Pakistan: the Faisalabad Obstetric Flying Squad A
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

FIRMS in AOR of RD PUNJAB Ser Name of Firm Chemical RD
Appendix-A FIRMS IN AOR OF RD PUNJAB Ser Name of Firm Chemical RD 1 M/s A.A Textile Processing Industries, Faisalabad Hydrochloric Acid Punjab 2 M/s A.B Exports (Pvt) Ltd, Faisalabad Hydrochloric Acid Punjab 3 M/s A.M Associates, Lahore Hydrochloric Acid Punjab 4 M/s A.M Knit Wear, Faisalabad Hydrochloric Acid Punjab 5 M/s A.S Chemical, Multan Hydrochloric Acid Punjab 6 M/s A.T Impex, Lahore Hydrochloric Acid Punjab 7 M/s AA Brothers Chemical Traders, Sialkot Hydrochloric Acid Punjab 8 M/s AA Fabrics, Faisalabad Hydrochloric Acid Punjab 9 M/s AA Spinning Mills Ltd, Faisalabad Hydrochloric Acid Punjab 10 M/s Aala Production Industries (Pvt) Ltd, Faisalabad Hydrochloric Acid Punjab 11 M/s Aamir Chemical Store, Multan Hydrochloric Acid Punjab 12 M/s Abbas Chemicals, Lahore Hydrochloric Acid Punjab M/s Abdul Razaq & Sons Tezab and Spray Centre, 13 Hydrochloric Acid Punjab Toba Tek Singh 14 M/s Abubakar Anees Textiles, Faisalabad Hydrochloric Acid Punjab 15 M/s Acro Chemicals, Lahore Toluene & MEK Punjab 16 M/s Agritech Ltd, Lahore Hydrochloric Acid Punjab 17 M/s Ahmad Chemical Traders, Muridke Hydrochloric Acid Punjab 18 M/s Ahmad Chemmicals, Lahore Hydrochloric Acid Punjab 19 M/s Ahmad Industries (Pvt) Ltd, Khanewal Hydrochloric Acid Punjab 20 M/s Ahmed Chemical Traders, Faisalabad Hydrochloric Acid Punjab 21 M/s AHN Steel, Lahore Hydrochloric Acid Punjab 22 M/s Ajmal Industries, Kamoke Hydrochloric Acid Punjab 23 M/s Ajmer Engineering Electric Works, Lahore Hydrochloric Acid Punjab Hydrochloric Acid & Sulphuric 24 M/s Akbari Chemical Company, -

S# BRANCH CODE BRANCH NAME CITY ADDRESS 1 24 Abbottabad
BRANCH S# BRANCH NAME CITY ADDRESS CODE 1 24 Abbottabad Abbottabad Mansera Road Abbottabad 2 312 Sarwar Mall Abbottabad Sarwar Mall, Mansehra Road Abbottabad 3 345 Jinnahabad Abbottabad PMA Link Road, Jinnahabad Abbottabad 4 131 Kamra Attock Cantonment Board Mini Plaza G. T. Road Kamra. 5 197 Attock City Branch Attock Ahmad Plaza Opposite Railway Park Pleader Lane Attock City 6 25 Bahawalpur Bahawalpur 1 - Noor Mahal Road Bahawalpur 7 261 Bahawalpur Cantt Bahawalpur Al-Mohafiz Shopping Complex, Pelican Road, Opposite CMH, Bahawalpur Cantt 8 251 Bhakkar Bhakkar Al-Qaim Plaza, Chisti Chowk, Jhang Road, Bhakkar 9 161 D.G Khan Dera Ghazi Khan Jampur Road Dera Ghazi Khan 10 69 D.I.Khan Dera Ismail Khan Kaif Gulbahar Building A. Q. Khan. Chowk Circular Road D. I. Khan 11 9 Faisalabad Main Faisalabad Mezan Executive Tower 4 Liaqat Road Faisalabad 12 50 Peoples Colony Faisalabad Peoples Colony Faisalabad 13 142 Satyana Road Faisalabad 585-I Block B People's Colony #1 Satayana Road Faisalabad 14 244 Susan Road Faisalabad Plot # 291, East Susan Road, Faisalabad 15 241 Ghari Habibullah Ghari Habibullah Kashmir Road, Ghari Habibullah, Tehsil Balakot, District Mansehra 16 12 G.T. Road Gujranwala Opposite General Bus Stand G.T. Road Gujranwala 17 172 Gujranwala Cantt Gujranwala Kent Plaza Quide-e-Azam Avenue Gujranwala Cantt. 18 123 Kharian Gujrat Raza Building Main G.T. Road Kharian 19 125 Haripur Haripur G. T. Road Shahrah-e-Hazara Haripur 20 344 Hassan abdal Hassan Abdal Near Lari Adda, Hassanabdal, District Attock 21 216 Hattar Hattar -

Capturing the Demographic Dividend in Pakistan
