Identification of Neoepitopes Recognized by Tumor-Infiltrating Lymphocytes (Tils) from Patients with Glioma
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Seq2pathway Vignette
seq2pathway Vignette Bin Wang, Xinan Holly Yang, Arjun Kinstlick May 19, 2021 Contents 1 Abstract 1 2 Package Installation 2 3 runseq2pathway 2 4 Two main functions 3 4.1 seq2gene . .3 4.1.1 seq2gene flowchart . .3 4.1.2 runseq2gene inputs/parameters . .5 4.1.3 runseq2gene outputs . .8 4.2 gene2pathway . 10 4.2.1 gene2pathway flowchart . 11 4.2.2 gene2pathway test inputs/parameters . 11 4.2.3 gene2pathway test outputs . 12 5 Examples 13 5.1 ChIP-seq data analysis . 13 5.1.1 Map ChIP-seq enriched peaks to genes using runseq2gene .................... 13 5.1.2 Discover enriched GO terms using gene2pathway_test with gene scores . 15 5.1.3 Discover enriched GO terms using Fisher's Exact test without gene scores . 17 5.1.4 Add description for genes . 20 5.2 RNA-seq data analysis . 20 6 R environment session 23 1 Abstract Seq2pathway is a novel computational tool to analyze functional gene-sets (including signaling pathways) using variable next-generation sequencing data[1]. Integral to this tool are the \seq2gene" and \gene2pathway" components in series that infer a quantitative pathway-level profile for each sample. The seq2gene function assigns phenotype-associated significance of genomic regions to gene-level scores, where the significance could be p-values of SNPs or point mutations, protein-binding affinity, or transcriptional expression level. The seq2gene function has the feasibility to assign non-exon regions to a range of neighboring genes besides the nearest one, thus facilitating the study of functional non-coding elements[2]. Then the gene2pathway summarizes gene-level measurements to pathway-level scores, comparing the quantity of significance for gene members within a pathway with those outside a pathway. -

Gene Expression Profiling of Corpus Luteum Reveals the Importance Of
bioRxiv preprint doi: https://doi.org/10.1101/673558; this version posted February 27, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY-NC-ND 4.0 International license. 1 Gene expression profiling of corpus luteum reveals the 2 importance of immune system during early pregnancy in 3 domestic sheep. 4 Kisun Pokharel1, Jaana Peippo2 Melak Weldenegodguad1, Mervi Honkatukia2, Meng-Hua Li3*, Juha 5 Kantanen1* 6 1 Natural Resources Institute Finland (Luke), Jokioinen, Finland 7 2 Nordgen – The Nordic Genetic Resources Center, Ås, Norway 8 3 College of Animal Science and Technology, China Agriculture University, Beijing, China 9 * Correspondence: MHL, [email protected]; JK, [email protected] 10 Abstract: The majority of pregnancy loss in ruminants occurs during the preimplantation stage, which is thus 11 the most critical period determining reproductive success. While ovulation rate is the major determinant of 12 litter size in sheep, interactions among the conceptus, corpus luteum and endometrium are essential for 13 pregnancy success. Here, we performed a comparative transcriptome study by sequencing total mRNA from 14 corpus luteum (CL) collected during the preimplantation stage of pregnancy in Finnsheep, Texel and F1 15 crosses, and mapping the RNA-Seq reads to the latest Rambouillet reference genome. A total of 21,287 genes 16 were expressed in our dataset. Highly expressed autosomal genes in the CL were associated with biological 17 processes such as progesterone formation (STAR, CYP11A1, and HSD3B1) and embryo implantation (eg. -

