Needs Assesment for the Mental Disability Advocacy Program
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Proposal for FOSS4G Europe 2020 Valmiera Th 30 September 2019
Proposal for FOSS4G Europe 2020 Valmiera th 30 September 2019 OVERVIEW In cooperation with Valmiera City council and Valmiera Development Agency we propose the FOSS4G Europe 2020 conference to take place in Valmiera, Latvia. We would like to propose the FOSS4G Europe 2020 conference to take place in Valmiera as the international nor european FOSS4G events have not yet been to this North-Eastern part of Europe. Latvia is democratic republic for almost 30 years and part of the European Union for the past 15 years the conference would be set in an environment that the FOSS4GE event has not been in before. As with Latvia’s setting in the zigzag of history the guiding motto behind the conference would be to remember the past but look and live for the future. Valmiera is a town situated in the historic Vidzeme region on the banks of the Gauja river. About 100 km North-East from the Latvian capital Rīga, and 50 km from the Estonian Southern border. The place dates back to the 13th century; Valmiera was founded in 1283 with city rights granted in 1323. Valmiera was a site of the Livonian Order (an autonomous branch of the Teutonic Order) stronghold - Valmiera castle. To this day the castle’s ruins lie in the city centre. Most of the old buildings dating back to the 18th-19th century were destroyed in the fires during the last war. Nevertheless we would like to urge the participants to discover the city and its historic surroundings as an extracurricular activity to the conference: hiking the Gauja National Park, kayaking on the Gauja river, bobsleighing in Sigulda, and a visit to the Turaida castle. -

Intrazonal Agricultural Resources in Kurzeme Peninsula
ECONOMICS INTRAZONAL AGRICULTURAL RESOURCES IN KURZEME PENINSULA Linda Siliòa Latvia University of Agriculture e-mail: [email protected] Abstract The paper focuses on the exposition of the research results on agricultural resources in Kurzeme peninsula–climatic resources, qualitative evaluation of the land, condition of land amelioration, topographic resources, and structural breakdown of farm land by types of use. It is concluded that extremely various climatic and soil conditions govern in the region. The Southeast part of Kurzeme peninsula is displayed very favourably by the aggregate value of agricultural resources. Labour productivity in Kurzeme has been analysed as well. Key words: agriculture, factor, peninsula, resources. Introduction ferent and even extremely different. These aspects have Encyclopaedical publication ‘Pasaules zemes un stimulated more profound or profound complex research tautas’ (Lands and Peoples of the World, 1978) defines on each intrazone or micro-region, or sub-district of natu- Kurzeme peninsula as the Northwest part of Latvia lying ral conditions. between the Baltic Sea in the West and the Riga Gulf in the K. Brîvkalns (1959), a researcher of soil and natural East. conditions, has displayed five sub-districts or intrazones of Latvian geographers (Latvijas ìeogrâfija, 1975) char- natural conditions (soils) in Kurzeme: acterise Kurzeme peninsula and its intrazonal differences • coastal sandy lowland (1a) stretching along the from climatic (Temòikova, 1958), relief, soil, and other as- coasts of the Baltic Sea and the Riga Gulf and covers pects essential for agriculture (Brîvkalns et al., 1968). the Northern part of the region; The total length of the sea and gulf borderline is twice • Western Kurzeme plain and hill land (2a) – parts of longer than its land borderline, where it verges on Dobele Liepâja and Kuldîga districts; and Riga districts. -
Summary of the Development Vision 2030 for Tourism and Transport Corridor of the VIA Hanseatica Route
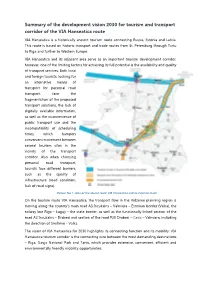
Summary of the development vision 2030 for tourism and transport corridor of the VIA Hanseatica route VIA Hanseatica is a historically ancient tourism route connecting Russia, Estonia and Latvia. This route is based on historic transport and trade routes from St. Petersburg through Tartu to Riga and further to Western Europe. VIA Hanseatica and its adjacent area serve as an important tourism development corridor, however, one of the limiting factors for achieving its full potential is the availability and quality of transport services. Both local and foreign tourists, looking for an alternative means of transport for personal road transport, face the fragmentation of the proposed transport solutions, the lack of digitally available information, as well as the inconvenience of public transport use and the incompatibility of scheduling times, which hampers convenient movement between several tourism sites in the vicinity of the transport corridor. Also when choosing personal road transport, tourists face different barriers, such as the quality of infrastructure (road condition, lack of road signs). Picture No 1: Area of the tourist route VIA Hanseatica and its external reach On the tourism route VIA Hanseatica, the transport flow in the Vidzeme planning region is moving along the country's main road A3 Incukalns – Valmiera – Estonian border (Valka), the railway line Riga – Lugaji – the state border, as well as the functionally linked section of the road A2 Incukalns – Drabesi and section of the road P20 Drabesi – Cesis – Valmiera, including the direction of Smiltene - Valka. The vision of VIA Hanseatica for 2030 highlights its connecting function and its mobility: VIA Hanseatica tourism corridor is the connecting wire between the most demanding destinations – Riga, Gauja National Park and Tartu, which provides extensive, convenient, efficient and environmentally friendly mobility opportunities. -

