palmo 21 Sakyadhita: Empowering the Daughters of the Buddha Thea Mohr 27 Buddhist Women of Bhutan Tenzin Dadon (Sonam Wangmo) 43 Buddhist Laywomen of Nepal Nivedita Kumari Mishra 45 Himalayan Buddhist Nuns Pacha Lobzang Chhodon 59 Great Women Practitioners of Buddhadharma: Inspiration in Modern Times Sherab Sangmo 63 Buddhist Nuns of Vietnam Thich Nu Dien Van Hue 67 A Survey of the Bhikkhunī Saṅgha in Vietnam Thich Nu Dong Anh (Nguyen Thi Kim Loan) 71 Nuns of the Mendicant Tradition in Vietnam Thich Nu Tri Lien (Nguyen Thi Tuyet) 77 vi | Bridging Worlds UNDERSTANDING BUDDHIST WOMEN OF TAIWAN Buddhist Women in Taiwan Chuandao Shih 85 A Perspective on Buddhist Women in Taiwan Yikong Shi 91 The Inspiration ofVen. -

Curriculum 28 Day/ 200 Hour Yoga & Meditation
Curriculum 28 day/ 200 hour Yoga & Meditation & Teacher- Training Leh/ Ladakh 2015 Hatha 24- Days Topic/ Dharana/ Mantras Sanskrit/ Pranayama & Mudra/ Jnana - Yoga Anatomy Methodology (Sunday off) theme Asana Dhyana/ / Japa Hindi Kriya Bandha Meditation 1 day Arrivalday/ Open Ceremony Arrivalday/ Open Ceremony pre-pranayama Yama:Ahimsa, Satya, Asteya, sitting pose: sukhasana, OM- AUM, exercise: Dhamma, Dukha, Brahmacharya, Aparigraha; Stütz & Observing, listen, voice, siddasana, padmasana, Namskara Gayatri sanskrit Yama & Yogabreathing (full Sila, Samadhi, Niyama: Sauca, Santosa, Bewegung I. language, sitting in, role 3 days dandasana, vajrasana; mudra, Jnana/ Tapas, Svadyaya, Mantra, Om alphabeth, yoga, abdome- Panja, breathing- skeleton of the teacher, Niyama pawanmuktasana (anti mudra Isvarapranidhana, Vedas, mani padme jappa, chanting breathing), neti, meditation system demonstration asanas rheumatic, anti gastric) Upanishads, Vedanta, hum brahma mudra Samkya Surya namaskara ( Sun Mahakumbhakas: Bhagavatgita, Hatha- Preparing a Yoga class salutation); Standing pose: Mahamudra, Brahmari, sitali, sitkari, Yoga, Bhakti- Yoga, SHANTI Likhita jappa; (classroom organisation, tatasana, trikoasana, aswini mudra, mindfulness, Kapalhabathi, surya Karma - Yoga, Jnana- MANTRA – numbers and time managment, Prana & vrikasana, chin mudra, walking II. muscles 4 days bheda, bhastrika, Yoga, Kundalini- Yoga, OM SAHANA hindu/ Hindi/ sequencing virabhadrasana; invert chinmaya meditation, and tissues Apana murcha, plavini; Chakra, nadis, Ida, VAVATU, So- -

Download Article
Advances in Social Science, Education and Humanities Research (ASSEHR), volume 340 2019 International Conference on Education Innovation and Economic Management (ICEIEM 2019) Buddhism Exchanges in Trans-Himalaya Region: Development and Recommendations Yi Zhang Institute of Taoism and Religious Culture Sichuan University Chengdu, China Abstract—This paper attempts to explain the historical II. DEVELOPMENT OF BUDDHISM EXCHANGES IN TRANS- development of exchange of Buddhism between China and the HIMALAYA REGION Trans-Himalayan countries, as well as its positive effects on the bilateral relations between them, and give some useful A. Han Dynasty (202BD-220AD) recommendations. It argued that Buddhism has become a The initial stage of Buddhist communication between powerful cultural tie that binds the nations in the region and promotes friendship between the Himalayan states. It also China and the countries of the trans-Himalaya region was suggested that China should make further efforts to excavate started during the Han Dynasty. It is widely believed that Buddhist relics and sort out Buddhist spiritual resources on the Buddhism was introduced into China during the reign of silk road, promote the communication between Mahayana Emperor Ming of the Eastern Han Dynasty. The eminent Buddhism and Theravada continuously on the basis of seeking monk Zhu Shemoteng and the Zhu Falan arrived in Luoyang, common ground while reserving differences, encourage and translated Buddhist scriptures and carried forward Buddha support educational cooperation between China and Buddhist dharma. Since then, the number of monks who came to China universities and colleges in trans-Himalaya countries through gradually increased. She Moteng translated a volume of the expanding the friendly exchanges between youth students and Sutra of Forty-two Chapters. -
