A Case Study of Mukuru Kwa Njenga, Nairobi
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Efficiency of Nairobi's Kariobangi Wastewater Treatment Plant
THE EFFICIENCY OF NAIROBI’S KARIOBANGI WASTEWATER TREATMENT PLANT BY ANDERE CLEMENT MIRUKA REG. NO: I56/69022/2013 A RESEARCH THESIS SUBMITTED IN PARTIAL FULFILLMENT FOR THE AWARD OF THE DEGREE OF MASTER OF SCIENCE IN ENVIRONMENTAL CHEMISTRY OF THE UNIVERSITY OF NAIROBI AUGUST, 2016 DECLARATION This thesis is my original idea and has never been presented for award of a degree at any other University Sign……………………………………. Date…………………………………… Andere Clement Miruka. This thesis is submitted with our approval as research supervisors Sign……………………………………. Date………………………………………. Prof. David K. Kariuki. Department of Chemistry, University of Nairobi Sign……………………………………. Date……………………………………… Prof. Amir O. Yusuf Department of Chemistry, University of Nairobi Sign……………………………………. Date……………………………………… Dr. John O. Onyatta Department of Chemistry, University of Nairobi ii ABSTRACT Kariobangi Sewerage Treatment Plant in Nairobi City County is a conventional mechanical wastewater treatment plant with an installed capacity of 32,000 m3/day and has an in built methenation unit. It is the only available conventional mechanical wastewater treatment plant in the city and its efficiency is therefore, of paramount importance. A total of 48 samples from three sites within the plant namely the Inlet (I), the Clarifier(C) and the Outlet (O) were analyzed for various parameters. Development activities within the treatment plant’s catchment area were assessed with view to establish their effects on the performance of the plant. Physico-chemical parameters, chemical parameters, heavy metals, oil & grease and bacteriological presence analyses were carried out so as to evaluate the efficiency of the plant. The physico-chemical parameters analyzed included settleable solids (SS), chemical oxygen demand (COD), and biochemical oxygen demand after five days (BOD5). -

Slum Toponymy in Nairobi, Kenya a Case Study Analysis of Kibera
Urban and Regional Planning Review Vol. 4, 2017 | 21 Slum toponymy in Nairobi, Kenya A case study analysis of Kibera, Mathare and Mukuru Melissa Wangui WANJIRU*, Kosuke MATSUBARA** Abstract Urban informality is a reality in cities of the Global South, including Sub-Saharan Africa, which has over half the urban population living in informal settlements (slums). Taking the case of three informal settlements in Nairobi (Kibera, Mathare and Mukuru) this study aimed to show how names play an important role as urban landscape symbols. The study analyses names of sub-settlements (villages) within the slums, their meanings and the socio-political processes behind them based on critical toponymic analysis. Data was collected from archival sources, focus group discussion and interviews, newspaper articles and online geographical sources. A qualitative analysis was applied on the village names and the results presented through tabulations, excerpts and maps. Categorisation of village names was done based on the themes derived from the data. The results revealed that village names represent the issues that slum residents go through including: social injustices of evictions and demolitions, poverty, poor environmental conditions, ethnic groupings among others. Each of the three cases investigated revealed a unique toponymic theme. Kibera’s names reflected a resilient Nubian heritage as well as a diverse ethnic composition. Mathare settlements reflected political struggles with a dominance of political pioneers in the village toponymy. Mukuru on the other hand, being the newest settlement, reflected a more global toponymy-with five large villages in the settlement having foreign names. Ultimately, the study revealed that ethnic heritage and politics, socio-economic inequalities and land injustices as well as globalization are the main factors that influence the toponymy of slums in Nairobi. -

