Ultrastructural Studies in Fetal I-Cell Disease
Total Page:16
File Type:pdf, Size:1020Kb

Load more
Recommended publications
-

Essential Function of the Alveolin Network in the Subpellicular
RESEARCH ARTICLE Essential function of the alveolin network in the subpellicular microtubules and conoid assembly in Toxoplasma gondii Nicolo` Tosetti1, Nicolas Dos Santos Pacheco1, Eloı¨se Bertiaux2, Bohumil Maco1, Lore` ne Bournonville2, Virginie Hamel2, Paul Guichard2, Dominique Soldati-Favre1* 1Department of Microbiology and Molecular Medicine, Faculty of Medicine, University of Geneva, Geneva, Switzerland; 2Department of Cell Biology, Sciences III, University of Geneva, Geneva, Switzerland Abstract The coccidian subgroup of Apicomplexa possesses an apical complex harboring a conoid, made of unique tubulin polymer fibers. This enigmatic organelle extrudes in extracellular invasive parasites and is associated to the apical polar ring (APR). The APR serves as microtubule- organizing center for the 22 subpellicular microtubules (SPMTs) that are linked to a patchwork of flattened vesicles, via an intricate network composed of alveolins. Here, we capitalize on ultrastructure expansion microscopy (U-ExM) to localize the Toxoplasma gondii Apical Cap protein 9 (AC9) and its partner AC10, identified by BioID, to the alveolin network and intercalated between the SPMTs. Parasites conditionally depleted in AC9 or AC10 replicate normally but are defective in microneme secretion and fail to invade and egress from infected cells. Electron microscopy revealed that the mature parasite mutants are conoidless, while U-ExM highlighted the disorganization of the SPMTs which likely results in the catastrophic loss of APR and conoid. Introduction *For correspondence: Toxoplasma gondii belongs to the phylum of Apicomplexa that groups numerous parasitic protozo- Dominique.Soldati-Favre@unige. ans causing severe diseases in humans and animals. As part of the superphylum of Alveolata, the ch Apicomplexa are characterized by the presence of the alveoli, which consist in small flattened single- membrane sacs, underlying the plasma membrane (PM) to form the inner membrane complex (IMC) Competing interest: See of the parasite. -

A Role for Crinophagy in Pancreatic Islet B-Cells Minireview Based on a Doctoral Thesis
Upsala J Med Sci 92: 99-1 13, 1987 A Role for Crinophagy in Pancreatic Islet B-cells Minireview based on a doctoral thesis Annika Schnell Landstrom Department of Medical Cell Biology, Uppsala University, Uppsala, Sweden INTRODUCTORY REMARKS ON LYSOSOMES The lysosomes were first observed by Christian de Duve and his collaborators in December 1949 as "a cryptic form of latent acid phosphatase" (18). This observation lead to the suggestion that the enzyme could be located in a distinct group of subcellular granules, segregated from the rest of the cell by a limiting membrane. Further studies showed that these granules contained a number of acid hydrolases. The granules or bodies were thus supposed to have lytic properties and they were named lysosomes (18, 19). Soon after the discovery of the lysosome its role in cellular events such as intracellular digestion and phagocytosis was established. The presence of acid hydrolases, primarily acid phosphatase, as evidenced by enzyme cytochemistry, was the main criterium for morphological identification of a lysosome. In 1966 de Duve and Wattiaux (20) suggested a nomenclature for the lysosomal system, based in part on morphological criteria but mainly on the known functions of the lysosomes (Fig. 1). At that time the existence of some of the lysosomal particles was still under debate. The concept of primary lyso- somes, which had not yet taken part in intracellular degradation, was thus proposed. Lysosomes which had been involved in some kind of degradation were named secondary lysosomes. Depending on whether the secondary lysosomes were supposed to have been involved in either autophagy, i.e. -