Chapter 3 Chapter 3 Potential Analysis of Regional Development
CHAPTER 3 CHAPTER 3 POTENTIAL ANALYSIS OF REGIONAL DEVELOPMENT 3.1 National and Regional Policy on Socioeconomic Development 3.1.1 Review of Development Policy Latvia aims at ensuring equal working, income, social, and cultural opportunities for all inhabitants of the state, as mentioned in the following legislation, development strategies and policies. However, the former course of development after independence in 1991 has resulted in differences in living environment and opportunities of economic activity in different regions of Latvia. In many areas including LWC, insufficient economic development and activity, high unemployment rate, low income, unequal conditions for social and cultural life have been found. (1) Law on Spatial Development Planning of Latvia The Law on Spatial Development Planning of Latvia was adopted in October 1998. According to this new law, development and land use planning in Latvia is to be carried out, as such: - Local governments of districts, state cities, towns, and townships should prepare spatial development plans of their administrative areas, - Spatial development plans of higher level should be observed when producing spatial development plans of lower levels, and - Land use plans of regional and local municipal levels should be prepared in accordance with the relevant spatial development plans. Development and land use plans for LWC, therefore, has to observe and coordinate with the directions and strategies mentioned in the existing national, regional, district, and township level plans. (2) National development strategies The long-term goal of development strategy for Latvia is to become a socially harmonized country with a dynamic, open and equal opportunity as well as its own national identity. -