Slum Growth and Space Transformation: the Implication on Service Delivery and Environment Gathogo P. Kimotho B63/80699/2012 a Re
Slum Growth and Space Transformation: The Implication on Service Delivery and Environment Gathogo P. Kimotho B63/80699/2012 A Research Thesis Submitted in Partial Fulfilment of the Requirements for the Award of the Degree of Master of Arts in Planning of the University of Nairobi. June, 2015 i Declaration I Kimotho Gathogo hereby certify that this is my original work and it has not been presented to any other academic or professional institution for scholarly purposes or otherwise. Signed: Kimotho Gathogo………………………………………..Date: ………………… Supervisor: Dr. Musyimi Mbathi………………………………….Date:………………… ii Dedication: iii Acknowledgement I sincerely thank my supervisor Dr. Musyimi Mbathi for the invaluable support, guidance and encouragement he offered before and during the research period. I would not have achieved this work without your assistance. Secondly, I wish to sincerely thank Dr. Fridah Mugo who put in long hours to read and correct my work. My sincere gratitude also goes out to Dr. Romanus Opiyo for the encouragement and ideas during the research period, I remain forever grateful. Also not leaving out Mr. Zack Maleche and Mr. Karisa Dadu who really assisted me during the formulation of the research proposal. Special appreciation to Dr. Kenneth Mubea for the brilliant GIS and remote sensing ideas and for the encouragement and mentoring all through my postgraduate studies. Also special appreciation to Miss. Wangechi Weru who was always by my side encouraging me even when I almost gave up. I am forever grateful to my superiors at work Eng. Evans Kinyua and Eng. Kenneth Gitahi for the invaluable assistance they offered during my study period. -

Automated Clearing House Participants Bank / Branches Report
Automated Clearing House Participants Bank / Branches Report 21/06/2017 Bank: 01 Kenya Commercial Bank Limited (Clearing centre: 01) Branch code Branch name 091 Eastleigh 092 KCB CPC 094 Head Office 095 Wote 096 Head Office Finance 100 Moi Avenue Nairobi 101 Kipande House 102 Treasury Sq Mombasa 103 Nakuru 104 Kicc 105 Kisumu 106 Kericho 107 Tom Mboya 108 Thika 109 Eldoret 110 Kakamega 111 Kilindini Mombasa 112 Nyeri 113 Industrial Area Nairobi 114 River Road 115 Muranga 116 Embu 117 Kangema 119 Kiambu 120 Karatina 121 Siaya 122 Nyahururu 123 Meru 124 Mumias 125 Nanyuki 127 Moyale 129 Kikuyu 130 Tala 131 Kajiado 133 KCB Custody services 134 Matuu 135 Kitui 136 Mvita 137 Jogoo Rd Nairobi 139 Card Centre Page 1 of 42 Bank / Branches Report 21/06/2017 140 Marsabit 141 Sarit Centre 142 Loitokitok 143 Nandi Hills 144 Lodwar 145 Un Gigiri 146 Hola 147 Ruiru 148 Mwingi 149 Kitale 150 Mandera 151 Kapenguria 152 Kabarnet 153 Wajir 154 Maralal 155 Limuru 157 Ukunda 158 Iten 159 Gilgil 161 Ongata Rongai 162 Kitengela 163 Eldama Ravine 164 Kibwezi 166 Kapsabet 167 University Way 168 KCB Eldoret West 169 Garissa 173 Lamu 174 Kilifi 175 Milimani 176 Nyamira 177 Mukuruweini 180 Village Market 181 Bomet 183 Mbale 184 Narok 185 Othaya 186 Voi 188 Webuye 189 Sotik 190 Naivasha 191 Kisii 192 Migori 193 Githunguri Page 2 of 42 Bank / Branches Report 21/06/2017 194 Machakos 195 Kerugoya 196 Chuka 197 Bungoma 198 Wundanyi 199 Malindi 201 Capital Hill 202 Karen 203 Lokichogio 204 Gateway Msa Road 205 Buruburu 206 Chogoria 207 Kangare 208 Kianyaga 209 Nkubu 210 -

Kenya 2020 Human Rights Report