Insight Newsletter
INSIGHT NEWSLETTER FALL WINTER A Dharma Life: 2 0 1 0 / 2 0 1 1 The Extraordinary is Always Arising A Profile of Ruth Denison IMS Schedules: The Retreat Center 2011 Dharma elder Ruth Denison, who celebrates her 88th birthday this year, has led The Forest Refuge 2011 courses at IMS since it opened in 1976. She is one of three Westerners who received permission to teach from Burmese master Sayagi U Ba Khin, and she was the first Teacher Profile Buddhist teacher in the US to lead an all-women’s Buddhist meditation retreat. IMS News & Developments Beloved by many for her unique teaching style, she reflects here on how she came to the Buddha’s teachings and developed her own way of communicating them to her BCBS Schedule: 2011 Listing students, so that they too can taste the extraordinary in their lives. y connection to the dharma atmosphere available to us than the ordinary Mstarted early in childhood. I was way of being. I once read a woman’s born in East Prussia, where my father had description of how things looked to her a large flower nursery. To help the people after she became a nun and went to live in who came to work in the fields I would walk a monastery. It was powerful – it shifted along a row giving water to the flowers. my awareness from the ordinary way of When I looked back and saw that the water life, the ordinary way of seeing things, to was unevenly distributed, I would think, the extraordinary that is always just right “This one will be very sad” – I animated there, if you allow yourself to stop. -
Experience of Samadhi
THE EXPERIENCE OF SAM API 11 An In-depth Exploration of Buddhist Meditation ■ Richard Shan km an ■ Includes interviews with Jack Kornfield, Sharon Salzberg, Christina Feldman, and other teachers The Experience of Samadhi THE EXPERIENCE OF SAMADHI An In-depth Exploration of Buddhist Meditation Richard Shankman SHAMBHALA Boston & London 2 0 0 8 Shambhala Publications, Inc. Horticultural Hall 300 Massachusetts Avenue Boston, Massachusetts 02115 •^^w.shambhala.com © 2008 by Richard Shankman Pages 219-20 constitute a continuation of the copyright page. A l rights reserved. No part of this book may be reproduced in any form or by any means, electronic or mechanical, including photocopying, recording, orby any information storage and retrieval system, without permission in writing from the publisher. 987654321 First Edition Printed in Canada @ This edition is printed on acid-free paper that meets the American National Standards Institute Z39.48 Standard. O This book was printed on 100% postconsumer recycled paper. For more information please visit us at •^^w.shambhala.com. Distributed in the United States by Random House, Inc., and in Canada by Random. House of Canada Ltd Interior design and composition: Greta D. Sibley & Associates Library of Congress Cataloging-in-Publication- Data Shankman, Richard. The experience of samadhi: an in-depth exploration of Buddhist meditation / Richard Shankman.—1st ed. p. cm. ■ Includes bibliographical references and index. ISBN 978-1-59030-521-8 (pbk.: alk. paper) 1. Samadhi. 2. Buddhist literature, Pali—History and criticism. 3. Buddhists—Interviews. 1. Title. BQ5630.S16S43 2008 294^3 '4435 DC22 2008017613 CONTENTS Preface | ix Acknowledgments | xii Introduction | xiii PART ONE SAMADHI IN THE PALI TEXTS I. -
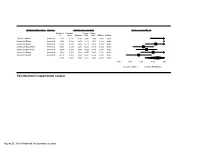
Pain Threshold in Laboratory Studies Pain Threshold in Experimental
