Issue - 10 Vol
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Bank Wise-District Wise Bank Branches (Excluding Cooperative
Bank wise-District wise Bank Branches (Excluding Cooperative Bank/District No. of Branches Allahabad Bank 205 Agar-Malwa 2 Anuppur 2 Balaghat 4 Bhopal 25 Burhanpur 1 Chhatarpur 3 Chhindwara 8 Damoh 3 Datia 1 Dewas 1 Dhar 1 Dindori 1 East Nimar 1 Gwalior 3 Harda 1 Hoshangabad 3 Indore 12 Jabalpur 24 Katni 6 Mandla 4 Mandsaur 2 Morena 1 Narsinghpur 7 Neemuch 2 Panna 3 Raisen 1 Rajgarh 2 Ratlam 2 Rewa 16 Sagar 6 Satna 28 Sehore 2 Seoni 2 Shahdol 3 Shajapur 1 Shivpuri 2 Sidhi 5 Singrauli 6 Tikamgarh 1 Ujjain 2 Vidisha 4 West Nimar 1 Andhra Bank 45 Betul 1 Bhind 1 Bhopal 8 Burhanpur 1 Chhindwara 1 Dewas 1 Dhar 1 East Nimar 1 Gwalior 2 Harda 1 Hoshangabad 2 Indore 11 Jabalpur 3 Katni 1 Narsinghpur 2 Rewa 1 Sagar 1 Satna 1 Sehore 2 Ujjain 1 Vidisha 2 Au Small Finance Bank Ltd. 37 Agar-Malwa 1 Barwani 1 Betul 1 Bhopal 2 Chhatarpur 1 Chhindwara 2 Dewas 2 Dhar 2 East Nimar 1 Hoshangabad 1 Indore 2 Jabalpur 1 Katni 1 Mandla 1 Mandsaur 2 Neemuch 1 Raisen 2 Rajgarh 1 Ratlam 2 Rewa 1 Satna 1 Sehore 2 Shajapur 1 Tikamgarh 1 Ujjain 1 Vidisha 2 West Nimar 1 Axis Bank Ltd. 136 Agar-Malwa 1 Alirajpur 1 Anuppur 1 Ashoknagar 1 Balaghat 1 Barwani 3 Betul 2 Bhind 1 Bhopal 20 Burhanpur 1 Chhatarpur 1 Chhindwara 2 Damoh 1 Datia 1 Dewas 1 Dhar 4 Dindori 1 East Nimar 1 Guna 2 Gwalior 10 Harda 1 Hoshangabad 3 Indore 26 Jabalpur 5 Jhabua 2 Katni 1 Mandla 1 Mandsaur 1 Morena 1 Narsinghpur 1 Neemuch 1 Panna 1 Raisen 2 Rajgarh 2 Ratlam 2 Rewa 1 Sagar 3 Satna 2 Sehore 1 Seoni 1 Shahdol 1 Shajapur 2 Sheopur 1 Shivpuri 2 Sidhi 2 Singrauli 2 Tikamgarh 1 Ujjain 5 Vidisha 2 West Nimar 4 Bandhan Bank Ltd. -
Contact List
State District Phone No Adress ICICI LOMBARD GIC MP Agar Malwa Amit Gupta 9919002646 Durga Plaza, 1st Floor, House no. 37, Freeganj, Ujjain – 456010 ICICI LOMBARD GIC, MP Anuppur Ramesh Joshi 7408432160 Burhar Road, Above Mewar Hospital, Shahdol- 484001 ICICI LOMBARD GIC MP Dewas Mohd Shahnawaz 9758802175 Durga Plaza, 1st Floor, House no. 37, Freeganj, Ujjain – 456010 ICICI LOMBARD GIC, MP Mandsaur Rakesh Rojde 8657450353 3rd Floor, Lunwat Plaza, 19 College Road, Ratlam - 457001 ICICI LOMBARD GIC, MP Neemuch Sharad Sharma 9918901588 3rd Floor, Lunwat Plaza, 19 College Road, Ratlam - 457001 ICICI LOMBARD GIC, MP Ratlam Navdeep Saxena 9648935524 3rd Floor, Lunwat Plaza, 19 College Road, Ratlam - 457001 ICICI LOMBARD GIC, MP Shahdol Sudhir Mishra 9534024900 Burhar Road, Above Mewar Hospital, Shahdol- 484001 ICICI LOMBARD GIC MP Shajapur Ratnesh Singh 7045193704 Durga Plaza, 1st Floor, House no. 37, Freeganj, Ujjain – 456010 ICICI LOMBARD GIC MP Ujjain Amit Ghode 9039708869 Durga Plaza, 1st Floor, House no. 37, Freeganj, Ujjain – 456010 ICICI LOMBARD GIC, MP Umaria Ravendra Kushwaha 7389918115 Burhar Road, Above Mewar Hospital, Shahdol- 484001 MP State Head Sourav Kumar Sethi 9674751470 State District Phone No Adress 3rd Floor, North Block, Bahu Plaza Jammu-180001, Jammu J&K Doda Mudasir Bhat 01912474024 & Kashmir 3rd Floor, Chinar Complex, Residency Road, Srinagar- J&K Poonch Farooq Wani 01942457073 190001, Jammu & Kashmir 3rd Floor, Chinar Complex, Residency Road, Srinagar- J&K Ramban Afroza Rashid 01942457073 190001, Jammu & Kashmir 3rd -