CAPTURING THE DEMOGRAPHIC DIVIDEND IN PAKISTAN ZEBA A. SATHAR RABBI ROYAN JOHN BONGAARTS EDITORS WITH A FOREWORD BY DAVID E. BLOOM The Population Council confronts critical health and development issues—from stopping the spread of HIV to improving reproductive health and ensuring that young people lead full and productive lives. Through biomedical, social science, and public health research in 50 countries, we work with our partners to deliver solutions that lead to more effective policies, programs, and technologies that improve lives around the world. Established in 1952 and headquartered in New York, the Council is a nongovernmental, nonprofit organization governed by an international board of trustees. © 2013 The Population Council, Inc. Population Council One Dag Hammarskjold Plaza New York, NY 10017 USA Population Council House No. 7, Street No. 62 Section F-6/3 Islamabad, Pakistan http://www.popcouncil.org The United Nations Population Fund is an international development agency that promotes the right of every woman, man, and child to enjoy a life of health and equal opportunity. UNFPA supports countries in using population data for policies and programmes to reduce poverty and to ensure that every pregnancy is wanted, every birth is safe, every young person is free of HIV and AIDS, and every girl and woman is treated with dignity and respect. Library of Congress Cataloging-in-Publication Data Capturing the demographic dividend in Pakistan / Zeba Sathar, Rabbi Royan, John Bongaarts, editors. -- First edition. pages ; cm Includes bibliographical references. ISBN 978-0-87834-129-0 (alkaline paper) 1. Pakistan--Population--Economic aspects. 2. Demographic transition--Economic aspects--Pakistan. -

Ethnomedicinal Profile of Flora of District Sialkot, Punjab, Pakistan
ISSN: 2717-8161 RESEARCH ARTICLE New Trend Med Sci 2020; 1(2): 65-83. https://dergipark.org.tr/tr/pub/ntms Ethnomedicinal Profile of Flora of District Sialkot, Punjab, Pakistan Fozia Noreen1*, Mishal Choudri2, Shazia Noureen3, Muhammad Adil4, Madeeha Yaqoob4, Asma Kiran4, Fizza Cheema4, Faiza Sajjad4, Usman Muhaq4 1Department of Chemistry, Faculty of Natural Sciences, University of Sialkot, Punjab, Pakistan 2Department of Statistics, Faculty of Natural Sciences, University of Sialkot, Punjab, Pakistan 3Governament Degree College for Women, Malakwal, District Mandi Bahauddin, Punjab, Pakistan 4Department of Chemistry, Faculty of Natural Sciences, University of Gujrat Sialkot Subcampus, Punjab, Pakistan Article History Abstract: An ethnomedicinal profile of 112 species of remedial Received 30 May 2020 herbs, shrubs, and trees of 61 families with significant Accepted 01 June 2020 Published Online 30 Sep 2020 gastrointestinal, antimicrobial, cardiovascular, herpetological, renal, dermatological, hormonal, analgesic and antipyretic applications *Corresponding Author have been explored systematically by circulating semi-structured Fozia Noreen and unstructured questionnaires and open ended interviews from 40- Department of Chemistry, Faculty of Natural Sciences, 74 years old mature local medicine men having considerable University of Sialkot, professional experience of 10-50 years in all the four geographically Punjab, Pakistan diversified subdivisions i.e. Sialkot, Daska, Sambrial and Pasrur of E-mail: [email protected] district Sialkot with a total area of 3106 square kilometres with ORCID:http://orcid.org/0000-0001-6096-2568 population density of 1259/km2, in order to unveil botanical flora for world. Family Fabaceae is found to be the most frequent and dominant family of the region. © 2020 NTMS. -

Consolidated List of HBL and Bank Alfalah Branches for Ehsaas Emergency Cash Payments
