Direct Tv Tlc Go
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
FY12 Annual Report
PROTECTING OUR LAND FOR future generations Annual Report 2011–2012 From the Chair As Triangle Land Conservancy progressed through our 29th year, we began the twin processes of reflection and assessment which typically accompany preparation for a significant anniversary. We look back with deep gratitude to longtime Triangle residents for their prescient decision nearly 30 years ago to found TLC. Since then, Triangle Land Conservancy has played an important role in blending the growth and vitality of our region with open spaces that provide a variety of benefits for residents and that are readily recognized by those relocating to the area. Today the healthy and vibrant Triangle is consistently voted in national top ten lists for livability and business, as well as being recently acknowledged as top ten in eco- friendliest, healthiest, and cleanest. Part of the Triangle’s success lies in its decision to protect our natural resources—our water and our land. It has not always been easy. The economic crisis of 2008 continues to present chal- lenges in the conservation funding landscape. However, TLC’s decision a few years ago to change the way we work, moving away from the concept of protecting our resources from something, to protecting our resources for something—safeguard- ing clean water, preserving wildlife habitat, keeping local farms and food in our community, and providing places for people to connect with nature—has allowed us to maximize every dollar raised, develop innovative community partnerships and connect with new people. The powerful results of this decision were on full display in 2011–2012. -

Table of Contents WARNING Before Playing This Game, Read the Xbox 360® Console and Xbox 360 Controller
Table of ConTenTs WARNING Before playing this game, read the Xbox 360® console and xbox 360 controller ............................................ 2 accessory manuals for important safety and health information. Keep all manuals for future reference. For replacement console and accessory manuals, go to xbox live ..................................................................... 2 www.xbox.com/support. introduction ............................................................ 3 controls—neW! ....................................................... 3 the Game screen .................................................... 16 Important Health Warning About Playing Video Games superstar selection ............................................ 16 Photosensitive seizures A very small percentage of people may experience a seizure when exposed to main menu ..................................................................17 certain visual images, including flashing lights or patterns that may appear in video games. Even people who have no history of seizures or epilepsy may have WWe universe ..........................................................17 an undiagnosed condition that can cause these “photosensitive epileptic seizures” while watching video games. limb tarGet system—neW! .................................. 19 These seizures may have a variety of symptoms, including lightheadedness, altered extreme rules controls .....................................21 vision, eye or face twitching, jerking or shaking of arms or legs, disorientation, confusion, -

Cablefax Dailytm Friday — February 14, 2014 What the Industry Reads First Volume 25 / No
