FDA Approval Status and Research Evidence Quality - Psychotropic Medications in Children
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Report of the Advisory Group to Recommend Priorities for the IARC Monographs During 2020–2024
IARC Monographs on the Identification of Carcinogenic Hazards to Humans Report of the Advisory Group to Recommend Priorities for the IARC Monographs during 2020–2024 Report of the Advisory Group to Recommend Priorities for the IARC Monographs during 2020–2024 CONTENTS Introduction ................................................................................................................................... 1 Acetaldehyde (CAS No. 75-07-0) ................................................................................................. 3 Acrolein (CAS No. 107-02-8) ....................................................................................................... 4 Acrylamide (CAS No. 79-06-1) .................................................................................................... 5 Acrylonitrile (CAS No. 107-13-1) ................................................................................................ 6 Aflatoxins (CAS No. 1402-68-2) .................................................................................................. 8 Air pollutants and underlying mechanisms for breast cancer ....................................................... 9 Airborne gram-negative bacterial endotoxins ............................................................................. 10 Alachlor (chloroacetanilide herbicide) (CAS No. 15972-60-8) .................................................. 10 Aluminium (CAS No. 7429-90-5) .............................................................................................. 11 -

What's the Best First Line Anticonvulsant?
What’s the best first line anticonvulsant? Stephen Hanson, DVM, MS, Dip. ACVIM (Neurology) Recurring seizure activity is a relatively common problem in canine patients. Nowadays, there are several good options for medical treatment, which makes the choice of which drug to use a little more complicated. All anticonvulsant drugs have advantages and disadvantages, so the selection of a first-line drug should be tailored for the individual patient and client. Phenobarbital: This has been the standard first choice drug for decades. The nice thing about Phenobarbital is that it works fairly well, controlling seizures in about 70% of dogs with epilepsy. Also, it is inexpensive and readily available. The biggest down-sides are its induction of hepatic metabolism and the need for frequent upward dose adjustments, as well as its potential to cause hepatotoxicity. The potential for liver disease increases with time, so a 2 year old dog placed on this medication is more likely to develop hepatotoxicity in his life-time than a 10 year old dog. Phenobarbital can also cause sedation and ataxia. While this is usually mild/transient, it can be a real problem in dogs with other pre- existing signs of intracranial disease. Polyuria, polydipsia and polyphagia are other common side effects. These signs vary widely in severity between patients. Pros: cheap, available at any corner pharmacy, works well Cons: higher doses required with time, possible serious liver side-effects Good first-line choice for middle-aged to older dogs without any pre-existing liver issues Poor choice for dogs with liver disease, dogs with other intracranial signs Questionable choice for young epileptic dogs Potassium/sodium bromide: This was the most commonly-used add on anticonvulsant drug for a long time. -

Chapter 25 Mechanisms of Action of Antiepileptic Drugs
Chapter 25 Mechanisms of action of antiepileptic drugs GRAEME J. SILLS Department of Molecular and Clinical Pharmacology, University of Liverpool _________________________________________________________________________ Introduction The serendipitous discovery of the anticonvulsant properties of phenobarbital in 1912 marked the foundation of the modern pharmacotherapy of epilepsy. The subsequent 70 years saw the introduction of phenytoin, ethosuximide, carbamazepine, sodium valproate and a range of benzodiazepines. Collectively, these compounds have come to be regarded as the ‘established’ antiepileptic drugs (AEDs). A concerted period of development of drugs for epilepsy throughout the 1980s and 1990s has resulted (to date) in 16 new agents being licensed as add-on treatment for difficult-to-control adult and/or paediatric epilepsy, with some becoming available as monotherapy for newly diagnosed patients. Together, these have become known as the ‘modern’ AEDs. Throughout this period of unprecedented drug development, there have also been considerable advances in our understanding of how antiepileptic agents exert their effects at the cellular level. AEDs are neither preventive nor curative and are employed solely as a means of controlling symptoms (i.e. suppression of seizures). Recurrent seizure activity is the manifestation of an intermittent and excessive hyperexcitability of the nervous system and, while the pharmacological minutiae of currently marketed AEDs remain to be completely unravelled, these agents essentially redress the balance between neuronal excitation and inhibition. Three major classes of mechanism are recognised: modulation of voltage-gated ion channels; enhancement of gamma-aminobutyric acid (GABA)-mediated inhibitory neurotransmission; and attenuation of glutamate-mediated excitatory neurotransmission. The principal pharmacological targets of currently available AEDs are highlighted in Table 1 and discussed further below. -