DF6079-TBRG4 Antibody
Affinity Biosciences website:www.affbiotech.com order:[email protected] TBRG4 Antibody Cat.#: DF6079 Concn.: 1mg/ml Mol.Wt.: 71kDa Size: 100ul,200ul Source: Rabbit Clonality: Polyclonal Application: WB 1:500-1:2000, IHC 1:50-1:200, IF/ICC 1:100-1:500, ELISA(peptide) 1:20000-1:40000 *The optimal dilutions should be determined by the end user. Reactivity: Human,Mouse,Rat Purification: The antiserum was purified by peptide affinity chromatography using SulfoLink™ Coupling Resin (Thermo Fisher Scientific). Specificity: TBRG4 Antibody detects endogenous levels of total TBRG4. Immunogen: A synthesized peptide derived from human TBRG4, corresponding to a region within C-terminal amino acids. Uniprot: Q969Z0 Description: TBRG4 (transforming growth factor beta regulator 4), also known as CPR2 (cell cycle progression restoration protein 2) or FASTKD4 (FAST kinase domain-containing protein 4), is a 631 amino acid protein that contains one RAP domain and belongs to the FAST kinase family. TBRG4 is ubiquitously expressed and may have a role in cell cycle progression. Existing as two alternatively spliced isoforms, the gene encoding TBRG4 maps to human chromosome 7p13. Chromosome 7 is approximately 158 million bases long, encodes over 1000 genes and makes up about 5% of the human genome. Chromosome 7 has been linked to Osteogenesis imperfecta, Pendred syndrome, Lissencephaly, Citrullinemia and Shwachman-Diamond syndrome. The deletion of a portion of the q arm of chromosome 7 is associated with Williams-Beuren syndrome, a condition characterized by mild mental retardation, an unusual comfort and friendliness with strangers and an elfin appearance. Deletions of portions of the q arm of chromosome 7 are also seen in a number of myeloid disorders including cases of acute myelogenous leukemia and myelodysplasia. -

Noelia Díaz Blanco
Effects of environmental factors on the gonadal transcriptome of European sea bass (Dicentrarchus labrax), juvenile growth and sex ratios Noelia Díaz Blanco Ph.D. thesis 2014 Submitted in partial fulfillment of the requirements for the Ph.D. degree from the Universitat Pompeu Fabra (UPF). This work has been carried out at the Group of Biology of Reproduction (GBR), at the Department of Renewable Marine Resources of the Institute of Marine Sciences (ICM-CSIC). Thesis supervisor: Dr. Francesc Piferrer Professor d’Investigació Institut de Ciències del Mar (ICM-CSIC) i ii A mis padres A Xavi iii iv Acknowledgements This thesis has been made possible by the support of many people who in one way or another, many times unknowingly, gave me the strength to overcome this "long and winding road". First of all, I would like to thank my supervisor, Dr. Francesc Piferrer, for his patience, guidance and wise advice throughout all this Ph.D. experience. But above all, for the trust he placed on me almost seven years ago when he offered me the opportunity to be part of his team. Thanks also for teaching me how to question always everything, for sharing with me your enthusiasm for science and for giving me the opportunity of learning from you by participating in many projects, collaborations and scientific meetings. I am also thankful to my colleagues (former and present Group of Biology of Reproduction members) for your support and encouragement throughout this journey. To the “exGBRs”, thanks for helping me with my first steps into this world. Working as an undergrad with you Dr. -

Global Mapping of Herpesvirus-‐Host Protein Complexes Reveals a Novel Transcription
Global mapping of herpesvirus-host protein complexes reveals a novel transcription strategy for late genes By Zoe Hartman Davis A dissertation submitted in partial satisfaction of the Requirements for the degree of Doctor of Philosophy in Infectious Disease and Immunity in the Graduate Division of the University of California, Berkeley Committee in charge: Professor Britt A. Glaunsinger, Chair Professor Laurent Coscoy Professor Qiang Zhou Spring 2015 Abstract Global mapping of herpesvirus-host protein complexes reveals a novel transcription strategy for late genes By Zoe Hartman Davis Doctor of Philosophy in Infectious Diseases and Immunity University of California, Berkeley Professor Britt A. Glaunsinger, Chair Mapping host-pathogen interactions has proven instrumental for understanding how viruses manipulate host machinery and how numerous cellular processes are regulated. DNA viruses such as herpesviruses have relatively large coding capacity and thus can target an extensive network of cellular proteins. To identify the host proteins hijacked by this pathogen, we systematically affinity tagged and purified all 89 proteins of Kaposi’s sarcoma-associated herpesvirus (KSHV) from human cells. Mass spectrometry of this material identified over 500 high-confidence virus-host interactions. KSHV causes AIDS-associated cancers and its interaction network is enriched for proteins linked to cancer and overlaps with proteins that are also targeted by HIV-1. This work revealed many new interactions between viral and host proteins. I have focused on one interaction in particular, that of a previously uncharacterized KSHV protein, ORF24, with cellular RNA polymerase II (RNAP II). All DNA viruses encode a class of genes that are expressed only late in the infectious cycle, following replication of the viral genome. -