KENYA 2020 HUMAN RIGHTS REPORT EXECUTIVE SUMMARY Kenya is a republic with three branches of government: an executive branch, led by a directly elected president; a bicameral parliament consisting of the Senate and National Assembly; and a judiciary. In the 2017 general elections, the second under the 2010 constitution, citizens cast ballots for president, deputy president, and parliamentarians, as well as county governors and legislators. International and domestic observers judged the elections generally credible, although some civil society groups and the opposition alleged there were irregularities. The Independent Electoral and Boundaries Commission declared Jubilee Coalition Party candidate Uhuru Kenyatta had won re-election as president over opposition candidate Raila Odinga. The Supreme Court subsequently annulled the results for president and deputy president, citing irregularities, and the court ordered a new vote for president and deputy president that the opposition boycotted. The Independent Electoral and Boundaries Commission declared President Kenyatta winner of the new vote, and the Supreme Court upheld the results. The National Police Service maintains internal security and reports to the Ministry of Interior and Coordination of National Government. The National Intelligence Service collects intelligence internally as well as externally and reports directly to the president. The Kenya Defense Forces report to the Ministry of Defense and are responsible for external security but have some domestic security responsibilities, -

KASARANI CONSTITUENCY Oct 2002
TABLE OF CONTENTS Preface…………………………………………………………………….. i 1. District Context………………………………………………………… 1 1.1. Demographic characteristics………………………………….. 1 1.2. Socio-economic Profile………………………………………….. 1 2. Constituency Profile………………………………………………….. 1 2.1. Demographic characteristics………………………………….. 1 2.2. Socio-economic Profile………………………………………….. 2 2.3. Electioneering and Political Information……………………. 2 2.4. 1992 Election Results…………………………………………… 2 2.5. 1994 By-Elections results-1…………………………………… 2 2.6. 1994 By-Elections results-2…………………………………… 3 2.7. 1997 Election Results…………………………………………… 3 2.8. Main problems……………………………………………………. 3 3. Constitution Making/Review Process…………………………… 4 3.1. Constituency Constitutional Forums (CCFs)………………. 4 3.2. District Coordinators……………………………………………. 6 4. Civic Education………………………………………………………… 7 4.1. Phases covered in Civic Education 4.2. Issues and Areas Covered 7 7 5. Constituency Public Hearings……………………………………… 7 5.1. Logistical Details…………………………………………………. 5.2. Attendants Details……………………………………………….. 7 5.3. Concerns and Recommendations…………………………….. 8 8 Appendices 33 1. DISTRICT CONTEXT Kasarani constituency falls within Nairobi province. 1.1. Demographic Characteristics Male Female Total District Population by Sex 1,153,828 989,426 2,143,254 Total District Population Aged 18 years & 397,038 429,639 826,677 Below Total District Population Aged Above 18 756,790 559,787 1,316,577 years District Population by sex 1,153,828 989,426 2,143,254 Population Density (persons/Km2) 3,079 1.2. Socio-economic Profile Nairobi province has: • The highest urban population in Kenya. • The highest population density. • A young population structure. • The highest monthly mean household income in the country and the least number of malnourished children • More than 50% of the population living in absolute poverty • High inequalities by class and other social economic variables • Very low primary and secondary school enrollments • Poor access to safe drinking water and sanitation Nairobi has eight constituencies. -

Kenya's Scorecard on Security and Justice : Broken Promises And