BNSSG Shared Care Guidance Please Complete All Sections
NHS Bristol North Bristol NHS Trust NHS North Somerset University Hospitals Bristol NHS Foundation Trust NHS South Gloucestershire Weston Area Health NHS Trust BNSSG Shared Care Guidance Please complete all sections AMBER 3 month Section 1: Heading Avon & Wiltshire Mental Health Partnership NHS Trust Trust(s) Speciality / Department Mental Health Agreement for Lithium Drug (please prescribe by brand name and specify formulation: Priadel, Camcolit®, Liskonum®, Li-Liquid® ) 1. The management of acute manic or hypomanic episodes. 2. The management of episodes of recurrent depressive disorders where treatment with other antidepressants has Indication been unsuccessful. 3. The prophylaxis against bipolar affective disorders. 4. Control of aggressive behaviour or intentional self harm. Section 2: Treatment Schedule Dosage is adjusted based on serum-lithium concentration. Lithium levels must be taken 12 hours post dose, otherwise clinical value is lost. Lithium has a narrow therapeutic range necessitating blood levels between 0.4-1.2mmol/L. The lower end of this range is used for elderly and infirmed patients and the upper end for younger patients, particularly those being treated for an episode of mania. Clinicians should aim for levels of 0.6-0.8 mmol/L, with higher levels possibly being of benefit for patients with predominantly manic symptoms. Usual dose and frequency of Rarely 1.2mmol/L may be used. administration The starting dose is usually 400mg at night (200mg in the elderly), adjusted to achieve the desired serum-lithium concentration. Bloods should be taken 12 hours post dose. For tablet preparations dose is usually given as a single dose at night; for liquid preparations, the dose may be spilt to twice a day. -

(12) United States Patent (10) Patent No.: US 9,642,912 B2 Kisak Et Al
USOO9642912B2 (12) United States Patent (10) Patent No.: US 9,642,912 B2 Kisak et al. (45) Date of Patent: *May 9, 2017 (54) TOPICAL FORMULATIONS FOR TREATING (58) Field of Classification Search SKIN CONDITIONS CPC ...................................................... A61K 31f S7 (71) Applicant: Crescita Therapeutics Inc., USPC .......................................................... 514/171 Mississauga (CA) See application file for complete search history. (72) Inventors: Edward T. Kisak, San Diego, CA (56) References Cited (US); John M. Newsam, La Jolla, CA (US); Dominic King-Smith, San Diego, U.S. PATENT DOCUMENTS CA (US); Pankaj Karande, Troy, NY (US); Samir Mitragotri, Santa Barbara, 5,602,183 A 2f1997 Martin et al. CA (US); Wade A. Hull, Kaysville, UT 5,648,380 A 7, 1997 Martin 5,874.479 A 2, 1999 Martin (US); Ngoc Truc-ChiVo, Longueuil 6,328,979 B1 12/2001 Yamashita et al. (CA) 7,001,592 B1 2/2006 Traynor et al. 7,795,309 B2 9/2010 Kisak et al. (73) Assignee: Crescita Therapeutics Inc., 8,343,962 B2 1/2013 Kisak et al. Mississauga (CA) 8,513,304 B2 8, 2013 Kisak et al. 8,535,692 B2 9/2013 Pongpeerapat et al. (*) Notice: Subject to any disclaimer, the term of this 9,308,181 B2* 4/2016 Kisak ..................... A61K 47/12 patent is extended or adjusted under 35 2002fOOO6435 A1 1/2002 Samuels et al. 2002fOO64524 A1 5, 2002 Cevc U.S.C. 154(b) by 204 days. 2005, OO 14823 A1 1/2005 Soderlund et al. This patent is Subject to a terminal dis 2005.00754O7 A1 4/2005 Tamarkin et al. -