One Time ODF+ & ODF++ Updated.Xlsx
ODF++ Certified: 958 State Number of ULB Certified Andaman and Nicobar 1 Andhra Pradesh 7 Chandigarh 1 Chhattisgarh 169 Delhi 3 Gujarat 111 Haryana 14 Himachal Pradesh 2 Jharkhand 3 Karnataka 2 Madhya Pradesh 296 Maharashtra 213 Odisha 21 Punjab 66 Rajasthan 6 Telangana 9 Uttar Pradesh 31 Uttarakhand 3 Grand Total 958 ULB Census Code State District ULB 804041 Andaman and Nicobar South Andaman Port Blair 802947 Andhra Pradesh Visakhapatnam Greater Visakhapatnam 802969 Andhra Pradesh Krishna Vijaywada 803014 Andhra Pradesh Chittoor Tirupati 802988 Andhra Pradesh Prakasam Ongole 802982 Andhra Pradesh Guntur Tenali 802940 Andhra Pradesh Srikakulam Rajam 802952 Andhra Pradesh East Godavari Rajahmundry 800286 Chandigarh Chandigarh Chandigarh 801911 Chhattisgarh Koria Baikunthpur_C 801912 Chhattisgarh Koria Manendergarh 801913 Chhattisgarh Koria Khongapani 801914 Chhattisgarh Koria Jhagrakhand 801915 Chhattisgarh Koria Nai ledri 801916 Chhattisgarh Koria Chirimiri 801918 Chhattisgarh Balrampur Balrampur_C 801919 Chhattisgarh Balrampur Wadrafnagar 801921 Chhattisgarh Surajpur Jarhi 801922 Chhattisgarh Balrampur Kusmi 801926 Chhattisgarh Surajpur Premnagar 801927 Chhattisgarh Sarguja Ambikapur 801928 Chhattisgarh Kathua Lakhanpur_C 801929 Chhattisgarh Balrampur Rajpur_C 801930 Chhattisgarh Sarguja Sitapur_CH 801932 Chhattisgarh JashpurNagar Jashpur 801934 Chhattisgarh JashpurNagar Kotba 801936 Chhattisgarh Raigarh Lailunga 801937 Chhattisgarh Raigarh Gharghora 801939 Chhattisgarh Raigarh Raigarh 801941 Chhattisgarh Raigarh Kharsia 801944 Chhattisgarh -

DIP Ratlam.Pdf
Contents S. No. Topic Page No. 1. General Characteristics of the District 03 1.1 Location & Geographical Area 03 1.2 Topography 03 1.3 Availability of Minerals. 04 1.4 Forest 04 1.5 Administrative set up 04 2. District at a glance 5-7 2.1 Existing Status of Industrial Area in the District Ratlam 08 3. Industrial Scenario Of -Ratlam 08 3.1 Industry at a Glance 08 3.2 Year Wise Trend Of Units Registered 09 3.3 Details Of Existing Micro & Small Enterprises & Artisan Units In 10 The District 3.4 Large Scale Industries / Public Sector undertakings 11 3.5 Major Exportable Item 11 3.6 Growth Trend 11 3.7 Vendorisation / Ancillarisation of the Industry 11 3.8 Medium Scale Enterprises 11 3.8.1 List of the units in Ratlam & near by Area 12 3.8.2 Major Exportable Item 12 3.9 Service Enterprises 12 3.9.1 Coaching Industry 12 3.9.2 Potentials areas for service industry 12 3.10 Potential for new MSMEs 12 4 Steps to set up MSMEs 13 Page 2 Brief Industrial Profile of Ratlam District 1. General Characteristics of the District Ratlam 1.1 Location & Geographical Area. Ratlam is situated in North-West region of Madhya Pradesh from 23 05' North to 23 52' North Longitude and 74 31' East to 75 41' East Latitude. It is bounded by Mandsaur District in North, Jhabua and Dhar on t he South, Ujjain on the East, Chhitorgarh and Banswara District of Rajasthan on the West, Shajapur District of Madhya Pradesh and Jhalawar District of Rajasthan on the North. -

Agenda for 590Th SEIAA Meeting Dated 19.12.2019 1