www.cablefax.com, Published by Access Intelligence, LLC, Tel: 301-354-2101 5 Pages Today CableFAX DailyTM Friday — February 14, 2014 What the Industry Reads First Volume 25 / No. 031 Next Step: Comcast Must Convince Regulators, Consumers It’s a White Knight A lot is being made about whether the $45bln proposed Comcast-Time Warner Cable combo will pass regulatory muster, but it’s fair to ask whether it will pass consumer scrutiny. Regulatory bodies always look at mergers in the context of the public interest, but the public might be more interested in this deal than previous Comcast transac- tions. Sure, there were concerns raised when Comcast acquired NBCU in ’11, but the programmer didn’t have a direct link to consumers the way TWC does. And it’s not like these are beloved companies—they rank at the bot- tom of the American Customer Satisfaction Index for the subscription TV industry. An L.A. Times story on the deal Thurs was headlined, “How a cable monopoly can get even worse for you.” Comcast and TWC don’t see it that way, repeatedly referring to the deal Thurs as “pro-consumer” and saying it won’t reduce competition because the 2 don’t overlap in any market. “Once you take a breath and think it through analytically and get past some of the hysteria,” you find substantial public interest benefits, Comcast evp David Cohen told reporters. Sen Judiciary Antitrust subc- mte chair Amy Klobuchar (D-MN) and ranking member Mike Lee (R-UT) already have promised to hold a hearing. -

Liberty Global and Discovery Communications Renew Long-Term, Comprehensive Distribution Partnership
Liberty Global and Discovery Communications Renew Long-Term, Comprehensive Distribution Partnership Multiplatform agreement spans 12 markets in Europe and entire portfolio of Discovery and Eurosport Networks, including first-time ever full and unique coverage of Olympic Games beginning in 2018 London, United Kingdom – August 2, 2016: Liberty Global and Discovery Communications today announce a long-term, comprehensive renewal of their distribution agreement that guarantees delivery of Discovery’s full portfolio of fan-favorite networks, including flagships Discovery Channel, TLC, ID and Eurosport, to Liberty Global customers across its 12 European countries: Austria, Belgium, Czech Republic, Germany, Hungary, Ireland, Poland, Romania, Netherlands, Slovakia, Switzerland and the United Kingdom. The deal also includes digital rights, ensuring passionate fans can access their favorite networks and shows on multiple screens, in and out of the home, through Liberty Global’s broadband companies, which include UPC, Virgin Media, Ziggo, Telenet and Unitymedia. “Discovery is the leader in premium and provocative real-world entertainment through our loved brands that engage and entertain passionate communities across the globe. From world-class sporting events like the Olympic Games, Grand Slam Tennis, and important local sports to globally popular shows like GOLD RUSH, CAKE BOSS, and SHARK WEEK, this new deal strengthens our great partnership with Liberty Global and provides their customers with more premium content from Discovery’s networks and brands, across more screens than ever before,” said JB Perrette, President and CEO, Discovery Networks International. Bruce Mann, Managing Director, Programming, Liberty Global, added: “This long-term renewal provides Liberty Global with guaranteed access to Discovery’s broad stable of world-famous brands. -

Discovery Communications to Acquire Scripps Networks Interactive for $14.6 Billion