DEMAND REDUCTION a Glossary of Terms
UNITED NATIONS PUBLICATION Sales No. E.00.XI.9 ISBN: 92-1-148129-5 ACKNOWLEDGEMENTS This document was prepared by the: United Nations International Drug Control Programme (UNDCP), Vienna, Austria, in consultation with the Commonwealth of Health and Aged Care, Australia, and the informal international reference group. ii Contents Page Foreword . xi Demand reduction: A glossary of terms . 1 Abstinence . 1 Abuse . 1 Abuse liability . 2 Action research . 2 Addiction, addict . 2 Administration (method of) . 3 Adverse drug reaction . 4 Advice services . 4 Advocacy . 4 Agonist . 4 AIDS . 5 Al-Anon . 5 Alcohol . 5 Alcoholics Anonymous (AA) . 6 Alternatives to drug use . 6 Amfetamine . 6 Amotivational syndrome . 6 Amphetamine . 6 Amyl nitrate . 8 Analgesic . 8 iii Page Antagonist . 8 Anti-anxiety drug . 8 Antidepressant . 8 Backloading . 9 Bad trip . 9 Barbiturate . 9 Benzodiazepine . 10 Blood-borne virus . 10 Brief intervention . 11 Buprenorphine . 11 Caffeine . 12 Cannabis . 12 Chasing . 13 Cocaine . 13 Coca leaves . 14 Coca paste . 14 Cold turkey . 14 Community empowerment . 15 Co-morbidity . 15 Comprehensive Multidisciplinary Outline of Future Activities in Drug Abuse Control (CMO) . 15 Controlled substance . 15 Counselling and psychotherapy . 16 Court diversion . 16 Crash . 16 Cross-dependence . 17 Cross-tolerance . 17 Custody diversion . 17 Dance drug . 18 Decriminalization or depenalization . 18 Demand . 18 iv Page Demand reduction . 19 Dependence, dependence syndrome . 19 Dependence liability . 20 Depressant . 20 Designer drug . 20 Detoxification . 20 Diacetylmorphine/Diamorphine . 21 Diuretic . 21 Drug . 21 Drug abuse . 22 Drug abuse-related harm . 22 Drug abuse-related problem . 22 Drug policy . 23 Drug seeking . 23 Drug substitution . 23 Drug testing . 24 Drug use . -

Guidance on the Use of Mood Stabilizers for the Treatment of Bipolar Affective Disorder Version 2
Guidance on the use of mood stabilizers for the treatment of bipolar affective disorder Version 2 RATIFYING COMMITTEE DRUGS AND THERAPEUTICS GROUP DATE RATIFIED July 2015 REPLACES Version 1 dated July 2013 NEXT REVIEW DATE July 2017 POLICY AUTHORS Jules Haste, Lead Pharmacist, Brighton and Hove Members of the Pharmacy Team (contributors are listed overleaf) If you require this document in an alternative format, i.e. easy read, large text, audio or Braille please contact the pharmacy team on 01243 623349 Page 1 of 49 Contributors Jed Hewitt, Chief Pharmacist - Governance & Professional Practice James Atkinson, Pharmacist Team Leader Mental Health and Community Services Miguel Gomez, Lead Pharmacist, Worthing. Hilary Garforth, Lead Pharmacist, Chichester. Pauline Daw, Lead Pharmacist (CRHTs & AOT), East Sussex. Iftekhar Khan, Lead Pharmacist (S&F Service), East Sussex. Graham Brown, Lead Pharmacist CAMHS & EIS. Gus Fernandez, Specialist Pharmacist MI and MH Lisa Stanton, Specialist Pharmacist Early Intervention Services & Learning Disabilities. Nana Tomova, Specialist Pharmacist, Crawley. Page 2 of 49 Section Title Page Number Introduction and Key Points 4 1. General principles in the treatment of acute mania 6 2. General principles in the treatment of bipolar depression 8 3. General principles in long term treatment 10 4. Rapid cycling 13 5. Physical health 13 6. Treatment in special situations 6.1 Pregnancy 15 6.2 Breast-feeding 17 6.3 Older adults 19 6.4 Children and adolescents 22 6.5 Learning disabilities 29 6.6 Cardiac dysfunction 30 6.7 Renal dysfunction 34 6.8 Hepatic dysfunction 37 6.9 Epilepsy 41 7. The risk of switching to mania with antidepressants 43 8. -

Homicide and Associated Steroid Acute Psychosis: a Case Report
Hindawi Publishing Corporation Case Reports in Medicine Volume 2011, Article ID 564521, 4 pages doi:10.1155/2011/564521 Case Report Homicide and Associated Steroid Acute Psychosis: A Case Report G. Airagnes,1, 2 C. Rouge-Maillart,1, 3 J.-B. Garre,2, 3 and B. Gohier2 1 Service de M´edecine L´egale, CHU d’Angers, 49933 Angers Cedex 09, France 2 D´epartement de Psychiatrie et de Psychologie m´edicale, CHU d’Angers, 49933 Angers Cedex 09, France 3 IFR 132, Universit´e d’Angers, 49035 Angers, France Correspondence should be addressed to G. Airagnes, [email protected] Received 22 June 2011; Revised 26 August 2011; Accepted 26 September 2011 Academic Editor: Massimo Gallerani Copyright © 2011 G. Airagnes et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. We report the case of an old man treated with methylprednisolone for chronic lymphoid leukemia. After two months of treatment, he declared an acute steroid psychosis and beat his wife to death. Steroids were stopped and the psychotic symptoms subsided, but his condition declined very quickly. The clinical course was complicated by a major depressive disorder with suicidal ideas, due to the steroid stoppage, the leukemia progressed, and by a sudden onset of a fatal pulmonary embolism. This clinical case highlights the importance of early detection of steroid psychosis and proposes, should treatment not be stopped, a strategy of dose reduction combined with a mood stabilizer or antipsychotic treatment. -