Lysosomes, Smooth Endoplasmic Reticulum, Mitochondria, And
Undergraduate – Graduate 4. Lysosomes, Smooth Histology Lecture Series Endoplasmic Reticulum, Larry Johnson, Professor Veterinary Integrative Biosciences Mitochondria, and Inclusions Texas A&M University College Station, TX 77843 Objective Lysosomal ultrastructure and function/dysfunction along with continued discussion on protein sorting and protein targeting Smooth endoplasmic reticulum ultrastructure and function in typical cells and those specialized to secrete steroids Mitochondrial ultrastructure, function, origin, and incorporation of cytoplasmic proteins Inclusions Ribosomes translate mRNA in the production of protein. SER Reactions • Scaler reactions Cytosolic proteins a + b = c • Vectorial reactions a + b = c membranes RER proteins • Cytosol is the part of the cytoplasm that is not held by any of the organelles in the cell. On the other hand, cytoplasm is the part of the cell which is contained within the entire cell membrane. • Cytoplasm is cytosol plus organelles = every thing between the cell membrane and the nuclear envelope Cytosolic proteins RER proteins Scaler reactions Vectorial reactions Lysosome Ultrastructure Secondary lysosomes Lysosome Enzymes present - phosphatases, proteases, nucleases, lipid degrading enzymes Lysosome Method of detection - localization of enzymes as primary lysosomes look like secretory granules Histochemical reaction using the local enzyme plus substrate to produce black precititate Localization of lysosomal enzymes Lysosome Negative charges on inner leaflet of lysosomal membrane - protect from -

ASAP, a Human Microtubule-Associated Protein Required for Bipolar Spindle Assembly and Cytokinesis
ASAP, a human microtubule-associated protein required for bipolar spindle assembly and cytokinesis Jean-Michel Saffin*, Magali Venoux*, Claude Prigent†, Julien Espeut‡, Francis Poulat*, Dominique Giorgi*, Ariane Abrieu‡, and Sylvie Rouquier*§ *Institut de Ge´ne´ tique Humaine, Centre National de la Recherche Scientifique, Unite´Propre de Recherche 1142, Rue de la Cardonille, 34396 Montpellier Ce´dex 5, France; †Centre National de la Recherche Scientifique, Unite´Mixte de Recherche 6061 Ge´ne´ tique et De´veloppement, Groupe Cycle Cellulaire, Equipe Labellise´e LNCC, Universite´de Rennes I, Institut Fe´de´ ratif de Recherche 140, 2 Avenue du Pr Le´on Bernard, 35043 Rennes, France; and ‡Centre de Recherche de Biochimie Macromole´culaire, Centre National de la Recherche Scientifique Formation de Recherche en Évolution 2593, 1919 Route de Mende, 34293 Montpellier Ce´dex 5, France Edited by J. Richard McIntosh, University of Colorado, Boulder, CO, and approved June 13, 2005 (received for review February 4, 2005) We have identified a unique human microtubule-associated pro- function, that directly binds to MTs. ASAP colocalizes with MTs in tein (MAP) named ASAP for ASter-Associated Protein. ASAP local- interphase, becomes associated with the mitotic spindle and spindle izes to microtubules in interphase, associates with the mitotic poles, and localizes to the central body and the residual body during spindle during mitosis, localizes to the central body during cyto- late mitosis and cytokinesis, respectively. We show that its overex- kinesis and directly binds to purified microtubules by its COOH- pression impedes the formation of a normal bipolar mitotic spindle. terminal domain. Overexpression of ASAP induces profound bun- We demonstrate that ASAP is an essential factor for successful dling of cytoplasmic microtubules in interphase cells and aberrant completion of mitosis, as depletion of ASAP from cells by RNA monopolar spindles in mitosis. -

Cytoskeletal Variations in an Asymmetric Cell Division Support Diversity in Nematode Sperm Size and Sex Ratios Ethan S
© 2017. Published by The Company of Biologists Ltd | Development (2017) 144, 3253-3263 doi:10.1242/dev.153841 RESEARCH ARTICLE Cytoskeletal variations in an asymmetric cell division support diversity in nematode sperm size and sex ratios Ethan S. Winter1,*, Anna Schwarz2,*, Gunar Fabig2,*, Jessica L. Feldman3,*, AndréPires-daSilva4, Thomas Müller-Reichert2, Penny L. Sadler1,5 and Diane C. Shakes1,‡ ABSTRACT During sperm development, asymmetric partitioning plays yet Asymmetric partitioning is an essential component of many another role; it streamlines sperm for optimal motility. Mature developmental processes. As spermatogenesis concludes, sperm sperm are small and motile, and thus one key step in their are streamlined by discarding unnecessary cellular components into differentiation is the post-meiotic shedding of organelles and cellular wastebags called residual bodies (RBs). During nematode cytoplasmic components that are either unnecessary for or spermatogenesis, this asymmetric partitioning event occurs shortly detrimental to subsequent sperm function (Fig. 1A). This after anaphase II, and both microtubules and actin partition into a shedding event involves two steps: (1) the differential partitioning central RB. Here, we use fluorescence and transmission electron of cellular components into a cellular wastebag known as a residual microscopy to elucidate and compare the intermediate steps of RB body (RB), and (2) the subsequent separation of this RB from the formation in Caenorhabditis elegans, Rhabditis sp. SB347 (recently sperm -