Agenda for 590th SEIAA Meeting dated 19.12.2019 1. Case No. – 6672/2019 Shri Rohit Kumar Sharma, C.P.Mission Compound, Dist. Jhansi, UP – 472001 Prior Environment Clearance for Granite (Dimension Stone) Mine in an area of 4.00 ha. (1,200 cum per annum) (Khasra No. 21), Village - Vijaypur, Tehsil - Mohangarh, Dist. Tikamgarh, (MP). 2. Case No. – 6658/2019 Shri Rao Anuj Pratap Singh, Shri Maa Mining Office No. 2, Manglam, Village - Lolri Rajmarg, Tehsil - Tendukheda, Dist. Narsinghpur, MP – 487330 Prior Environment Clearance for Stone Quarry in an area of 3.50 ha. (16,875 cum per annum) (Khasra No. 54, 57), Village - Nadiya, Tehsil - Kesli, Dist. Sagar, (MP) 3. Case No. – 6643/2019 Shri Hemraj Meena, Ward No. 12, Ibrahimpura, Jhora Narsingarh Road, Berasia, Dist. Bhopal, MP – 464106 Prior Environment Clearance for Murrum Quarry in an area of 2.00 ha. (10,500 cum per annum) (Khasra No. 7/1), Village - Baabddiikhaar, Tehsil - Berasia, Dist. Bhopal, (MP). 4. Case No. – 6676/2019 Shri Arvind Sharma S/o Shri Ramnarayan Sharma, Village - Dongargaon, Tehsil - Susner, Dist. Agar Malwa, MP – 465449 Prior Environment Clearance for Metal Stone Quarry in an area of 2.00 ha. (15,000 cum per annum ) (Khasra No. 885), Village - Dongargaon, Tehsil - Susner, Dist. Agar Malwa, (MP) 5. Case No. 6459/2019 Smt. Beena Singh W/o Shri Rishi Kumar Singh, R/o Semariya, Tehsil - Gopad Banas, Dist. Sidhi, MP- Prior Environment Clearance for Metal Stone Quarry in an area of 3.130 ha. (20815 cum per annum) (Khasra No. 466, 74, 75 Parts), Village - Karaundi & Kushiyari, Tehsil - Bahari, Dist. -

State:Madhya Pradesh Agriculture Contingency Plan: Shajapur District
State:Madhya Pradesh Agriculture Contingency Plan: Shajapur District 1.0 District Agriculture profile 1.1 Agro -Climatic /Ecological Zone IX Agro Ecological Sub Region (ICAR) Sub region No.13,AE Sub region 5.2, Agro ecological region :I 5D2& I 5 C3 Agro-Climatic Region (Planning Sub Zone 24, ACZ 9.3,Region : Central Plateau, PCS3 Commission) Agro Climatic Zone (NARP) Malwa Plateau Agroecological Zone(X) List all the districts or part thereof falling Indore, Ujjain, Ratlam, Mandsour, Nimach, Rajgarh, some part of Dhar and Jhabua district under the NARP Zone Geographic coordinates of district Latitude Longitude Altitude 23.06 0 to 24.19 0 N 75.41 0 to 77.02 0E 453 mm Name and address of the concerned ZRS/ Zonal Agricultural Research Station, College of Agriculture, Old Sehore road near to Daly college, ZARS/ RARS/ RRS/ RRTTS Indore Madhya Pradesh-452 001 Mention the KVK located in the district Krishi Vigyan Kendra, Girwar, Shajapur (M.P.) 465001 1.2 Rainfall Average (mm) Normal Onset Normal Cessation ( specify week and month) (specify week and month) SW monsoon (June-Sep): 697.6 3rd week of june Last week of sept NE Monsoon(Oct-Dec): 221 Winter (Jan- March) 00 - - Summer (Apr-May) 00 - - Annual 927 - - 1.3 Land use Geographical Forest Land under Permanent Cultivable Land under Barren and Current Other pattern of the area area non- pastures wasteland Misc. tree uncultivable fallows fallows district (latest agricultural crops and land statistics) use groves Area (Lakh ha) 6.18 0.06 1.02 0.5 0.10 -- 0.02 -- -- 1. -

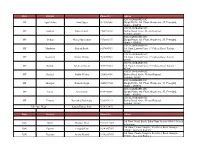
MPCON UBI Bank Mitr Madhya Pradesh