JSC “Latvian State Roads”
JSC “Latvian State Roads” Annual Report 2004 JSC “Latvian State Roads” Annual Report 2004 2 Contents State Joint Stock Company “Latvian State Roads” Today . 4 Structure of State Joint Stock Company “Latvian State Roads” . 7 Personnel . 10 Road Laboratory . 14 Latvian Road Museum . 15 International Co-operation . 17 Resolution of Auditor . 19 Balance . 20 Tax and Social Security Payments . 22 Review on Changes in Equities . 23 Calculation of Reserve Fund for Time Period from January 1 to October 25, 2004 (turnover cost method) . 24 Profit/Loss Calculation for the Period from October 25 to December 31, 2004 (categorised in columns according to period cost method) . 25 Latvian Road Network . 26 Latvian Road Map . 27 Latvian State Roads by District . 28 Latvian State Main Roads by District . 29 Latvian State 1st Class Roads by District . 30 Latvian State 2nd Class Roads by District . 31 3 Annual Report 2004 JSC “Latvian State Roads” Bridges on Latvian State Roads . 32 Location of Bridges on Latvian State Roads . .33 Average Annual Daily Traffic Intensity . 34 Vehicles Registered in Latvia . 36 Road Network Development . 37 Environmental Protection . 40 Road Routine Maintenance . 42 Expenditures for State Road Routine Maintenance in 2004 . 45 Executed Routine Maintenance Works on State Roads in 2004 by District and City . 48 Winter Road Maintenance . 51 Maintenance of State Main and 1st Class Roads in the Winter of 2004/2005 . 52 Road and Bridge Periodic Maintenance and Reconstruction . 53 Road Traffic Organisation . 61 State Road Financing . 66 Financing of Cohesion Fund Projects in the Road Sector . 68 Financing for Investment Project “Improvements in VIA BALTICA Route and West–East Corridor” . -
Healthcare Obstacles to the Efficiency and Effectiveness of Health Systems
Easing legal and administrative obstacles in EU border regions Case Study No. 15 Healthcare Obstacles to the efficiency and effectiveness of health systems (Estonia – Latvia) Written by I. Styczyńska, D. Po February 2017 EUROPEAN COMMISSION Directorate-General for Regional and Urban Policy Directorate D: European Territorial Co-operation, Macro-regions, Interreg and Programme Implementation I Unit D2: Interreg, Cross-Border Cooperation, Internal Borders Contacts: Ana-Paula LAISSY (head of unit), Alexander FERSTL (contract manager) E-mail: [email protected] European Commission B-1049 Brussels EUROPEAN COMMISSION Easing legal and administrative obstacles in EU border regions Case Study No. 15 Healthcare Obstacles to the efficiency and effectiveness of health systems (Estonia – Latvia) Annex to the Final Report for the European Commission Service Request Nr 2015CE160AT013 Competitive Multiple Framework Service Contracts for the provision of Studies related to the future development of Cohesion Policy and the ESI Funds (Lot 3) Directorate-General for Regional and Urban Policy 2017 EN Europe Direct is a service to help you find answers to your questions about the European Union. Freephone number (*): 00 800 6 7 8 9 10 11 (*) The information given is free, as are most calls (though some operators, phone boxes or hotels may charge you). LEGAL NOTICE This document has been prepared for the European Commission however it reflects the views only of the authors, and the Commission cannot be held responsible for any use which may be made of the information contained therein. More information on the European Union is available on the Internet (http://www.europa.eu). -

When the Nearest Hospital Happens to Be Abroad
OVERCOMING OBSTACLES IN BORDER REGIONS WHEN THE NEAREST HOSPITAL HAPPENS TO BE ABROAD Valka and Valga showcase need to share medical services What would you do if you broke your arm and the closest The twin towns of Valka and Valga share a long history hospital was across the border? and were previously one municipality. When Latvia and Estonia joined the Schengen area in 2007, they essentially A woman in the Latvian town of Valka didn’t think twice. became a single urban region again. In much pain, she rushed to a hospital three kilometres away in Valga, Estonia. But despite their proximity and EU regulations guaranteeing the right of citizens access to cross-border medical The decision saved her from a 55 kilometre journey to care, Latvians face a number of obstacles or difficulties the nearest hospital in Latvia. But it came at a cost – linked to a lack of information, language barriers, she ended up paying out of pocket for her treatment complex payment and reimbursement procedures due to hurdles hampering EU cross-border healthcare and onerous administrative requirements. cooperation. The situation in Valka and Valga is not uncommon and highlights the need to bolster healthcare cooperation in EU border regions. Regional and September 2017 Urban Policy One region, one hospital Valka and Valga are virtually one urban area split by an international border instituted in 1991 when the Baltic States regained independence after decades of Soviet rule. However, Valga has a hospital whereas Valka does not. Short of traveling 55 kilometres to the nearest regional Vidzeme hospital in the city of Valmiera, Latvians in Valka with emergencies are left with few options other than to cross into Estonia. -