Universidade Nova De Lisboa Instituto De Higiene E Medicina Tropical
Universidade Nova de Lisboa Instituto de Higiene e Medicina Tropical Regulation of the apoptosis pathway in Rhipicephalus annulatus ticks by the protozoan Babesia bigemina Catarina Sofia Bento Monteiro DISSERTAÇÃO PARA A OBTENÇÃO DO GRAU DE MESTRE EM PARASITOLOGIA MÉDICA JANEIRO, 2018 Universidade Nova de Lisboa Instituto de Higiene e Medicina Tropical Regulation of the apoptosis pathway in Rhipicephalus annulatus ticks by the protozoan Babesia bigemina Autor: Catarina Sofia Bento Monteiro Orientador: Doutora Ana Isabel Amaro Gonçalves Domingos (IHMT, UNL) Coorientador: Doutora Sandra Isabel da Conceição Antunes (IHMT, UNL) Dissertação apresentada para cumprimento dos requisitos necessários à obtenção do grau de mestre em parasitologia médica The results obtained during the development of this master project were reported at two international conferences: Monteiro, C, Domingos, A, and Antunes, S 2017, ´Regulation of the apoptosis pathway in Rhipicephalus annulatus ticks by the protozoan Babesia bigemina´, COST action: EuroNegVec, 11-13 September, Crete, Greece. Monteiro, C, Domingos, A, and Antunes, S 2017 ´Is the apoptosis pathway in Rhipicephalus annulatus ticks regulated by the protozoan Babesia bigemina?´ Conference: Biotecnología Habana 2017: ´La Biotecnología Agropecuaria en el siglo XXI´, 3-6 December, Varadero, Cuba. i Acknowledgments Quero, desde já, agradecer à Doutora Ana Domingos por se ter disponibilizado a orientar-me e por não ter desistido de mim. À Doutora Sandra Antunes, pelo apoio constante e compreensão durante toda esta longa jornada. Admiro a simplicidade com que encaras a vida. À Joana Couto pela boa disposição e prontidão em ajudar. És das pessoas mais genuínas que já conheci. À Joana Ferrolho com quem partilho o mesmo gosto pela medicina veterinária. -

Master Biomedizin 2018 1) UCSC & Uniprot 2) Homology 3) MSA 4) Phylogeny
Master Biomedizin 2018 1) UCSC & UniProt 2) Homology 3) MSA 4) Phylogeny Pablo Mier 1 [email protected] Genomics *Images from: Wikipedia 1 a. Get the fasta sequence of the human (Homo sapiens) protein P53 from UniProt (https://www.uniprot.org/). Which one of all the isoforms should you download? P04637 b. Find the P53 protein from mouse (Mus musculus). As you see, there is more than one entry for mouse. Which UniProt entry should you select? P02340 c. BLAT the human P53 using “hg38” as database (in UCSC, http://genome.ucsc.edu/cgi-bin/hgBlat), and answer: How many amino acids has the query sequence? 393 aa And how many nucleotides? 1179 nt Is it a perfect alignment? No Which is the genomic locus of the target? Chr17 7669612-7676594 d. Visualize and navigate through the P53 genome region, and answer: Which genes are around? ATP1B2 and WRAP53 How many exons does it have? 9 exons e. BLAT the mouse P53 against the human genome “hg38”. What do you observe? The result is worse (85%) Human Mouse (Homo sapiens) (Mus musculus) Pablo Mier 2 [email protected] Genomics *Images from: UniProt 1 a. P04637 (P53_HUMAN). The canonical. b. P02340 (P53_MOUSE). Pablo Mier 3 [email protected] Genomics *Images from: UCSC 1 c. 393 amino acids Not a perfect alignment chr17 393*3 = 1179 nucleotides (“lpennvl”) 7669612-7676594 d. ATP1B2 and WRAP53. 9 exons (9 blocks). 9 8 7 6 5 4 3 2 1 e. The result is worse (85%). Pablo Mier 4 [email protected] UniProt database 2 a. -