Kenya’s scorecard on security and justice : Broken promises and unfinished business Report July 2017 / 696/a Cover Picture: Kenyan riot police officers hold batons as they detain a suspected supporter of the Kenya’s opposition Coalition for Reforms and Democracy (CORD), during a protest on May 16, 2016 in Nairobi, outside the headquarters of the Independent Electoral and Boundaries Commission (IEBC). Opposition protestors led by former Prime Minister Raila Odinga gathered outside the Indepedent Electoral and Boundaries Comission building to demand the dismissal of IEBC commissioners, after alleged bias towards the ruling Jubillee Alliance Party. TABLE OF CONTENTS LIST OF ABBREVATIONS AND ACRONYMS 4 EXECUTIVE SUMMARY 6 MetHODoloGY 8 INTRODUctION 8 I. SECURITY SECTOR REFORM : INSTITUTIONAL PARALYSIS AT THE EXPENSE OF HUMAN RIGHTS 9 A. Legal and institutional framework 9 A.1. Legal Framework 9 A.2. Key institutions in the security sector 11 A.3 Structure of the security agencies 13 B. Persisting deficiencies within the security sector 13 B.1. Security agencies remain one of the main perpetrators of human rights violations 13 B.1.1 Human rights violations arising from counter-terrorism measures 14 B.1.2 Normalization and Digitization of Extra-judicial killings and executions 17 B.1.3 Policing protests 22 B.1.4 Lack of Transparency, Coordination and Accountability in Joint Security Operations 24 B.1.5 Increase in illegal firearms 25 B.1.6 Surveillance and digital security 26 B.1.7 Security challenges in the context of the 2017 general elections 28 B.2. Persisting weaknesses in the accountability process for security agencies 30 B.2.1 General accountability for human rights violations by security agencies 30 B.2.2 Accountability of the police 31 B.2.3 Accountability of the military 37 B.3. -
Chapter 5: Nairobi and Its Environment
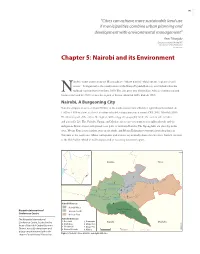
145 “Cities can achieve more sustainable land use if municipalities combine urban planning and development with environmental management” -Ann Tibaijuki Executive Director UN-HABITAT Director General UNON 2007 (Tibaijuki 2007) Chapter 5: Nairobi and its Environment airobi’s name comes from the Maasai phrase “enkare nairobi” which means “a place of cool waters”. It originated as the headquarters of the Kenya Uganda Railway, established when the Nrailhead reached Nairobi in June 1899. The city grew into British East Africa’s commercial and business hub and by 1907 became the capital of Kenya (Mitullah 2003, Rakodi 1997). Nairobi, A Burgeoning City Nairobi occupies an area of about 700 km2 at the south-eastern end of Kenya’s agricultural heartland. At 1 600 to 1 850 m above sea level, it enjoys tolerable temperatures year round (CBS 2001, Mitullah 2003). The western part of the city is the highest, with a rugged topography, while the eastern side is lower and generally fl at. The Nairobi, Ngong, and Mathare rivers traverse numerous neighbourhoods and the indigenous Karura forest still spreads over parts of northern Nairobi. The Ngong hills are close by in the west, Mount Kenya rises further away in the north, and Mount Kilimanjaro emerges from the plains in Tanzania to the south-east. Minor earthquakes and tremors occasionally shake the city since Nairobi sits next to the Rift Valley, which is still being created as tectonic plates move apart. ¯ ,JBNCV 5IJLB /BJSPCJ3JWFS .BUIBSF3JWFS /BJSPCJ3JWFS /BJSPCJ /HPOH3JWFS .PUPJOF3JWFS %BN /BJSPCJ%JTUSJDUT /BJSPCJ8FTU Kenyatta International /BJSPCJ/BUJPOBM /BJSPCJ/PSUI 1BSL Conference Centre /BJSPCJ&BTU The Kenyatta International /BJSPCJ%JWJTJPOT Conference Centre, located in the ,BTBSBOJ 1VNXBOJ ,BKJBEP .BDIBLPT &NCBLBTJ .BLBEBSB heart of Nairobi's Central Business 8FTUMBOET %BHPSFUUJ 0510 District, has a 33-story tower and KNBS 2008 $FOUSBM/BJSPCJ ,JCFSB Kilometres a large amphitheater built in the Figure 1: Nairobi’s three districts and eight divisions shape of a traditional African hut. -