1 Stability and Function of a Putative Microtubule Organizing Center in The
bioRxiv preprint doi: https://doi.org/10.1101/099267; this version posted March 14, 2017. The copyright holder for this preprint (which was not certified by peer review) is the author/funder. All rights reserved. No reuse allowed without permission. Stability and function of a putative microtubule organizing center in the human parasite Toxoplasma gondii Jacqueline M. Leung1, Yudou He1, Fangliang Zhang2, Yu-Chen Hwang3, Eiji Nagayasu4, Jun Liu1, John M. Murray1, Ke Hu1# 1Department of Biology, Indiana University, Bloomington, IN, 47405, USA 2Department of Molecular and Cellular Pharmacology, University of Miami, Miller School of Medicine, Miami, FL, 33136, USA 3Nikon Instruments Inc., Melville, New York, 11747, USA 4Department of Infectious Diseases, University of Miyazaki, Miyazaki, Japan Running title: Stability of the apical polar ring #: Address correspondence to: Email: [email protected] 1 bioRxiv preprint doi: https://doi.org/10.1101/099267; this version posted March 14, 2017. The copyright holder for this preprint (which was not certified by peer review) is the author/funder. All rights reserved. No reuse allowed without permission. ABSTRACT The organization of the microtubule cytoskeleton is dictated by microtubule nucleators or organizing centers. Toxoplasma gondii, an important human parasite, has an array of 22 regularly spaced cortical microtubules stemming from a hypothesized organizing center, the apical polar ring. Here, we examine the functions of the apical polar ring by characterizing two of its components, KinesinA and APR1, and discovered that its putative role in templating can be separated from its mechanical stability. Parasites that lack both KinesinA and APR1 (ΔkinesinAΔapr1) are capable of generating 22 cortical microtubules. -
The Golgi Complex and Cell Secretion
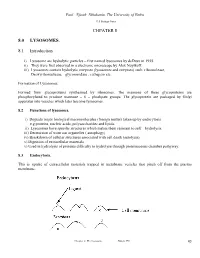
Paul Njiruh Nthakanio, The University of Embu Cell Biology Notes CHPATER 8 8.0 LYSOSOMES. 8.1 Introduction i) Lysosome are hydrolytic particles – first named lysosomes by deDuve in 1955. ii) They were first observed in a electronic microscope by Alex Noyikoff. iii) Lysosomes contain hydrolytic enzymes (lysosomes and enzymes) such ribonuclease, Deoxyribonuclease, glycoronidase , cathepsin etc. Formation of Lysosomes. Formed from glucoproteins synthesised by ribosomes. The mannose of these glycoproteins are phosphorylated to produce mannose – 6 – phoshpate groups. The glycoprotein are packaged by Golgi apparatus into vesicles which later become lysosomes. 8.2 Functions of lysosomes. i) Degrade major biological macromolecules (foreign matter) taken up by endocytosis e.g proteins, nucleic acids, polysaccharides and lipids. ii) Lysosomes have specific structures which makes them resistant to self – hydrolysis. iii) Destruction of worn out organelles ( autophagy) iv) Breakdown of cellular structures associated with cell death (autolysis). v) Digestion of extracellular materials. v) Used in hydrolysis of proteins difficulty to hydrolyse through proteinaceous chamber pathyway. 8.3 Endocytosis. This is uptake of extracellular materials trapped in membrane vesicles that pinch off from the plasma membrane. Chapter 8: The Lysosome. Njiruh. PN 43 Paul Njiruh Nthakanio, The University of Embu Cell Biology Notes 8.3.1 Definition of some terms i) Phagocytosis – refers to uptake of materials which form vesicles and consists of large particles (visible by light microscope). ii) Pinocytosis – refers to uptake of all other matter including small particles and soluble macromolecules such as antibodies, hormones and toxins. For endocytosis to take place there must be interaction between the material being ingested and the plasma membrane binding site. -