Discovery communications to acquire Scripps Networks Interactive for $14.6 Billion July 31, 2017 Combination to Accelerate Growth Across Linear, Digital and Short-Form Platforms Around the World and Create a Global Leader in Real Life Entertainment Combined company will have nearly 20% of ad-supported pay-TV viewership in the U.S. Becomes home to five of the top female networks in ad-supported pay-TV with over 20% share of women watching primetime in the U.S. Optionality for next generation growth opportunities through exploitation of brands, formats, talent and 8,000 hours of original programming annually Over 7 billion monthly streams creates leading short-form, mobile-first digital player Significant cost synergies estimated at approximately $350 million Expected to be accretive to Adjusted Earnings per Share and Free Cash Flow in first year after close Investor call scheduled for Monday, July 31, at 8:00 a.m. Eastern Time (ET) Silver Spring, Md. and Knoxville, Tenn. - Discovery Communications, Inc. (Nasdaq: DISCA, DISCB, DISCK) (“Discovery”) and Scripps Networks Interactive, Inc. (Nasdaq: SNI) (“Scripps”) today announced that they have signed a definitive agreement for Discovery to acquire Scripps in a cash-and-stock transaction valued at $14.6 billion, or $90 per share, based on Discovery’s Friday, July 21 closing price. The purchase price represents a premium of 34% to Scripps’ unaffected share price as of Tuesday, July 18, 2017. The transaction is expected to close by early 2018. “This is an exciting new chapter for Discovery. Scripps is one of the best run media companies in the world with terrific assets, strong brands and popular talent and formats. -

FY20 Superintendent's Proposed Budget
Manassas Park City Schools FY2020 Superintendent’s Proposed Budget 1 Park Center Court, Suite A, Manassas Park, VA 20111 www.mpark.net This page is intentionally blank i Table of Contents Guide to Understanding the Budget iv Budget Types iv Document Organization iv Acknowledgements v Executive Team v School Board v Awards vi Organizational Section 1 Manassas Park City Schools Overview 5 The City of Manassas Park 5 Governance 7 Division Organization 7 Strategic Plan 13 Mission 13 Vision 13 Beliefs 13 Goals and Objectives 13 Budget Development Process 17 Statutory Guidelines 17 Budget Development 17 Budget Calendar 18 Key Budget Drivers 19 Revenue Forecasting 22 Expenditure Forecasting 23 Financial Section 27 All Funds Summary 29 Statement of Revenues and Expenditures 29 Revenues 30 Expenditures 30 Classification Structure 31 Fund Descriptions 33 Federal Fund 35 Statement of Revenues and Expenditures 35 Revenues 35 Expenditures 36 Fund Balance 36 General Fund 37 Statement of Revenues and Expenditures 37 Revenues 37 Expenditures 38 Fund Balances 38 Major Shifts 38 Instructional Program Summary 39 Virginia Preschool Initiative Program 39 ii Head Start Program 41 Early Childhood Special Education Program 42 Cougar Elementary School 44 Manassas Park Elementary School 48 Manassas Park Middle School 52 Manassas Park High School 56 Office of Instruction 60 Special Programs Department 64 Assessment and Accountability Department 70 Division-wide Support 72 School Board 72 Office of the Superintendent 74 Office of the Deputy Superintendent 77 Finance -

THQ Online Manual