Kenya: Evicted Residents Vulnerable to Covid-19
First UA: 75/20 Index: AFR 32/2284/2020 Kenya Date: 7 May 2020 URGENT ACTION EVICTED RESIDENTS VULNERABLE TO COVID-19 Despite obtaining interim orders from the Environment and Lands Court halting the evictions, more than 7,000 households of Kariobangi Sewerage Farmers Slum, Korogocho Market, Kisumu Ndogo and Nyayo Village, Nairobi, Kenya, were forcibly evicted by the Nairobi City Water and Sewerage Company (NCWSC) between 4 and 6 May. Residents have title deeds to their homes and have been paying levies to the county government for the land. The NCWSC has rendered residents homeless during the Covid-19 pandemic, increasing their vulnerability to contracting the virus. TAKE ACTION: WRITE AN APPEAL IN YOUR OWN WORDS OR USE THIS MODEL LETTER H.E Uhuru Kenyatta The President of the Republic of Kenya and Commander in Chief of the Armed Forces Office of the President PO Box 62345 – 00200 Nairobi, Kenya Email: [email protected] Twitter: @UKenyatta Dear H.E, President Uhuru Kenyatta, I am very concerned that more than 7,000 households from Kariobangi Sewerage Farmers Slum, Korogocho Market, Kisumu Ndogo and Nyayo Village have been left homeless after facing forced eviction by the NCWSC between 4 and 6 May. On 2 May, the Officer Commanding Police Division of Starehe Division and Deputy County Commissioner told residents of Kariobangi Sewerage Farmers Slum to vacate their homes and allow NCWSC to use the land to which they claimed ownership. However, residents have title deeds and have been paying land rates or levies to the government for the land. On 3 May, the residents sought and obtained an interim order from the Environment and Land Court to halt the eviction until the matter was heard on 7 May. -

Nairobi Matatu Routes Thika Town
GITHUNGURI KIAMBU ROAD NAIROBI MATATU ROUTES THIKA TOWN 237 120 Route Outbound Inbound BOMA ROAD 36 From City Center 33 To City Center 48B 116 LIMURU Stop Terminus City Center Junction RUIRU TOWN Kiambu Komarocks Westlands Yaya 145D 100/100A 19C 48 Jacaranda Githunguri Lavington 145B 145 34B 48A 120 Kayole KAYOLE Valley Arcade BYPASS Ndumberi 1960 LIMURU ROAD Kayole 48B/O KIAMBU ROAD KIAMBU RD. 121 Yaya NDUMBERI Clayworks Mwiki KILELESHWA 1961C 120 BANANA TERMINUS 107D Caltex Kayole 48C 17B Kangemi 121 KIAMBU KENYATTA Baba Ndogo 1961CK GOLF UNIVERSITY Pipeline Jogoo 22/23 25 Uthiru Lucky Summer 33PJ THIKA RD. THIKA 30 106 Pipeline Mombasa Kikuyu KENYATTA 25A 116 M COFFEE UNIVERSITY Kariobangi 33PM KIAMBU JKIA 105 ESTATE Limuru 27 WAY WAIYAKI Kahawa EMBAKASI 34J Sukari Mathare N 114W/115/135 135 Lunga Lunga 237 29/30 Wangige 115 WINDSOR Ngumba 70/71 GOLF KAHAWA WEST 145 South C 118 Wangige 114W RUAKA Kahawa KARURA 45K 43 Wendani KU 12C KPA 119 44Z 107 44G/Z Gathiga ELDORET-MALABA RD Thindigwa 12D 44K Roysambu KU Fedha Estate 119A Highridge 44G 44K 33B/FED Githurai 11A GITHURAI Ruai Bypass RD. PARKLANDS KWAHERI MARURUI Ruaka NORTHERN BYPASS RD. MOMBASA 45G 33H 107D KU Utawala 11F WANGIGE 44 Banana PROGGIE 45K 33UTW USUI LIMURU ROAD 121 45P Githurai Proggie Athiriver 106 Car Wash Ndenderu 45P 110ATH 120 Sunton Kitengela 107 118 GATHIGA Runda KING’EERO GICHAGI LIMURU RD. UN Gichagi Roysambu Footbridge 110KIT 100A 49 Strathmore 103 129 EASTERN BYPASS Ruiru Town 108 Kasarani Corner Stone Limuru Police Naivas Academy 100 14A 145 Deep West 108 116 Ridgeways 53 Ruiru Town Torrents (Loop) Karen Dagoretti Village Market ROYSAMBU/ 14B Safari Park Seasons GETATHURU ROAD 119A 145D Langata 237 KASARANI 17B 1 REDHILL Thika Town Rikana Joster 145 15 Garden City / 49 237 Highrise 119 Homeland Eastleigh RD. -