Autophagy in Human Skin Fibroblasts: Impact of Age
International Journal of Molecular Sciences Article Autophagy in Human Skin Fibroblasts: Impact of Age Hei Sung Kim 1 ID , Seo-Yeon Park 2, Seok Hoon Moon 1, Jeong Deuk Lee 1 and Sungjoo Kim 2,* 1 Department of Dermatology, Incheon St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, 222 Banpo-daero, Seocho-gu, Seoul 06591, Korea; [email protected] (H.S.K.); [email protected] (S.H.M.); [email protected] (J.D.L.) 2 Department of Medical Life Sciences, The Catholic University of Korea, 222 Banpo-daero, Seocho-gu, Seoul 06591, Korea; [email protected] * Correspondence: [email protected]; Tel.: +82-10-5599-2603 Received: 20 June 2018; Accepted: 27 July 2018; Published: 1 August 2018 Abstract: Autophagy is an intracellular stress response that is enhanced under starvation conditions, and also when the cellular components are damaged. Aging accompanies an increase in intracellular stress and has significant impact on the skin. Since dermal fibroblasts are a powerful indicator of skin aging, we compared the autophagic activity of human skin fibroblasts between the young and old. According to TEM analyses, the number of autophagosomes per 1 µm2 cytoplasmic area was similar between young and aged fibroblasts. The amount of LC3 (microtubule-associated protein 1 light chain 3)-II, a form associated with autophagic vacuolar membranes, was also similar between the groups from Western blot analysis. Although residual bodies were more common in aged dermal fibroblasts, LC3 turnover and p62 assay showed little difference in the rate of lysosomal proteolysis between the young and old. -

Lysosomes and the Skin
THE J OURNAL m- I NVEST IGATIVE DEIlMATOLOGY, 65:259- 27 1, 1975 Vol. 65, No. 3 Copyright © 1975 by The Williams & Wilkins Co. Printed in U.S.A . REVIEW ARTICLE James H. Herndon, Jr., M.D. Review Article Editor LYSOSOMES AND THE SKIN GERALD S. LAZARUS , M.D. · , VICTOR B. HATCHER , PH.D., AND NORMAN LEVINE , M .D. D epartments of M edicine and Biochemistry, Albert Einstein College of M edicine, and DiVl:sion of Dermatology, Department of M edicine, Montefi ore Hospital and Medical Center, Bron.x , New York The importance of lysosomes in cutaneous phys as a secondary lysosome or digestive vacuole (Fig. iology was a ppreciated early. The studies of Fell 1) . and Mellanby [1) on vitamin A induction of The substrate containing organell es can ori gi mucouS meta plasia in chick skin and the investiga nate by several distinct mechanisms . Heterophagy tions of Weissman and Fell [2] on lysosomal is a process by which t he cell can engulf foreign labilization by ultraviolet light, were landmarks in material into h eterophagoso mes (Fig. 1) by either our understanding of lysoso mal physiology. Subse phagocytosis, which is the uptake of larger, insolu quently lysosomes have been shown to be impor ble substances, or pinocytosis, which is the inges tant in keratinization, pigmentat ion, and seba tion of sma ll er soluble material. The two processes ceous secretion. The lysosomal system also partici are known coll ectively as endocytosis. The fusion pates in numerous pathologic processes in skin of a heterophagosome with a primary lysosome incl uding epidermal phagocytosis, inflammation, produces a digestive vacuole. -

Formation of Sperm Flagella and Removal of Cytoplasm by Autophagy
bioRxiv preprint doi: https://doi.org/10.1101/051219; this version posted May 3, 2016. The copyright holder for this preprint (which was not certified by peer review) is the author/funder. All rights reserved. No reuse allowed without permission. Dual functions of Intraflagellar Transport Protein IFT20 in spermiogenesis: formation of sperm flagella and removal of cytoplasm by autophagy Zhengang Zhang1, 2, Wei Li2, Yong Zhang2, 3, Ling Zhang2, 4, Maria E Teves2, Hong Liu2, 4, Junpin Liu2, 5, Jerome F Strauss III2, Gregory J Pazour6, James A Foster7, Rex A. Hess8, Zhibing Zhang2 1.Department of Gastroenterology, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, Hubei, China, 430030; 2. Department of Obstetrics and Gynecology, Virginia Commonwealth University, Richmond, VA, 23298; 3. Department of Dermatology, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, Hubei, China, 430030; 4. School of Public Health, Wuhan University of Science and Technology, Wuhan, Hubei, 430065; 5. Wuhan Hospital for the Prevention and Treatment of Occupational Diseases; 6. Program in Molecular Medicine, University of Massachusetts Medical School, Worcester, MA 01605; 7. Department of Biology, Randolph-Macon College, Ashland, VA 23005; 8. Comparative Biosciences, College of Veterinary Medicine, University of Illinois, 2001 S. Lincoln, Urbana, IL 61802-6199. Address correspondence to: Zhibing Zhang, MD, PhD Associate Professor Department of Obstetrics/Gynecology Virginia Commonwealth University 1101 E Marshall Street Richmond, VA, 23298 Email: [email protected] Running title: IFT20 and spermiogenesis 1 bioRxiv preprint doi: https://doi.org/10.1101/051219; this version posted May 3, 2016. The copyright holder for this preprint (which was not certified by peer review) is the author/funder. -