Consolidated list of HBL and Bank Alfalah Branches for Ehsaas Emergency Cash Payments List of HBL Branches for payments in Punjab, Sindh and Balochistan ranch Cod Branch Name Branch Address Cluster District Tehsil 0662 ATTOCK-CITY 22 & 23 A-BLOCK CHOWK BAZAR ATTOCK CITY Cluster-2 ATTOCK ATTOCK BADIN-QUAID-I-AZAM PLOT NO. A-121 & 122 QUAID-E-AZAM ROAD, FRUIT 1261 ROAD CHOWK, BADIN, DISTT. BADIN Cluster-3 Badin Badin PLOT #.508, SHAHI BAZAR TANDO GHULAM ALI TEHSIL TANDO GHULAM ALI 1661 MALTI, DISTT BADIN Cluster-3 Badin Badin PLOT #.508, SHAHI BAZAR TANDO GHULAM ALI TEHSIL MALTI, 1661 TANDO GHULAM ALI Cluster-3 Badin Badin DISTT BADIN CHISHTIAN-GHALLA SHOP NO. 38/B, KHEWAT NO. 165/165, KHATOONI NO. 115, MANDI VILLAGE & TEHSIL CHISHTIAN, DISTRICT BAHAWALNAGAR. 0105 Cluster-2 BAHAWAL NAGAR BAHAWAL NAGAR KHEWAT,NO.6-KHATOONI NO.40/41-DUNGA BONGA DONGA BONGA HIGHWAY ROAD DISTT.BWN 1626 Cluster-2 BAHAWAL NAGAR BAHAWAL NAGAR BAHAWAL NAGAR-TEHSIL 0677 442-Chowk Rafique shah TEHSIL BAZAR BAHAWALNAGAR Cluster-2 BAHAWAL NAGAR BAHAWAL NAGAR BAZAR BAHAWALPUR-GHALLA HOUSE # B-1, MODEL TOWN-B, GHALLA MANDI, TEHSIL & 0870 MANDI DISTRICT BAHAWALPUR. Cluster-2 BAHAWALPUR BAHAWALPUR Khewat #33 Khatooni #133 Hasilpur Road, opposite Bus KHAIRPUR TAMEWALI 1379 Stand, Khairpur Tamewali Distt Bahawalpur Cluster-2 BAHAWALPUR BAHAWALPUR KHEWAT 12, KHATOONI 31-23/21, CHAK NO.56/DB YAZMAN YAZMAN-MAIN BRANCH 0468 DISTT. BAHAWALPUR. Cluster-2 BAHAWALPUR BAHAWALPUR BAHAWALPUR-SATELLITE Plot # 55/C Mouza Hamiaytian taxation # VIII-790 Satellite Town 1172 Cluster-2 BAHAWALPUR BAHAWALPUR TOWN Bahawalpur 0297 HAIDERABAD THALL VILL: & P.O.HAIDERABAD THAL-K/5950 BHAKKAR Cluster-2 BHAKKAR BHAKKAR KHASRA # 1113/187, KHEWAT # 159-2, KHATOONI # 503, DARYA KHAN HASHMI CHOWK, POST OFFICE, TEHSIL DARYA KHAN, 1326 DISTRICT BHAKKAR. -
Fundfor Sustainable Development (FSD) in North West Frontier Province (NWFP) by Mohammad Rafiq
Profiles ofthe NEFS: North West Frontier Province, Pakistan 103 Fundfor Sustainable Development (FSD) in North West Frontier Province (NWFP) by Mohammad Rafiq I. History alleviation and job creation. In the process, FSD hopes to address the issues of recurring costs, Following on the Pakistan National inefficiency, and governance associated with the Conservation Strategy (NCS), over the past state-delivered development. three years, the Government of NWFP has developed the Sarhad Provincial Conservation There is substantial political and Strategy (SPCS), “Sarhad” being the vernacular bureaucratic support for the fund. However, term for “Frontier.” Extensive public objections by the Finance Department are consultation was an important part of the delaying its establishment. process. A draft SPCS has been approved by the Provincial Cabinet. II. Goals The idea of a Fund for Sustainable The main purpose of FSD is to protect Development (FSD) in NWFP was conceived by the environment by encouraging sustainability in the IUCN-SPCS team working with the the use of natural resources of the province. Government of NWFP in the development of the The specific objectives are: SPCS. The Chief Minister then supported a “Policy for the Grant of Concessions of Mining > Investment in environmental rehabilitation, of Limestone in NWFP” and the SPCS resource conservation, and sustainable document’s recommendation for the development in a flexible, transparent, development of a fund. efficient and responsible manner; The main motivation for the fund was to: > Engendering public/private partnerships; and > Institute an innovative and flexible > Facilitating community participation in mechanism of financing environmental maintaining a healthy and productive improvements; environment. Enable and maintain partnerships between The fund has not done any strategic the public, private and independent sectors planning as yet, but plans to upon establishment. -