Corruption and Rural Communal Conflicts
Riskline / Country Report / 29 August 2021 KENYA Overall risk level High Reconsider travel Can be dangerous and may present unexpected security risks Travel is possible, but there is a potential for disruptions Overview Emergency Numbers Emergency 112 Emergency 999 Upcoming Events 30 August 2021 - 14 September 2021 Medium risk: Chinese officials suspend Nairobi-Changsha flights from 30 August-13 September- Update Chinese authorities announced that China Southern Airlines flight CZ6044 from Nairobi Airport (NBO/HKJK) in Kenya to Changsha Huanghua Airport (CSX/ZGHA) in China was suspended from 30 August for two weeks, due to COVID-19. Riskline / Country Report / 29 August 2021 / Kenya 2 Travel Advisories High risk: Banditry and cattle raids in central Kenya Reconsider travel to Baringo, Elgeyo Marakwet, Isiolo, Laikipia, southern Marsabit, Meru, Nyeri, Saduru, Trans Nzoia, southern Turkana and West Pokot until further notice, due to ongoing bandit attacks and insecurity. Banditry has been on the rise in areas of central Kenya since 2017, particularly in the west-central counties of Baringo, Elgeyo Marakwet, Laikipia, Saduru, (southern) Turkana and West Pokot and the central counties of Isiolo and (southern) Marsabit. The uptick in raids and clashes with local communities perpetrated primarily by armed herders is likely linked to a confluence of factors: drought conditions, overgrazing of animals, increasing rates of firearm ownership and even local political disputes. While the attacks have largely targeted members of the local community, a British national was killed in March 2017 while investigating burning buildings on a ranch in Laikipia. Security forces in the region also come under periodic attack, as was the case in the Jaldesa and Kukuto areas of Marsabit County, where at least 10 people, including two police officers, were killed by bandits in August 2019. -

Interruptions 05 05 2016.Pdf
AREA: NGONG VET, KERARAPON, BULBUL AREA: SIRIKWA QUARRY, KAMUKUNJI, KAPCHEROP DATE: Wednesday 11.05.2016 TIME: 9.00 A.M. – 5.00 P.M. DATE: Sunday 08.05.2016 TIME: 9.00 A.M. – 5.00 P.M. Part of Ngong Town, Scheme 305, Zambia, Olepolos, Ngong Vet, Kamukunji Est, Kiplombe, Kiplombe High Sch, Karetik, Richo Bulbul, Kerarapon & adjacent customers. Farm Kapsang, Kabenes Centre AIC, Kosyin High Sch, Ziwa Notice is hereby given under rule 27 of the Electric Power Rules that Centre, Mkonge Farm, Mkonge High Sch, Kapcherop, AIC Sango, AREA: PART OF RIVERSIDE DRIVE the electricity supply will be interrupted as here under: Kerotet Girls, Kabenes Centre, Twigaa Dispensary, Twigaa Mkt, DATE: Thursday 12.05.2016 TIME: 9.00 A.M. – 5.00 P.M. (It is necessary to interrupt supply periodically in order to Mwituti Sec Sch, Kipkeinyo Centre, Sirikwa Quarry, Tai Quarry, Mzima Springs Rd, Part of Riverside Drive, Mbabane Rd, Part of facilitate maintenance and upgrade of power lines or equipment Kimiriri Quarry, Lochab Quarry, Kaptinga Quarry, Kosyin Centre for better quality supply; to connect new lines to the network; Convent Rd, Chalbi Drive, Njumbi Rd, Amboseli Rd, Amboseli Lane, & adjacent customers. to connect new customers or to relocate power lines during road Lavington West Est, Kabarserian Rd, Waruku & adjacent customers. construction, etc.) TRANS NZOIA COUNTY NAIROBI NORTH REGION AREA: NAZARENE UNIVERSITY DATE: Thursday 12.05.2016 TIME: 9.00 A.M. – 5.00 P.M. AREA: MOI’S BRIDGE, MAJI MAZURI NAIROBI COUNTY Masai Lodge Rd, Nazarene Univ, Twala, Olosirikon, Part of Rongai & DATE: Saturday 07.05.2016 TIME: 8.00 A.M.