Full Postal Address Location of Photo of Bank Name of Name of Name of Name of Bank Gender Bank Mitra Sr No Vendor with Pincode (Bank BC Mitra Bank State District Mitra (M/F/O) Mobile No Longit Latitu Mitra Fixed Location ude de (JPG/PNG At/Post- Bangli Block- Union Bank Madhya Lakhan Singh Moman Badodia Dist- 1 MPCON SHAJAPUR M 9893218989 of India Pradesh Kelwa Shajapur State- Madhya Pradesh At/Post- Dastakhedi Union Bank Madhya Block- Moman Badodia 2 MPCON SHAJAPUR Anand Mewada M 8458819815 of India Pradesh Dist- Shajapur State- Madhya Pradesh At/Post- Dhanana Block- Union Bank Madhya Harnam Moman Badodia Dist- 3 MPCON SHAJAPUR M 9826985961 of India Pradesh Mewada Shajapur State- Madhya Pradesh At/Post- Kiloda Block- Union Bank Madhya Bheru Singh Moman Badodia Dist- 4 MPCON SHAJAPUR M 9424059754 of India Pradesh Patidar Shajapur State- Madhya Pradesh At/Post- Bhesoon Block- Union Bank Madhya RAJESH 5 MPCON DEWAS M Kannod Dist- Dewas 9893928290 of India Pradesh MUNDRA State- Madhya Pradesh At/Post- Lohari Block- Union Bank Madhya VIRENDRA 9406874280/8 6 MPCON DEWAS M Dewas Dist- Dewas of India Pradesh SINGH 965969224 State- Madhya Pradesh At/Post- Rehmanpura Union Bank Madhya GAJANAND Block- Kannod Dist- 7 MPCON DEWAS M 9993818205 of India Pradesh MEENA Dewas State- Madhya Pradesh At/Post- Ssa112284 Union Bank Madhya 8 MPCON DHAR Teena sisodiya F Block- Bagh Dist- Dhar 9826825206 of India Pradesh State- Madhya Pradesh At/Post- Ssa113348 Union Bank Madhya 9 MPCON DHAR Bherulal Parmar M Block- Dhar Dist- Dhar 9165289863 of India Pradesh -

Answered On:08.05.2002 Computerised Telephone Exchanges in Madhya Pradesh Jaibhan Singh Pawaiya
GOVERNMENT OF INDIA COMMUNICATIONS AND INFORMATION TECHNOLOGY LOK SABHA UNSTARRED QUESTION NO:6364 ANSWERED ON:08.05.2002 COMPUTERISED TELEPHONE EXCHANGES IN MADHYA PRADESH JAIBHAN SINGH PAWAIYA Will the Minister of COMMUNICATIONS AND INFORMATION TECHNOLOGY be pleased to state: (a) the number of computerised trunk telephone exchanges operating in Madhya Pradesh; (b) the number of such telephone exchanges proposed to be introduced in the State during the current year; and (c) the details of telephone exchanges expanded in the State during 2001-2002 and proposed to be expanded during 2002-2003? Answer THE MINISTER OF STATE IN THE MINISTRY OF COMMUNICATIONS AND INFORMATION TECHNOLOGY (SHRI TAPAN SIKDAR) (a) Sir, there is one conputerised trunk telephone exchange at Indore with one Remote Unit at Bhopal in Madhya Pradesh. (b) There is no proposal to introduce such conputerised trunk telephone exchange in the state during current year. (c) The details are given in Annexure I and II. Annexure- I Local Exchanges capacity expanded in M P Circle during 2001-02 Sl SSA Name of Station Capacity Expanded 1 Balaghat Baihar 660 2 Balaghat Balaghat 2000 3 Balaghat Kirnapur 400 4 Balaghat Lalburra 400 5 Balaghat Tirodi 176 6 Betul Amla 488 7 Betul Athner 176 8 Betul Bhainsdehi 424 9 Betul Bhimpur 176 10 Betul Chicholi 152 11 Betul Chopna 184 12 Bhind Bhind 2192 13 Bhind Gohad 128 14 Bhind Lahar 400 15 Bhind Mehgaon 256 16 Bhind Phooph 208 17 Bhopal Barkhedihasan 152 18 Bhopal Berasia 216 19 Bhopal Bhopal 10980 20 Bhopal Doraha 144 21 Bhopal Sehore 360 -
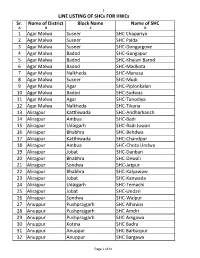
HWC-SHC Allotment List for CCCH