Subgroup within study Outcome Statistics for each study Hedges's g and 95% CI Hedges's Standard Lower Upper g error Variance limit limit Z-Value p-Value Tashani 2017Blank threshold 1.241 0.433 0.187 0.392 2.089 2.865 0.004 Forsyth 2014Blank threshold 3.012 0.458 0.210 2.114 3.910 6.577 0.000 Reiner 2016Blank threshold 0.631 0.233 0.054 0.175 1.088 2.712 0.007 Sharpe 2013high threat threshold 0.091 0.233 0.054 -0.366 0.549 0.392 0.695 Sharpe 2013low threat threshold 0.230 0.234 0.055 -0.229 0.689 0.983 0.326 Shires 2018Blank threshold 0.515 0.274 0.075 -0.023 1.053 1.877 0.060 Wang 2019 Blank threshold -0.110 0.281 0.079 -0.661 0.442 -0.390 0.697 0.719 0.287 0.082 0.157 1.282 2.506 0.012 -1.00 -0.50 0.00 0.50 1.00 Fav ours Control Fav ours Mindfulness Pain threshold in experimental samples Figure S1: Pain threshold in laboratory studies Subgroup within study Outcome Statistics for each study Hedges's g and 95% CI Hedges's Standard Lower Upper g error Variance limit limit Z-Value p-Value Tashani 2017Blank tolerance 0.548 0.402 0.162 -0.240 1.336 1.364 0.173 Esch 2017 Blank tolerance 0.311 0.352 0.124 -0.379 1.002 0.884 0.377 Forsyth 2014 Blank tolerance 3.698 0.517 0.267 2.685 4.711 7.153 0.000 Kingston 2007Blank tolerance 0.317 0.305 0.093 -0.280 0.914 1.040 0.299 Liu 2013 Blank tolerance 0.700 0.320 0.102 0.074 1.327 2.191 0.028 Sharpe 2013 high theat tolerance 0.254 0.234 0.055 -0.205 0.714 1.087 0.277 Sharpe 2013 low threat tolerance -0.205 0.234 0.055 -0.663 0.254 -0.876 0.381 Shires 2018 Blank tolerance 1.261 0.294 0.086 0.685 1.836 -

Is a Female Buddha Possible in Non-Esoteric Buddhism?
Gender and the Soteriology Debate in Buddhism: Is a Female Buddha Possible in Non-Esoteric Buddhism? Karma Sonam Palmo Shastri (Bachelor of Arts), Acharya (Masters in Philosophy) Central University of Tibetan Studies Submitted in fulfilment of the requirements for the degree of Doctor of Philosophy University of Tasmania November 2013 Declaration of Originality This thesis contains no material which has been accepted for a degree or diploma by the University or any other institution, except by way of background information and duly acknowledged in the thesis, and to the best of my knowledge and belief no material previously published or written by another person except where due acknowledgement is made in the text of the thesis, nor does the thesis contain any material that infringes copyright. Karma Sonam Palmo Dated Authority of Access This thesis may be made available for loan and limited copying and communication in accordance with the Copyright Act 1968. Karma Sonam Palmo Dated Acknowledgments First of all, I would like to thank the Tasmania Buddhist Studies Exchange Program between the University of Tasmania and the Central University of Tibetan Studies for generously granting me the Buddhist Studies Graduate Research Scholarship. Next, I thank my supervisors Dr. Lucy Tatman and Dr. Sonam Thakchoe for their advice, support, guidance and supervision throughout the completion of this thesis over the last four years. I owe special thanks to Lucy and Belinda for going through my final draft and suggesting grammatical corrections. I am also thankful to Ruth Gamble of Australia National University and James Stewart of University of Tasmania for generously sharing their resources during my early period of research. -

Philosophy East/West: Exploring Intersections Between
Document généré le 1 oct. 2021 10:38 Philosophical Inquiry in Education Philosophy East/West: Exploring Intersections Between Educational and Contemplative Practices (Ergas and Todd) and Reconstructing "Education" through Mindful Attention: Positioning the Mind at the Center of Curriculum and Pedagogy (Oren Ergas) Deborah Orr Volume 25, numéro 2, 2018 URI : https://id.erudit.org/iderudit/1070746ar DOI : https://doi.org/10.7202/1070746ar Aller au sommaire du numéro Éditeur(s) Canadian Philosophy of Education Society ISSN 2369-8659 (numérique) Découvrir la revue Citer ce document Orr, D. (2018). Philosophy East/West: Exploring Intersections Between Educational and Contemplative Practices (Ergas and Todd) and Reconstructing "Education" through Mindful Attention: Positioning the Mind at the Center of Curriculum and Pedagogy (Oren Ergas). Philosophical Inquiry in Education, 25(2), 232–245. https://doi.org/10.7202/1070746ar Copyright ©, 2018 Deborah Orr Ce document est protégé par la loi sur le droit d’auteur. L’utilisation des services d’Érudit (y compris la reproduction) est assujettie à sa politique d’utilisation que vous pouvez consulter en ligne. https://apropos.erudit.org/fr/usagers/politique-dutilisation/ Cet article est diffusé et préservé par Érudit. Érudit est un consortium interuniversitaire sans but lucratif composé de l’Université de Montréal, l’Université Laval et l’Université du Québec à Montréal. Il a pour mission la promotion et la valorisation de la recherche. https://www.erudit.org/fr/ Philosophical Inquiry in Education, Volume 25 (2018), No. 2, pp. 232–245 Review of Philosophy East/West: Exploring Intersections Between Educational and Contemplative Practices by Oren Ergas and Sharon Todd (Eds.). -