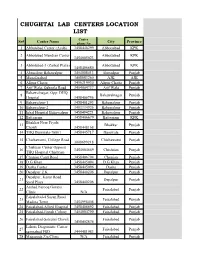
Chughtai Lab Centers Location List
CHUGHTAI LAB CENTERS LOCATION LIST Center Sr# Center Name City Province phone No 1 Abbotabad Center (Ayub) 3458448299 Abbottabad KPK 2 Abbotabad Mandian Center Abbottabad KPK 3454005023 3 Abbotabad-3 (Zarbat Plaza) Abbottabad KPK 3458406680 4 Ahmedpur Bahawalpur 3454008413 Ahmedpur Punjab 5 Muzafarabad 3408883260 AJK AJK 6 Alipur Chatta 3456219930 Alipur Chatta Punjab 7 Arif Wala, Qaboola Road 3454004737 Arif Wala Punjab Bahawalnagar, Opp: DHQ 8 Bahawalnagar Punjab Hospital 3458406756 9 Bahawalpur-1 3458401293 Bahawalpur Punjab 10 Bahawalpur-2 3403334926 Bahawalpur Punjab 11 Iqbal Hospital Bahawalpur 3458494221 Bahawalpur Punjab 12 Battgaram 3458406679 Battgaram KPK Bhakhar Near Piyala 13 Bhakkar Punjab Chowk 3458448168 14 THQ Burewala-76001 3458445717 Burewala Punjab 15 Chichawatni, College Road Chichawatni Punjab 3008699218 Chishtian Center Opposit 16 3454004669 Chishtian Punjab THQ Hospital Chishtian 17 Chunian Cantt Road 3458406794 Chunian Punjab 18 D.G Khan 3458445094 D.G Khan Punjab 19 Daska Center 3458445096 Daska Punjab 20 Depalpur Z.K 3458440206 Depalpur Punjab Depalpur, Kasur Road 21 Depalpur Punjab Syed Plaza 3458440206 Arshad Farooq Goraya 22 Faisalabad Punjab Clinic N/A Faisalabad-4 Susan Road 23 Faisalabad Punjab Madina Town 3454998408 24 Faisalabad-Allied Hospital 3458406692 Faisalabad Punjab 25 Faisalabad-Jinnah Colony 3454004790 Faisalabad Punjab 26 Faisalabad-Saleemi Chowk Faisalabad Punjab 3458402874 Lahore Diagonistic Center 27 Faisalabad Punjab samnabad FSD 3444481983 28 Maqsooda Zia Clinic N/A Faisalabad Punjab Farooqabad, -

Catalogue of Pakistani Vegetables and Fruits
CATALOGUE OF PAKISTANI VEGETABLES AND FRUITS © 2019 The Employers’ Federation of Pakistan (EFP) Head Office, 2nd Floor, State Life Building No. 2, Wallace Road, off I.I Chundrigar Road Karachi, 74000 Telephone: (+92)-21-32439347 Website: www.efp.org.pk The work produced is a product of Economic Council Secretariat and fully reflects the views of stakeholders and association of chambers and industries of the federation. Legal Rights The EC Secretariat has no objection to dissemination of information contained in this document for commercial or academic purposes as long as full reference is provided. All queries concerning legalities should be forwarded to the EC Secretariat, 10 Banglalore Town, Shahra-e-Faisal, Karachi, Pakistan; fax: (+92)-21-34310037; email: [email protected]. 2 Project BreXport Authorized by: Ismail Suttar, Chairman Asif Aziz Zuberi, Co-Chairman Authored by: Abdullah Ali Khan, Coordinator Muhammad Junaid Hanif, Industrial Research Analyst Research & Development, EFP-EC 3 TABLE OF CONTENTS EMPLOYERS’ FEDERATION OF PAKISTAN – ECONOMIC COUNCIL ............................................................ i PREFACE ....................................................................................................................................................................... ii PAKISTAN – UK TRADE: HS CODES ...................................................................................................................... iii DESCRIPTION OF VEGETABLES INCLUDED ...................................................................................................... -

Curriculum Vitae