INSTRUCTION BOOKLET LIMITED WARRANTY THQ (UK) LIMITED warrants to the original purchaser of this THQ (UK) LIMITED product that the medium on which the computer program is recorded is free from defects in materials and workmanship for a period of ninety (90) days from the date of purchase. This THQ (UK) LIMITED software is sold ”as is“, without express or implied warranty of any kind resulting from use of this program. THQ (UK) LIMITED agrees for a period of ninety (90) days to either repair or replace, at its option, free of charge, any THQ (UK) LIMITED product, postage paid, with proof of purchase, at its Customer Service centre. Replacement of this Game Disc, free of charge to the original purchaser is the full extent of our liability. Please mail to THQ (UK) LIMITED, Ground Floor; Block A, Dukes Court, Duke Street, Woking, Surrey, GU21 5BH. Please allow 28 days from dispatch for return of your Game Disc. This warranty is not applicable to normal wear and tear. This warranty shall not be applicable and shall be void if the defect in the THQ (UK) LIMITED product has arisen through abuse, unreasonable use, mistreatment or neglect. THIS WARRANTY IS IN LIEU OF ALL OTHER WARRANTIES AND NO OTHER REPRESENTATIONS OR CLAIMS OF ANY NATURE SHALL BE BINDING OR OBLIGATE THQ (UK) LIMITED. ANY IMPLIED WARRANTIES OF APPLICABILITY TO THIS SOFTWARE PRODUCT, INCLUDING WARRANTIES OF MERCHANTABILITY AND FITNESS FOR A PARTICULAR PURPOSE, ARE LIMITED TO THE NINETY (90) DAY PERIOD DESCRIBED ABOVE. IN NO EVENT WILL THQ (UK) LIMITED BE LIABLE FOR ANY SPECIAL, INCIDENTAL OR CONSEQUENTIAL DAMAGES RESULTING FROM POSSESSION, USE OR MALFUNCTION OF THIS THQ (UK) LIMITED PRODUCT. -

DOWNLOAD the ARVIG WIFI TV APP Watch on Your TV, Tablet, Computer and Smartphone
Contact: 888.992.7844 | [email protected] 24/7 Support: 877.290.0560 | [email protected] Chat Online: arvig.net | 7 days a week WiFi arvig.net/WiFiTV Delivered by Arvig® DOWNLOAD THE ARVIG WIFI TV APP Watch on your TV, tablet, computer and smartphone. Available in Google Play and App Store. MORE WAYS TO VIEW PERSONALIZED CLOUD DVR Works with your favorite It learns what you love and No more bulky boxes or wires. streaming devices; Amazon Fire TV, keeps those series and movies Access your recordings on Apple TV and more. front and center. virtually any device.* IT’S ALL HD REPLAY TV WATCH TV EVERYWHERE Auto detection gives Never miss another show. Watch up to the Anytime, anywhere! you the best TV past 72 hours of shows, movies, and sports Stream on almost view available. across most of our channel lineup.* any device.* Rochester Locals WiFi WIFI TV PLANS Delivered by Arvig® Essential Premium Packages Purchase á la Carte with Choice and 3 KIMT - CBS Rochester 7 The CW 609 This TV Complete WiFi Plans 4 KYIN - PBS Rochester 11 KTTC - NBC Rochester 5 KSMQ - PBS Rochester 12 KXLT - FOX Rochester HBO-Cinemax 6 KAAL - ABC Rochester 300 HBO 311 MoreMAX 301 HBO 2 312 MAX Latino 302 HBO Signature 313 5StarMAX 303 HBO Family 314 ThrillerMAX Choice Includes Essential Channels 304 HBO Comedy 315 MovieMAX 15 WGN - Chicago 47 CNN Headline News 81 HGTV 305 HBO Zone 316 OuterMAX 24 Lifetime 48 CNBC 83 Food Network 310 Cinemax 317 ActionMAX 25 USA Network 49 truTV 84 Travel Channel 26 TNT 50 Freeform 90 Bravo Showtime-TMC 27 TBS 53 Universal Kids 91 A&E -

Ta»!^Vw0,Rxded G