Interaction Between the Number of Visitors at Tourist Accommodation Establishments and the Economic Development in Latvia
Economics and Rural Development Vol. 8, No. 1, 2012 ISSN 1822-3346 INTERACTION BETWEEN THE NUMBER OF VISITORS AT TOURIST ACCOMMODATION ESTABLISHMENTS AND THE ECONOMIC DEVELOPMENT IN LATVIA Aina Muska1, Ligita Bite2 Latvia University of Agriculture, Latvia The research hypothesis: the economic development of a district affects the number of visitors at tourist accommodation establishments outside Riga region. The research aim is to identify a correlation between the number of visitors at tourist accommodation establishments and the economic development of a district in Latvia. The research was done using data broken down by statistical region and districts (a unit of administrative division of the territory of Latvia until the middle of 2009). The research showed that the majority (more than 60%) of visitors at Latvian tourist accommodation establishments were foreign tourists whose share at Riga tourist accommodation establishments accounted for more than 70%. Outside Riga region, more than 70% of visitors were local (Latvian) tourists, mostly business tourists. In the research period, more than half of visitors at tourist accommodation establishments concentrated in Riga region, while more than 10% – in Pieriga and Kurzeme regions. The share of visitors in the other regions did not exceed 6% of their total number. According to a cluster analysis, an explicit trend of monocentric economic development is specific to Latvia, resulting in significant differences between Riga, the capital city of Latvia, and the other districts of Latvia. The number of visitors at tourist accommodation establishments is higher in the clusters having a high (Riga) and medium (districts of Riga, Liepaja, Ventspils, and Daugavpils) level of economic development than in the clusters with a lower level of economic development (districts of Aluksne, Balvi, Dobele, Gulbene, Kraslava, Ludza, Preili, and Valka). -

ANNEX 2-X WP6 D6.3 Site-Assessment
Project: BiG>East (EIE/07/214) Assessment Studies for Specific Biogas Sites in Latvia Deliverable D 6.3 Submitted by: M.Sc.ing. Ilze Dzene EKODOMA Ltd. Noliktavas street 3-3, Riga LV-1010, Latvia 07 April 2009 With the support of: The sole responsibility for the content of this publication lies with the authors. It does not represent the opinion of the Community. The Euro- pean Commission is not responsible for any use that may be made of the information contained therein. 1 Contents Summary ..................................................................................................................................... 3 Results within Step 1: Selection of the Region......................................................................... 4 Description of the selected regions for potential Biogas Sites................................................. 4 Biogas Site 1: Ėekava parish ............................................................................................... 4 Biogas Site 2: Sesava parish................................................................................................. 6 Biogas Site 3: Zaube parish.................................................................................................. 8 Biomass supply ...................................................................................................................... 10 Biogas Site 1: Ėekava parish ............................................................................................. 10 Biogas Site 2: Sesava parish.............................................................................................. -