Supplementary Materials
Supplementary materials Supplementary Table S1: MGNC compound library Ingredien Molecule Caco- Mol ID MW AlogP OB (%) BBB DL FASA- HL t Name Name 2 shengdi MOL012254 campesterol 400.8 7.63 37.58 1.34 0.98 0.7 0.21 20.2 shengdi MOL000519 coniferin 314.4 3.16 31.11 0.42 -0.2 0.3 0.27 74.6 beta- shengdi MOL000359 414.8 8.08 36.91 1.32 0.99 0.8 0.23 20.2 sitosterol pachymic shengdi MOL000289 528.9 6.54 33.63 0.1 -0.6 0.8 0 9.27 acid Poricoic acid shengdi MOL000291 484.7 5.64 30.52 -0.08 -0.9 0.8 0 8.67 B Chrysanthem shengdi MOL004492 585 8.24 38.72 0.51 -1 0.6 0.3 17.5 axanthin 20- shengdi MOL011455 Hexadecano 418.6 1.91 32.7 -0.24 -0.4 0.7 0.29 104 ylingenol huanglian MOL001454 berberine 336.4 3.45 36.86 1.24 0.57 0.8 0.19 6.57 huanglian MOL013352 Obacunone 454.6 2.68 43.29 0.01 -0.4 0.8 0.31 -13 huanglian MOL002894 berberrubine 322.4 3.2 35.74 1.07 0.17 0.7 0.24 6.46 huanglian MOL002897 epiberberine 336.4 3.45 43.09 1.17 0.4 0.8 0.19 6.1 huanglian MOL002903 (R)-Canadine 339.4 3.4 55.37 1.04 0.57 0.8 0.2 6.41 huanglian MOL002904 Berlambine 351.4 2.49 36.68 0.97 0.17 0.8 0.28 7.33 Corchorosid huanglian MOL002907 404.6 1.34 105 -0.91 -1.3 0.8 0.29 6.68 e A_qt Magnogrand huanglian MOL000622 266.4 1.18 63.71 0.02 -0.2 0.2 0.3 3.17 iolide huanglian MOL000762 Palmidin A 510.5 4.52 35.36 -0.38 -1.5 0.7 0.39 33.2 huanglian MOL000785 palmatine 352.4 3.65 64.6 1.33 0.37 0.7 0.13 2.25 huanglian MOL000098 quercetin 302.3 1.5 46.43 0.05 -0.8 0.3 0.38 14.4 huanglian MOL001458 coptisine 320.3 3.25 30.67 1.21 0.32 0.9 0.26 9.33 huanglian MOL002668 Worenine -

FAM20B (N-14): Sc-164312
SAN TA C RUZ BI OTEC HNOL OG Y, INC . FAM20B (N-14): sc-164312 BACKGROUND SOURCE Chromosome 1 is the largest human chromosome spanning about 260 million FAM20B (N-14) is an affinity purified goat polyclonal antibody raised against base pairs and making up 8% of the human genome. There are about 3,000 a peptide mapping near the N-terminus of FAM20B of human origin. genes on chromosome 1, and considering the great number of genes there are also a large number of diseases associated with chromosome 1. Notably, the PRODUCT rare aging disease Hutchinson-Gilford progeria is associated with the LMNA Each vial contains 200 µg IgG in 1.0 ml of PBS with < 0.1% sodium azide gene which encodes lamin A. When defective, the LMNA gene product can and 0.1% gelatin. build up in the nucleus and cause characteristic nuclear blebs. The mechanism of rapidly enhanced aging is unclear and is a topic of continuing exploration. Blocking peptide available for competition studies, sc-164312 P, (100 µg The MUTYH gene is located on chromosome 1 and is partially responsible for peptide in 0.5 ml PBS containing < 0.1% sodium azide and 0.2% BSA). familial adenomatous polyposis. Stickler syndrome, Parkinsons, Gaucher dis - ease and Usher syndrome are also associated with chromosome 1. A break - APPLICATIONS point has been identified in 1q which disrupts the DISC1 gene and is linked FAM20B (N-14) is recommended for detection of FAM20B of mouse, rat and to schizophrenia. Aberrations in chromosome 1 are found in a variety of can - human origin by Western Blotting (starting dilution 1:200, dilution range cers including head and neck cancer, malignant melanoma and multiple myelo - 1:100-1:1000), immunofluorescence (starting dilution 1:50, dilution range ma. -

Og Raunvísindasvið - Líftækni
Háskólinn á Akureyri Viðskipta- og raunvísindasvið - Líftækni Námskeið LOK1126 og LOK1226 Heiti verkefnis Characterization of cathelicidin gene family members in Rock Ptarmigan (Lagopus muta) Verktími Janúar – maí 2017 Nemandi Hallgrímur Steinsson Leiðbeinandi Kristinn Pétur Magnússon Upplag Rafrænt auk þriggja prentaðra eintaka Blaðsíðufjöldi 53 Fjöldi viðauka 1 Fylgigögn Engin Útgáfu- og notkunarréttur Opið verkefni Yfirlýsingar „Ég lýsi því yfir að ég einn er höfundur þessa verkefnis og að það er afrakstur eigin rannsókna“ _________________________________ Hallgrímur Steinsson, 210878-5649 „Það staðfestist að verkefni þetta fullnægir að mínum dómi kröfum til prófs í námskeiðunum LOK1126 og LOK1226“ __________________________________ Kristinn P. Magnússon, leiðbeinandi ii Abstract Cathelicidins are a class of antimicrobial peptides expressed in vertebrate species which are part of the innate immune system. The aim of this thesis was to resolve genomic organization of the cathelicidin gene cluster in rock ptarmigan (Lagopus muta) and to predict the amino sequence of the mature peptides and analyze expression. To locate the cathelicidin genes the chicken (Gallus gallus) genome sequences were used to blast a novel draft genome of rock ptarmigan. The draft genome was subsequently used to design primers for PCR and sequencing, to enable obtaining the entire cathelicidin cluster. The characterization of the cathelicidin cluster in rock ptarmigan revealed all four cathelicidin genes orthologues found in chicken and turkey (Meleagris gallopavo), namely CATHL1, CATH2, CATH3, CATHB1, flanked by KLH18 and TBRG4, in the same order on chromosome 2. The genes map to a 15kb region, which is of similar size in chicken. The quality of the region is good except for two minor gaps of ~100bp. -