………………………….. Curriculum Vitae Name : Dr.Muhammad Tahir Nawaz E-mail: [email protected] [email protected] Distinctions Relevant Clusters CLUSTER CODE STATUS Management MM YES Engineering Management EM YES Project Management PM YES Human Resource Management HRM YES Technology Management TM YES Industrial Engineering and YES Management IEM Manufacturing Management MFM YES Telecom Management TEM NO Software Management SM NO Construction Management CM NO Quality Management QM YES Publications and Research Experience o National Publications (Conference): S.N PUBLICATI TITLE OF PAPER COMPLETE NAME HEC VOL NO. ISSUE NO. PAGE NO. O. ON DATE OF THE JOURNAL & CATEGORY FROM TO ADDRESS (W,X,Y,Z) / IMPACT FACTOR 1 JULY 2007 COMPETITVE STUDY ANNALS OF PUNJAB X 1 2 26 31 OF SOME MEDICAL COLLEGE, INTERESTING DATA FAISALABAD, OF MENTALLY PAKISTAN RETARTED CHILDRED FROM FAISALABAD & ISLAMABAD AND ITS MANAGEMENT 2 JUNE 2010 ROLE OF FEMALE PAKISTAN JOURNAL X 1 (PJS-09-1212) - - EMPLYEES IN OF SCIENCE, FIRST APPAREL INDUSTRY FLOOR, SHADMAN OF PAKISTAN PLAZA, SHADMAN MARKET LAHORE, PAKISTAN 3 NOV 2010 MEASURING FEMALE PAKISTAN JOURNAL X II PJS-09-1215 - - EMPLOYEE’S OF SCIENCE, FIRST EMPOWERMENT IN FLOOR, SHADMAN APPAREL INDUSTRY PLAZA, SHADMAN OF PAKISTAN MARKET, LAHORE PAKISTAN o International Publications (Conferences): PAPER TITLE: Topic: Auth: o Journal Publications: PAPER TITLE: Global Journals INC.(US) Topic: Globalization and right adoption of technology in Pakistan Auth: GJCST Volume 13, Issue 1, version 1.0 Jan 15 o Research Papers -
Expanding Pakistan's Exports Through the Generalized System of Preferences (GSP) Program
Expanding Pakistan's Exports through the Generalized System of Preferences (GSP) Program Bill Jackson Office of the U.S. Trade Representative Executive Office of the President June 2016 1 Presentation Summary Overview of the U.S. GSP Program Pakistan’s GSP exports to the U.S. How to increase Pakistan’s use of duty-free opportunities 2 GSP Program Enhanced access to U.S. market Expanded choices for U.S. industries & consumers Provides duty-free treatment for about 3,500 products from Pakistan and 121 other countries $17.4 billion in total U.S. GSP imports (2015) GSP program authorized through December 2017 3 GSP Program: Eligible Products Eligible Ineligible Many manufactured items & inputs Most textiles & apparel Jewelry Watches Many agricultural Footwear products Some gloves & leather Chemicals goods Minerals Marble Carpets 4 How many products are eligible for GSP duty-free treatment? Dutiable imports, 1,868, 17% MFN duty‐free products, 3,868, 36% GSP‐eligible imports (LDCs), 1,464, 14% GSP‐eligible imports (all), 3,511, 33% 5 U.S. and Pakistan Trade in 2015 U.S. imports from Pakistan: $3.7 billion GSP imports: $179 million (5% of total imports) Overall GSP utilization rate: 88% 6 Top GSP imports from Pakistan in 2015 GSP tariff Total GSP HTS chapter & Product description advantage Value 17 –Sugars & sugar confectionery Up to 5.6% $30.8 m 39 – Plastics in primary forms & semi‐ Up to 6.5% $26.8 m finished & finished products 71 –Precious and semiprecious jewelry Up to 11% $16.0 m 82 – Tools & cutlery made of base metals Up to 19% $15.1 m 63 – Textile articles, used textiles, & rags Up to 5.8% $14.3 m 09 –Spices Up to 6.4% $11.0 m 7 How to Qualify for Duty-Free Treatment under GSP Must be a GSP-eligible product Must be a product or growth of Pakistan or of SAARC If using non-Pakistani or non-SAARC inputs, local content & processing must be ≥ 35% of the value Must import directly into the U.S. -

Reclaiming Prosperity in Khyber- Pakhtunkhwa