1 LINE LISTING OF SHCs FOR HWCs Sr. Name of District Block Name Name of SHC A B C D 1 Agar Malwa Susner SHC Chapariya 2 Agar Malwa Susner SHC Palda 3 Agar Malwa Susner SHC-Dongargove 4 Agar Malwa Badod SHC-Gangapur 5 Agar Malwa Badod SHC-Khajuri Barod 6 Agar Malwa Badod SHC-Madkota 7 Agar Malwa Nalkheda SHC-Manasa 8 Agar Malwa Susner SHC-Modi 9 Agar Malwa Agar SHC-Piplonkalan 10 Agar Malwa Badod SHC-Sudwas 11 Agar Malwa Agar SHC-Tanodiya 12 Agar Malwa Nalkheda SHC-Tikona 13 Alirajpur Katthiwada SHC-Andharkanch 14 Alirajpur Ambua SHC-Badi 15 Alirajpur Udaigarh SHC-Badi Juwari 16 Alirajpur Bhabhra SHC-Behdwa 17 Alirajpur Katthiwada SHC-Chandpur 18 Alirajpur Ambua SHC-Chota Undwa 19 Alirajpur Jobat SHC-Danbari 20 Alirajpur Bhabhra SHC-Dewali 21 Alirajpur Sondwa SHC-Jetpur 22 Alirajpur Bhabhra SHC-Kalyawaw 23 Alirajpur Jobat SHC-Kanwada 24 Alirajpur Udaigarh SHC-Temachi 25 Alirajpur Jobat SHC-Undari 26 Alirajpur Sondwa SHC-Walpur 27 Anuppur Pushprajgarh SHC Alhawar 28 Anuppur Pushprajgarh SHC Amdri 29 Anuppur Pushprajgarh SHC Amgawa 30 Anuppur Kotma SHC Badra 31 Anuppur Anuppur SHC Barbaspur 32 Anuppur Anuppur SHC Bargawa Page 1 of 41 2 LINE LISTING OF SHCs FOR HWCs Sr. Name of District Block Name Name of SHC 33 Anuppur Jaithari SHC Beend 34 Anuppur Kotma SHC Beiharbandh 35 Anuppur Pushprajgarh SHC Bilaspur 36 Anuppur Kotma SHC Chaka 37 Anuppur Jaithari SHC Choi 38 Anuppur Jaithari SHC Chorbhdhi 39 Anuppur Jaithari SHC Chulha 40 Anuppur Kotma SHC Dhangawa 41 Anuppur Pushprajgarh SHC Gonda 42 Anuppur Jaithari SHC Gorshi 43 Anuppur Anuppur -

Ratlam District Madhya Pradesh
RATLAM DISTRICT MADHYA PRADESH Ministry of Water Resources Central Ground Water Board North Central Region Government of India BHOPAL 2013 1 RATLAM DISTRICT AT A GLANCE S.No. Items Statistics 1. General Information i) Geographical area 486100 Ha ii) Administrative Divisions (As on 2013) Number of Tehsil/Blocks 6/6 Number of Villages 1086 iii) Population (Census 2011) 1,454,483 iv) Normal Rainfall 992.90 mm 2. Geomorphology 1. Major Physiographic Units: 1. i. Malwa plateau in east 2. ii. Plateau of Sailana 3. iii. Western hills of Sailana 4. iv. Chambal valley 5. v. Mahi valley 2. Major Drainage: 6. I. Ganga Basin (Chambal Sub Basin) 7. II. Mahi Basin 3. Land Use Ha (‘000) a) Forest area 34.30 b) Net area sown 333 c) Gross cropped area 500 4. Major Soil Types Sandy and black cotton soil. 5. Principal Crops Soyabean, wheat, maize, cotton, opium, gram. 6. Irrigation by Different Sources No. Area irrigated Ha(‘000) Dug wells 52213 32.67 Tube wells/Bore wells 18801 51.98 Tanks/Ponds 144 1.48 Canals 41 1.39 Other Sources - 4.79 7. Number 0f Ground Water Monitoring Wells of CGWB (As on 31.3.2013) Number of Dug Wells 24 Number of Piezometers 28 8 Predominant Geological Formations Alluvium, Deccan Trap basalts, Vindhyan shales and sandstone 9 Hydrogeology 2 Major Water Bearing Formation Sandy alluvium, Weathered/vesicular basalt, flow contacts and fractured sandstone. Pre-monsoon depth to water level range 2.70 to 23.40 m bgl during 2012 Post-monsoon depth to water level range 1.48 to 14.28 m bgl during 2012 Long-term water level trend in 10 years Pre monsoon (2003-2012) Rise: 6.20 – 10.74 cm/yr Fall : 3.64 – 30.90 cm/yr Post monsoon Rise: 11.82 cm/yr Fall : 2.00 – 36.44 cm/yr 10. -

Cfreptiles & Amphibians