Anapanasati Sutta Student Notes April 2011
Anapanasati Sutta – Student Notes – 1 Anapanasati Sutta Student Notes: Session One 1. “Anapana” means “in-breath and out-breath” “Sati” means “mindfulness” or present moment awareness that simply notices what is happening without in any way interfering, without adding or subtracting anything to or from the experience. It’s bare awareness. So, anapanasati means “mindfulness while breathing in and out”. 2. Background to the sutta: It’s the end of the rainy-season retreat, and the Buddha is so pleased with the meditation practice of those gathered with him, that he announces he is going to stay on another month, the month of the white water-lily or white lotus moon. At the end of that month he gives this teaching on anapanasati, giving the teaching under the full moon at night. The Buddha says: “Mindfulness of in-and-out breathing, when developed and pursued, is of great benefit. Mindfulness of in-and-out breathing, when developed and pursued, brings the four foundations of mindfulness to perfection. The four foundations of mindfulness, when developed and pursued, bring the seven factors of awakening to their culmination. The seven factors of awakening, when developed and pursued, perfect clear insight and liberation.” In other words, anapanasati can lead to enlightenment. Four foundations of mindfulness (satipatthana) are: • Kaya (Body) • Vedana (Feelings or experiencing sensations as pleasant, unpleasant or neutral) • Citta (Mind or mental formations, thoughts and emotions) • Dhammas (mental objects, or perspectives on experience used to investigate reality) These four categories correspond to the four sets of contemplations in the anapanasati method. Seven factors of awakening are a spiral path of conditionality, leading towards enlightenment: 1. -
A MANUAL for BUDDHISM and DEEP ECOLOGY: SPECIAL EDITION by the WORLD BUDDHIST UNIVERSITY (With Permission of Author.) B.E
AA ManualManual forfor BuddhismBuddhism andand DeepDeep EcologyEcology Daniel H. Henning, Ph.D. HAN DD ET U 'S B B O RY eOK LIBRA E-mail: [email protected] Web site: www.buddhanet.net Buddha Dharma Education Association Inc. A MANUAL for BUDDHISM © 2002 Daniel H. Henning. All rights reserved. No part of this book may be reproduced, stored in a retrieval system, AND DEEP Or transmitted by any means, electronic, mechanical, photocopying, Recording, or otherwise, without written permission from the author. ECOLOGY ISBN: 1-4033-7006-0 Library of Congress Control Number: 2002095421 A MANUAL for BUDDHISM AND DEEP ECOLOGY: SPECIAL EDITION BY THE WORLD BUDDHIST UNIVERSITY (With permission of author.) B.E. 2549 (2006) Daniel H. Henning, Ph.D. “To the spiritual protection of trees and forests worldwide ” 1 CONTENTS Preface PREFACE BY THE WORLD BUDDHIST 2 by the World Buddhist University UNIVERSITY Practicing Buddhism is sometimes described as like walking though a ACKNOWLEDGMENTS 4 forest on a misty day. Eventually you “get wet” and come to a deeper understanding of the teachings. The same might be said about INTRODUCTION 5 environmentalism. Eventually, hopefully, it moves from manipulating or even saving the environment and becomes the CHAPTER ONE 9 environment. “Getting wet” in this sense is incorporating a spiritual perspective in working with and in the environment. This is called BUDDHISM AND VALUES Deep Ecology. ................................ CHAPTER TWO 21 Buddhism and Deep Ecology belong in the same title because at their DHAMMA, DEEP ECOLOGY, core they are both talking about how to be at home in the universe. AND ENVIRONMENT The original meaning of ecology goes back to the Greeks who saw the ......................................