Therapeutic Drug Monitoring Clinical Guide FOURTH EDITION
DIAGNOSTICS Therapeutic Drug Monitoring Clinical Guide FOURTH EDITION 1 Therapeutic Drug Monitoring Clinical Guide FOURTH EDITION Authors Mike Hallworth, MA, MSc, FRCPath Former Consultant Biochemist Royal Shrewsbury Hospital United Kingdom Ian Watson, MSc, PhD, FRCPath Former Consultant Biochemist and Toxicologist University Hospital Aintree Liverpool, United Kingdom Editors of the David Holt, DSc, PhD Third Edition Susan Tett, PhD, BPharm (Hons), MPS Steven H. Wong, PhD, DABCC (TC), FACB 2 CONTENTS THERAPEUTIC DRUG MONITORING . 5 RUFINAMIDE . 81 WHY IS TDM NECESSARY? . 6 TIAGABINE . 83 WHICH DRUGS SHOULD BE MONITORED? . 8 TOPIRAMATE . 85 PRACTICAL CONSIDERATIONS . 10 VALPROATE . 87 CALCULATION OF DOSAGE ADJUSTMENT . 15 VIGABATRIN . 89 OTHER APPROACHES TO OPTIMIZING THERAPY — ZONISAMIDE . 91 PHARMACOGENETICS AND BIOMARKERS . 17 ANTIFUNGALS . 94 EFFECTIVENESS OF TDM – DOES IT HELP PATIENTS? . 19 POSOCONAZOLE/VORICONAZOLE . 95 REFERENCES . 21 ANTINEOPLASTICS . 98 WEBSITES . 23 BUSULFAN . 99 DRUG DATA PROFILES . 24 METHOTREXATE . 101 PREFACE . 24 ANTIRETROVIRALS . 104 ADDICTION THERAPEUTICS . 28 ANTIRETROVIRALS . 105 BUPRENORPHINE . 29 BRONCHODILATOR, ANALEPTIC . 108 METHADONE . 31 THEOPHYLLINE . 109 ANALGESICS . 34 CAFFEINE . 111 ACETAMINOPHEN (PARACETAMOL) . 35 CARDIAC AGENTS . 114 ACETYLSALICYLIC ACID (ASPIRIN) . 37 ANTI-ARRHYTHMICS MORPHINE . 39 AMIODARONE . 115 ANTIBIOTICS . 42 DISOPYRAMIDE . 117 AMINOGLYCOSIDES FLECAINIDE . 119 AMIKACIN . 43 LIDOCAINE . 121 GENTAMICIN . 45 CARDIAC GLYCOSIDES TOBRAMYCIN . 47 DIGOXIN . 123 OTHER ANTIBIOTICS -
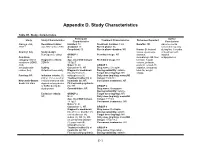
Appendix D. Study Characteristics
Appendix D. Study Characteristics Table D1. Study characteristics Participant Author Study Study Characteristics Treatment Characteristics Outcomes Reported Characteristics Conclusions Alacqua et al., Recruitment dates: Enrolled: 73 Treatment duration: 3 mo Benefits: NR Adverse events 2008 96 Jan 2002 to Dec 2003 Analyzed: 73 Run-in phase: No occurred frequently Completed: 50 Run-in phase duration: NR Harms: Behavioral during first 3 months Country: Italy Study design: issues, dyskinesia, of treatment with Retrospective cohort GROUP 1 Permitted drugs: NR dystonia, atypical Condition N: 2 dermatologic AE, liver antipsychotics. category: Mixed Diagnostic criteria: Age, mean±SD (range): Prohibited drugs: NR function, hepatic conditions (ADHD, DSM-IV 15.5±0.7 volume, prolactin, ASD, Males %: 50 GROUP 1 prolactin-related AE, schizophrenia- Setting: Caucasian %: NR Drug name: Clozapine sedation, sleepness, related, tics) Outpatient/community Diagnostic breakdown Dosing variability: variable total AE, weight (n): psychosis (1), Target dose (mg/day): NR change Funding: NR Inclusion criteria: (1) schizophrenia (1) Daily dose (mg/day), mean±SD ≤18 yr, (2) received an Treatment naïve (n): all (range): 150±70.1 Newcastle-Ottawa incident treatment with Inpatients (n): NR Concurrent treatments: NR Scale: 6/8 stars atypical antipsychotics First episode psychosis or SSRIs during the (n): NR GROUP 2 study period Comorbidities: NR Drug name: Olanzapine Dosing variability: variable Exclusion criteria: GROUP 2 Target dose (mg/day): NR NR N: 24 Daily dose -