WWW.IRCF.ORG/REPTILESANDAMPHIBIANSJOURNALTABLE OF CONTENTS IRCF REPTILES & AMPHIBIANSIRCF REPTILES • VOL 15,& NAMPHIBIANSO 4 • DEC 2008 •189 25(2):104-114 • AUG 2018 IRCF REPTILES & AMPHIBIANS CONSERVATION AND NATURAL HISTORY TABLE OF CONTENTS FEATURE ARTICLES Reptilian. Chasing Bullsnakes Diversity (Pituophis catenifer sayi) in Wisconsin: of the Bhopal Region in On the Road to Understanding the Ecology and Conservation of the Midwest’s Giant Serpent ...................... Joshua M. Kapfer 190 the State. The Shared Historyof of TreeboasMadhya (Corallus grenadensis) and HumansPradesh on Grenada: in Central India A Hypothetical Excursion ............................................................................................................................Robert W. Henderson 198 1* 2 1 RESEARCH ARTICLESAmit Manhas , Rajni Raina , and Ashwani Wanganeo . 1Department of EnvironmentalThe Texas Horned Sciences Lizard in andCentral Limnology, and Western Barkatullah Texas ....................... University, Emily Bhopal, Henry, Jason Madhya Brewer, Pradesh, Krista Mougey, India and (amitmanhas1986@gmail Gad Perry 204 .com) . The 2KnightDepartment Anole (Anolis of Zoology, equestris) inGovernment Florida Science and Commerce College, Bhopal, Madhya Pradesh, India .............................................Brian J. Camposano, Kenneth L. Krysko, Kevin M. Enge, Ellen M. Donlan, and Michael Granatosky 212 CONSERVATION ALERT Photographs by the senior author. World’s Mammals in Crisis ............................................................................................................................................................ -

IEE: India: SH-41: Agar-Barod-Alot-Jawra Project Road, Madhya Pradesh State Roads Project
Environmental Assessment Report Initial Environmental Examination for SH-41: Agar–Barod–Alot–Jawra Project Road Project Number: 43063 November 2010 IND: Madhya Pradesh State Roads Project III Prepared by Government of Madhya Pradesh for the Asian Development Bank (ADB). The initial environmental examination is a document of the borrower. The views expressed herein do not necessarily represent those of ADB’s Board of Directors, Management, or staff, and may be preliminary in nature. Table of Contents Executive Summary …………………………………………………………………………vii 1. INTRODUCTION 1 1.1. Project Background/Rationale .......................................................................... 1 1.2. Project Preparatory Technical Assistance (PPTA) and Environmental Assessment ................................................................................................................. 2 1.3. Purpose of the Study ....................................................................................... 2 1.4. Extent of IEE .................................................................................................... 3 1.5. IEE Content ..................................................................................................... 3 1.6. Team Composition and Acknowledgements .................................................... 3 1.7. Methodology .................................................................................................... 3 1.7.1. Information/ data Sources ...........................................................................