Catalogue of Latvian Latridiidae (Insecta: Coleoptera) Andris Bukejsa, Dmitry Telnovb & Wolfgang H
This article was downloaded by: [Andris Bukejs] On: 12 December 2013, At: 23:47 Publisher: Taylor & Francis Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK Zoology and Ecology Publication details, including instructions for authors and subscription information: http://www.tandfonline.com/loi/tzec20 Catalogue of Latvian Latridiidae (Insecta: Coleoptera) Andris Bukejsa, Dmitry Telnovb & Wolfgang H. Rückerc a Vienības iela 42-29, Daugavpils LV-5401, Latvia b Stopiņu novads, Dārza iela 10, Dzidriņas LV-2130, Latvia c Von-Ebner-Eschenbach-Straße 12, Neuwied D-56567, Germany Published online: 27 Nov 2013. To cite this article: Andris Bukejs, Dmitry Telnov & Wolfgang H. Rücker (2013) Catalogue of Latvian Latridiidae (Insecta: Coleoptera), Zoology and Ecology, 23:4, 312-322, DOI: 10.1080/21658005.2013.862060 To link to this article: http://dx.doi.org/10.1080/21658005.2013.862060 PLEASE SCROLL DOWN FOR ARTICLE Taylor & Francis makes every effort to ensure the accuracy of all the information (the “Content”) contained in the publications on our platform. However, Taylor & Francis, our agents, and our licensors make no representations or warranties whatsoever as to the accuracy, completeness, or suitability for any purpose of the Content. Any opinions and views expressed in this publication are the opinions and views of the authors, and are not the views of or endorsed by Taylor & Francis. The accuracy of the Content should not be relied upon and should be independently verified with primary sources of information. Taylor and Francis shall not be liable for any losses, actions, claims, proceedings, demands, costs, expenses, damages, and other liabilities whatsoever or howsoever caused arising directly or indirectly in connection with, in relation to or arising out of the use of the Content. -

Explore Valka Municipality!
EXPLORE VALKA MUNICIPALITY! The municipality of Valka is located in the north-east of Latvia, on the Estonian border. The municipality is often called “Latvia’s Nord Gate”. There are five parishes and one city in the municipality of Valka. The city of Valka is the centre of the municipality; it is located on the border, so it is called the city where Latvia starts. The Estonian city of Valga is located nearby. When you are in Valka- Valga, you are in two countries at the same time. The national highway and tourism routes run through Valka municipality. In this area you can see unique heritage objects, and can camp or stay at guesthouses. Valka is 157 kilometres from Riga, the capital city of Latvia, and 88 kilometres from the Estonian city of Tartu. You need a passport in order to cross the border. It is a good idea to book before visiting these points of interest! 1 Valka Local History Museum Rīgas Street 64, Valka, ph. +371 64722198, [email protected] 57° 46’ 5” 26° 0’ 23” Jānis Cimze started the first seminary for Vidzeme parish schoolteachers at the 19th century, on the site where the museum now is. Many famous figures of Latvian and Estonian culture and education were educated at this seminary. Due to the museum’s historical location, it seeks to popularize the work of Jānis Cimze, who was a pedagogue and a founder of the Latvian choir singing culture, as well as that of his pupils. It also aims to promote public interest and knowledge concerning the historical events that have taken place in Valka County. -

Law on Judicial Power
Disclaimer: The English language text below is provided by the State Language Centre for information only; it confers no rights and imposes no obligations separate from those conferred or imposed by the legislation formally adopted and published. Only the latter is authentic. The original Latvian text uses masculine pronouns in the singular. The State Language Centre uses the principle of gender-neutral language in its English translations. In addition, gender-specific Latvian nouns have been translated as gender-neutral terms, e.g. chairperson. Text consolidated by Valsts valodas centrs (State Language Centre) with amending laws of: 16 December 1993; 15 June 1994; 6 April 1995; 28 September 1995; 21 December 1995; 23 May 1996; 29 January 1997; 1 October 1997; 14 October 1998; 15 October 1998; 11 November 1999; 8 November 2001; 31 October 2002; 19 June 2003; 4 December 2003; 17 March 2005; 22 September 2005; 28 September 2005; 23 February 2006; 2 November 2006; 8 November 2007; 3 April 2008; 14 November 2008; 12 December 2008; 30 April 2009. If a whole or part of a section has been amended, the date of the amending law appears in square brackets at the end of the section. If a whole section, paragraph or clause has been deleted, the date of the deletion appears in square brackets beside the deleted section, paragraph or clause. The Supreme Council of the Republic of Latvia has adopted a Law: On Judicial Power Part I General Provisions Chapter I Judicial Power Section 1. Judicial Power (1) An independent judicial power exists in the Republic of Latvia, alongside the legislative and the executive power.