THREE CENTS. Vou Lill....N°-17,193. NEW-YORK, MONDAY, DECEMBER ll, 1893.-TEB PAGES PRICE demandI an extra credit to reinforce the Wi re given that the military and police patrols in WILL Hi: RIQHT-A BOtiT PACE! GRESHAM AND THURSTON, THE BOMB-THROWER FOUND. police Barcelona be Increased f..r the purpose of de MRS. rOY'S NARRATIVE while they ars repre_rtng the Anarchists. oin Anarchists snd revolutionaries of all kinds, whether seton or theorist1*. G,:TT1N:; m **"* here and the IrV Rome, Dec. IB.The sewapspers MAY THIS TIME REVERSE PLAIN WORDS TO THE FORMER. M. DUPUVSDEATH JUS OBJECT Ta»!^vW0,rXDEDOf those wh. W(.,,. v.,.lr(1.(1 in ,h,. rham. publi generally strongly den >.'in.-e the Anarchist THI HEW LYU-KN E AGAB9T DAKIEL THE PRESIDENT ber were to Dieu. outrage in the Er.-nch Chamber. Deputy RsmpoldL yesterday removed the HOtel It.eHeal, has fives notice lu the Italian Chamber of OM'.HUN. HU :>\V.V POLICY. IJ.- gravest case was that of Oulllotler. whose Deputies that at the n»-xt sitting he will mn*" a WHAT OCCUUKED AT THE INTERVIEWS IN THE HAVOC HF- WROUGHT IN ttWl was fractured. The vote ot sympathy with the French Chamber. The GLORYING skull was success- Anarchists comment on thc with here Furls outrage rf, ** N >w i-i.;: TBE GOVESE- TUE TWO. THE FRENCH CHAMBER. fully trepanned this morning by Dr. Deja rs. undisguised gie-. MISMNf* LINKS IN TRI*. CHAIN THAT COMPLETE*-. SAID to CtSIOt BETWEEN and PA UT unless complications set in the patient will ANARCHIST PRINTS. -
IV Line Maintenance Orders(Central and Peripheral)
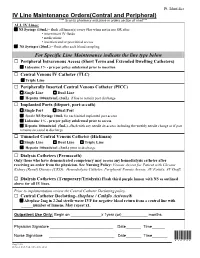
Pt. Identifier IV Line Maintenance Orders(Central and Peripheral) **** Scan to pharmacy and place in orders section of chart*** ALL IV Lines: NS Syringe (10mL)– flush all lumen(s) every 8hrs when not in use OR after: intermittent IV fluids medications insertion and/or post initial access NS Syringes (20mL) – flush after each blood sampling For Specific Line Maintenance indicate the line type below Peripheral Intravenous Access (Short Term and Extended Dwelling Catheters) Lidocaine 1% - prn per policy subdermal prior to insertion Central Venous IV Catheter (TLC) Triple Line Peripherally Inserted Central Venous Catheter (PICC) Single Line Dual Line Heparin 100units/mL (3mL) if line to remain post discharge Implanted Ports (lifeport, port-a-cath) Single Port Dual Port Sterile NS Syringe 10mL for each initial implanted port access Lidocaine 1% - prn per policy subdermal prior to access Heparin 100units/ml (5mL) –flush with any needle de-access including the weekly needle change or if port remains accessed at discharge Tunneled Central Venous Catheter (Hickman) Single Line Dual Line Triple Line Heparin 100units/mL (3mL) prior to discharge Dialysis Catheters (Permacath) Only those who have demonstrated competency may access any hemodialysis catheter after receiving an order from the physician. See Nursing Policy: Venous Access for Patient with Chronic Kidney (Renal) Disease (CKD): Hemodialysis Catheter, Peripheral Venous Access, AV Fistula, AV Graft, Dialysis Catheters (Temporary/Trialysis) Flush third purple lumen with NS as outlined above for all IV lines. Prior to implementation review the Central Catheter Declotting policy. Central Catheter Declotting-Alteplase / Cathflo Activase® Alteplase 2mg in 2.2ml sterile water IVP for negative blood return from a central line with ______number of lumens, May repeat x1. -

Xfinity Channel Lineup