The Daily Rhythm of Shedding and Degradation of Rod and Cone Outer Segment Membranes in the Chick Retina
The daily rhythm of shedding and degradation of rod and cone outer segment membranes in the chick retina Richard W. Young Newly hatched chickens were maintained on a daily light cycle of 12 hr of light and 12 hr of darkness for 12 days. The pigment epithelium was then examined by electron microscopy at different times of day. Shortly after the beginning of the light period, the rods discarded groups of outer segment membranes. During the remainder of the light period, the membranes were degraded by the pigment epithelium. Early in the dark period, the cones shed membranes, which were digested by the pigment epithelial cells during the subsequent hours of darkness. Available evidence suggests that at least some of the chemical activities of the visual cells and pigment epithelium oscillate with a daily rhythm, tohich is synchronized with the daily fluctua- tion of light in the environment. Key words: visual cells, daily rhythms, renewal, retina, membranes The continual renewal of the light-sensitive steps of membrane assembly. Groups of old membranes of rod outer segments has been membranes are shed intermittently from the amply documented in a wide selection of ver- tips of the rods. This tends to occur early in tebrate animals. In fact, the process has been the morning, in animals maintained on a observed wherever it has been sought—in cycle of 12 hr of light and 12 hr of darkness.3 amphibia, reptiles, birds, fish, and mammals. The adjacent pigment epithelial cells, which It seems to be a fundamental and universal envelop the ends of the outer segments, in- characteristic of rod visual cells.1 gest and degrade the detached membranes.4 The basic mechanism of the renewal pro- In contrast, progress in our understanding cess in rods is "membrane replacement," of the mechanism by which the other class of which has two components: formation of new visual cells, the cones, renew their outer membranes and disposal of old ones.2 The segments had been frustratingly slow. -

Vertebrate Primary Cilia: a Sensory Part of Centrosomal Complex in Tissue Cells, but a “Sleeping Beauty” in Cultured Cells?
Cell Biology International Cell Biology International 28 (2004) 139–150 www.elsevier.com/locate/cellbi Vertebrate primary cilia: a sensory part of centrosomal complex in tissue cells, but a “sleeping beauty” in cultured cells? Irina B. Alieva*, Ivan A. Vorobjev Laboratory of Cell Motility, A.N. Belozersky Institute for Physico-Chemical Biology, Moscow State University, Moscow, 119992, Russia Received 22 July 2003; accepted 4 November 2003 Abstract Primary cilium development along with other components of the centrosome in mammalian cells was analysed ultrastructurally and by immunofluorescent staining with anti-acetylated tubulin antibodies. We categorized two types of primary cilia, nascent cilia that are about 1 µm long located inside the cytoplasm, and true primary cilia that are several µm long and protrude from the plasma membrane. The primary cilium is invariably associated with the older centriole of each diplosome, having appendages at the distal end and pericentriolar satellites with cytoplasmic microtubules emanating from them. Only one cilium per cell is formed normally through G0, S and G2 phases. However, in some mouse embryo fibroblasts with two mature centrioles, bicilates were seen. Primary cilia were not observed in cultured cells where the mature centriole had no satellites and appendages (Chinese hamster kidney cells, line 237, some clones of -fibroblasts). In contrast to primary cilia, striated rootlets were found around active and non-active centrioles with the same frequency. In proliferating cultured cells, a primary cilium can be formed several hours after mitosis, in fibroblasts 2–4 h after cell division and in PK cells only during the S-phase. In interphase cells, formation of the primary cilium can be stimulated by the action of metabolic inhibitors and by reversed depolymerization of cytoplasmic microtubules with cold or colcemid treatments.