Working paper Reclaiming Prosperity in Khyber- Pakhtunkhwa A Medium Term Strategy for Inclusive Growth Full Report April 2015 When citing this paper, please use the title and the following reference number: F-37109-PAK-1 Reclaiming Prosperity in Khyber-Pakhtunkhwa A Medium Term Strategy for Inclusive Growth International Growth Centre, Pakistan Program The International Growth Centre (IGC) aims to promote sustainable growth in developing countries by providing demand-led policy advice informed by frontier research. Based at the London School of Economics and in partnership with Oxford University, the IGC is initiated and funded by DFID. The IGC has 15 country programs. This report has been prepared under the overall supervision of the management team of the IGC Pakistan program: Ijaz Nabi (Country Director), Naved Hamid (Resident Director) and Ali Cheema (Lead Academic). The coordinators for the report were Yasir Khan (IGC Country Economist) and Bilal Siddiqi (Stanford). Shaheen Malik estimated the provincial accounts, Sarah Khan (Columbia) edited the report and Khalid Ikram peer reviewed it. The authors include Anjum Nasim (IDEAS, Revenue Mobilization), Osama Siddique (LUMS, Rule of Law), Turab Hussain and Usman Khan (LUMS, Transport, Industry, Construction and Regional Trade), Sarah Saeed (PSDF, Skills Development), Munir Ahmed (Energy and Mining), Arif Nadeem (PAC, Agriculture and Livestock), Ahsan Rana (LUMS, Agriculture and Livestock), Yasir Khan and Hina Shaikh (IGC, Education and Health), Rashid Amjad (Lahore School of Economics, Remittances), GM Arif (PIDE, Remittances), Najm-ul-Sahr Ata-ullah and Ibrahim Murtaza (R. Ali Development Consultants, Urbanization). For further information please contact [email protected] , [email protected] , [email protected] . -
Assessing the 2017 Census of Pakistan Using Demographic Analysis: a Sub-National Perspective
WWW.OEAW.AC.AT VIENNA INSTITUTE OF DEMOGRAPHY WORKING PAPERS 06/2019 ASSESSING THE 2017 CENSUS OF PAKISTAN USING DEMOGRAPHIC ANALYSIS: A SUB-NATIONAL PERSPECTIVE MUHAMMAD ASIF WAZIR AND ANNE GOUJON Vienna Institute of Demography Austrian Academy of Sciences Welthandelsplatz 2, Level 2 | 1020 Wien, Österreich [email protected] | www.oeaw.ac.at/vid DEMOGRAPHY OF INSTITUTE VIENNA – VID Abstract In 2017, Pakistan implemented a long-awaited population census since the last one conducted in 1998. However, several experts are contesting the validity of the census data at the sub-national level, in the absence of a post-enumeration survey. We propose in this paper to use demographic analysis to assess the quality of the 2017 census at the sub- national level, using the 1998 census data and all available intercensal surveys. Applying the cohort-component method of population projection, we subject each six first-level subnational entities for which data are available to estimates regarding the level of fertility, mortality, international, and internal migration. We arrive at similar results as the census at the national level: an estimated 212.4 million compared to 207.7 million counted (2.3% difference). However, we found more variations at the sub-national level. Keywords Census, population projections, reconstruction, Pakistan, Pakistan provinces. Authors Muhammad Asif Wazir (corresponding author), United Nations Population Fund, Islamabad, Pakistan. Email: [email protected] Anne Goujon, Wittgenstein Centre for Demography and Global Human Capital (IIASA, VID/ÖAW, WU), Vienna Institute of Demography, Austrian Academy of Sciences and World Population Program, International Institute for Applied Systems Analysis. Email: [email protected] Acknowledgments This study is based on the publically available data and was not funded.