Channel Lineup 1-800-XFINITY | xfinity.com SARASOTA, MANATEE, VENICE, VENICE SOUTH, AND NORTH PORT Legend Effective: April 1, 2016 LIMITED BASIC 26 A&E 172 UP 183 QUBO 738 SPORTSMAN CHANNEL 1 includes Music Choice 27 HLN 179 GSN 239 JLTV 739 NHL NETWORK 2 ION (WXPX) 29 ESPN 244 INSP 242 TBN 741 NFL REDZONE <2> 3 PBS (WEDU SARASOTA & VENICE) 30 ESPN2 42 BLOOMBERG 245 PIVOT 742 BTN 208 LIVE WELL (WSNN) 31 THE WEATHER CHANNEL 719 HALLMARK MOVIES & MYSTERIES 246 BABYFIRST TV AMERICAS 744 ESPNU 5 HALLMARK CHANNEL 32 CNN 728 FXX (ENGLISH) 746 MAV TV 6 SUNCOAST NEWS (WSNN) 33 MTV 745 SEC NETWORK 247 THE WORD NETWORK 747 WFN 7 ABC (WWSB) 34 USA 768-769 SEC NETWORK (OVERFLOW) 248 DAYSTAR 762 CSN - CHICAGO 8 NBC (WFLA) 35 BET 249 JUCE 764 PAC 12 9 THE CW (WTOG) 36 LIFETIME DIGITAL PREFERRED 250 SMILE OF A CHILD 765 CSN - NEW ENGLAND 10 CBS (WTSP) 37 FOOD NETWORK 1 includes Digital Starter 255 OVATION 766 ESPN GOAL LINE <14> 11 MY NETWORK TV (WTTA) 38 FOX SPORTS SUN 57 SPIKE 257 RLTV 785 SNY 12 IND (WMOR) 39 CNBC 95 POP 261 FAMILYNET 47, 146 CMT 13 FOX (WTVT) 40 DISCOVERY CHANNEL 101 WEATHERSCAN 271 NASA TV 14 QVC 41 HGTV 102, 722 ESPNEWS 279 MLB NETWORK MUSIC CHOICE <3> 15 UNIVISION (WVEA) 44 ANIMAL PLANET 108 NAT GEO WILD 281 FX MOVIE CHANNEL 801-850 MUSIC CHOICE 17 PBS (WEDU VENICE SOUTH) 45 TLC 110 SCIENCE 613 GALAVISION 17 ABC (WFTS SARASOTA) 46 E! 112 AMERICAN HEROES 636 NBC UNIVERSO ON DEMAND TUNE-INS 18 C-SPAN 48 FOX SPORTS ONE 113 DESTINATION AMERICA 667 UNIVISION DEPORTES <5> 19 LOCAL GOVT (SARASOTA VENICE & 49 GOLF CHANNEL 121 DIY NETWORK 721 TV GAMES 1 includes Limited Basic VENICE SOUTH) 50 VH1 122 COOKING CHANNEL 734 NBA TV 1, 199 ON DEMAND (MAIN MENU) 19 LOCAL EDUCATION (MANATEE) 51 FX 127 SMITHSONIAN CHANNEL 735 CBS SPORTS NETWORK 194 MOVIES ON DEMAND 20 LOCAL GOVT (MANATEE) 55 FREEFORM 129 NICKTOONS 738 SPORTSMAN CHANNEL 299 FREE MOVIES ON DEMAND 20 LOCAL EDUCATION (SARASOTA, 56 AMC 130 DISCOVERY FAMILY CHANNEL 739 NHL NETWORK 300 HBO ON DEMAND VENICE & VENICE SOUTH) 58 OWN 131 NICK JR. -

Central Venous Catheters Clinical Considerations
Central Venous Catheters Clinical Considerations Igor Voskresensky 8.15.09 CVCs…Necessary Evil TLC Cordis MICU TRIC (triple lumen infusion catheter) Vascular Access Devices I. Nontunneled (TLC, Cordis, MAC, VasCath) ‐ short‐term, drips/meds, HDM/resus, dialysis, plasmapheresis, TPN II. Tunneled (Hickman, Broviac, Groshong) ‐ long‐term, OR, abx, chemo, TPN, pediatric, frequent lab work III. Peripherally inserted (PICC) ‐ long‐term, abx, TPN IV. Implanted ports (percutaneous, cutdown) ‐ long‐term, chemo, periodic transfusions Preparation for Insertion –C5, Do20, Teach100 • KTCLT, live it… • Patient’s anatomy, site selection, ultrasound? • Turn off tube feeds and check labs (plts, ffp?) • Know the process • Get your own things (syringes, flushes, claves) • Set it up, same way every time • Head‐Down‐burg • Pain control • Complications Pearls • Withdraw gently • Hand on the wire • Visualize needle tip with US • Shallow angle, hit the clavicle, arm tug • Poor form is unacceptable • No COW if the ports don’t draw/flush • No femoral access cardiology style • Secure your line with quality • Get a CXR (PTX, HTX, positioning) • If it don’t feel right, it probably ain’t right Complications • Catheter‐related (type, mechanical and antibacterial properties, use) • Patient‐related (anatomy, nature of disease, immunocompromise) • Site‐related (IJ, SC, Fem) • Catheter care (experience of medical and nursing staff, hygiene and care) Inten Car Med 28:1–17 NEJM 348:1123‐1133 Ann Surg 173:184–190 Chest 113:165–171 J Vasc Surg 48: 918‐925 Catheter‐Associated Infections • Colonization (semiquant vs. quant) ‐ 15 CFU agar vs. 1000 CFU broth • Exit‐site infection ‐ erythema, induration tenderness, purulence • CRBSI CRBSI • CVC colonization and peripheral blood cx • 10‐25 % associated mortality, $ • Sick pts, ETT/ICU/TPN, T‐T‐T‐T • SC/IJ vs.