Neurosteroid Metabolism in the Human Brain
European Journal of Endocrinology (2001) 145 669±679 ISSN 0804-4643 REVIEW Neurosteroid metabolism in the human brain Birgit Stoffel-Wagner Department of Clinical Biochemistry, University of Bonn, 53127 Bonn, Germany (Correspondence should be addressed to Birgit Stoffel-Wagner, Institut fuÈr Klinische Biochemie, Universitaet Bonn, Sigmund-Freud-Strasse 25, D-53127 Bonn, Germany; Email: [email protected]) Abstract This review summarizes the current knowledge of the biosynthesis of neurosteroids in the human brain, the enzymes mediating these reactions, their localization and the putative effects of neurosteroids. Molecular biological and biochemical studies have now ®rmly established the presence of the steroidogenic enzymes cytochrome P450 cholesterol side-chain cleavage (P450SCC), aromatase, 5a-reductase, 3a-hydroxysteroid dehydrogenase and 17b-hydroxysteroid dehydrogenase in human brain. The functions attributed to speci®c neurosteroids include modulation of g-aminobutyric acid A (GABAA), N-methyl-d-aspartate (NMDA), nicotinic, muscarinic, serotonin (5-HT3), kainate, glycine and sigma receptors, neuroprotection and induction of neurite outgrowth, dendritic spines and synaptogenesis. The ®rst clinical investigations in humans produced evidence for an involvement of neuroactive steroids in conditions such as fatigue during pregnancy, premenstrual syndrome, post partum depression, catamenial epilepsy, depressive disorders and dementia disorders. Better knowledge of the biochemical pathways of neurosteroidogenesis and -

Safety Data Sheet
SAFETY DATA SHEET Creation Date 22-Sep-2009 Revision Date 27-Dec-2020 Revision Number 2 SECTION 1: IDENTIFICATION OF THE SUBSTANCE/MIXTURE AND OF THE COMPANY/UNDERTAKING 1.1. Product identifier Product Description: Lithium citrate tribasic tetrahydrate Cat No. : 47373 Synonyms Lithium citrate tetrahydrate Molecular Formula C6 H5 Li3 O7 . 4 H2 O 1.2. Relevant identified uses of the substance or mixture and uses advised against Recommended Use Laboratory chemicals. Uses advised against No Information available 1.3. Details of the supplier of the safety data sheet Company Thermo Fisher (Kandel) GmbH . Erlenbachweg 2 76870 Kandel Germany Tel: +49 (0) 721 84007 280 Fax: +49 (0) 721 84007 300 E-mail address [email protected] www.alfa.com Product safety Tel + +049 (0) 7275 988687-0 1.4. Emergency telephone number Carechem 24: +44 (0) 1235 239 670 (Multi-language emergency number) Poison Information Center Mainz www.giftinfo.uni-mainz.de Telephone: +49(0)6131/19240 Exclusively for customers in Austria: Poison Information Center (VIZ) Emergency call 0-24 clock: +43 1 406 43 43 Office hours: Monday to Friday, 8am to 4pm, tel: +43 1 406 68 98 SECTION 2: HAZARDS IDENTIFICATION 2.1. Classification of the substance or mixture CLP Classification - Regulation (EC) No 1272/2008 Physical hazards Based on available data, the classification criteria are not met ______________________________________________________________________________________________ ALFAA47373 Page 1 / 10 SAFETY DATA SHEET Lithium citrate tribasic tetrahydrate Revision Date 27-Dec-2020 ______________________________________________________________________________________________ Health hazards Based on available data, the classification criteria are not met Environmental hazards Based on available data, the classification criteria are not met Full text of Hazard Statements: see section 16 2.2.