Product Sheet CA1009
API5 Antibody Applications: WB, IHC Detected MW: 51 kDa Cat. No. CA1009 Species & Reactivity: Human, Rat Isotype: Rabbit IgG BACKGROUND APPLICATIONS The apoptosis inhibitor-5 [API5; antiapoptosis Application: *Dilution: clone 11 (AAC-11); fibroblast growth factor-2 WB 1:1000 (FGF2)-interacting factor (FIF)] is a 504-aa IP n/d nuclear protein whose expression has been shown IHC 1:50-200 to prevent apoptosis after growth factor ICC n/d deprivation. It was shown that its antiapoptotic action seems to be mediated, at least in part, by FACS n/d *Optimal dilutions must be determined by end user. the suppression of the transcription factor E2F1- induced apoptosis. Moreover, it was also reported that API5 interacts with, and negatively regulates Acinus, a protein involved in apoptotic DNA QUALITY CONTROL DATA fragmentation. API5 can form homo-oligomers, through a leucine-zipper (LZ) motif, and oligomerization-deficient mutants of AAC-11 can no longer inhibit apoptosis nor interact with Acinus.1 The API5gene has been shown to be highly expressed in multiple cancer cell lines as well as in some metastatic lymph node tissues and in B-cell chronic lymphoid leukemia. API5 expression seems to confer a poor outcome in subgroups of patients with non-small cell lung carcinoma, whereas its depletion seems to be tumor cell lethal under condition of low-serum stress. Interestingly, API5 overexpression has been reported to promote both cervical cancer cells growth and invasiveness. Combined, these observations implicate API5as a putative metastatic oncogene and suggest that API5 could constitute a therapeutic target in cancer.2 References: 1. -
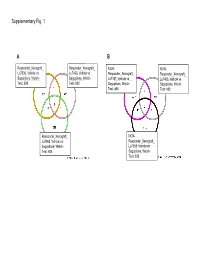
Supplementary Data
Supplementary Fig. 1 A B Responder_Xenograft_ Responder_Xenograft_ NON- NON- Lu7336, Vehicle vs Lu7466, Vehicle vs Responder_Xenograft_ Responder_Xenograft_ Sagopilone, Welch- Sagopilone, Welch- Lu7187, Vehicle vs Lu7406, Vehicle vs Test: 638 Test: 600 Sagopilone, Welch- Sagopilone, Welch- Test: 468 Test: 482 Responder_Xenograft_ NON- Lu7860, Vehicle vs Responder_Xenograft_ Sagopilone, Welch - Lu7558, Vehicle vs Test: 605 Sagopilone, Welch- Test: 333 Supplementary Fig. 2 Supplementary Fig. 3 Supplementary Figure S1. Venn diagrams comparing probe sets regulated by Sagopilone treatment (10mg/kg for 24h) between individual models (Welsh Test ellipse p-value<0.001 or 5-fold change). A Sagopilone responder models, B Sagopilone non-responder models. Supplementary Figure S2. Pathway analysis of genes regulated by Sagopilone treatment in responder xenograft models 24h after Sagopilone treatment by GeneGo Metacore; the most significant pathway map representing cell cycle/spindle assembly and chromosome separation is shown, genes upregulated by Sagopilone treatment are marked with red thermometers. Supplementary Figure S3. GeneGo Metacore pathway analysis of genes differentially expressed between Sagopilone Responder and Non-Responder models displaying –log(p-Values) of most significant pathway maps. Supplementary Tables Supplementary Table 1. Response and activity in 22 non-small-cell lung cancer (NSCLC) xenograft models after treatment with Sagopilone and other cytotoxic agents commonly used in the management of NSCLC Tumor Model Response type