Cutaneous Manifestations of SLE and Other Connective Tissue Diseases
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Visual Recognition of Autoimmune Connective Tissue Diseases
Seeing the Signs: Visual Recognition of Autoimmune Connective Tissue Diseases Utah Association of Family Practitioners CME Meeting at Snowbird, UT 1:00-1:30 pm, Saturday, February 13, 2016 Snowbird/Alta Rick Sontheimer, M.D. Professor of Dermatology Univ. of Utah School of Medicine Potential Conflicts of Interest 2016 • Consultant • Paid speaker – Centocor (Remicade- – Winthrop (Sanofi) infliximab) • Plaquenil – Genentech (Raptiva- (hydroxychloroquine) efalizumab) – Amgen (etanercept-Enbrel) – Alexion (eculizumab) – Connetics/Stiefel – MediQuest • Royalties Therapeutics – Lippincott, – P&G (ChelaDerm) Williams – Celgene* & Wilkins* – Sanofi/Biogen* – Clearview Health* Partners • 3Gen – Research partner *Active within past 5 years Learning Objectives • Compare and contrast the presenting and Hallmark cutaneous manifestations of lupus erythematosus and dermatomyositis • Compare and contrast the presenting and Hallmark cutaneous manifestations of morphea and systemic sclerosis Distinguishing the Cutaneous Manifestations of LE and DM Skin involvement is 2nd most prevalent clinical manifestation of SLE and 2nd most common presenting clinical manifestation Comprehensive List of Skin Lesions Associated with LE LE-SPECIFIC LE-NONSPECIFIC Cutaneous vascular disease Acute Cutaneous LE Vasculitis Leukocytoclastic Localized ACLE Palpable purpura Urticarial vasculitis Generalized ACLE Periarteritis nodosa-like Ten-like ACLE Vasculopathy Dego's disease-like Subacute Cutaneous LE Atrophy blanche-like Periungual telangiectasia Annular Livedo reticularis -

Update on Vasculitis: Overview and Relevant
An Bras Dermatol. 2020;95(4):493---507 Anais Brasileiros de Dermatologia www.anaisdedermatologia.org.br REVIEW Update on vasculitis: overview and relevant dermatological aspects for the clinical and ଝ,ଝଝ histopathological diagnosis --- Part II a,∗ b Thâmara Cristiane Alves Batista Morita , Paulo Ricardo Criado , b a a Roberta Fachini Jardim Criado , Gabriela Franco S. Trés , Mirian Nacagami Sotto a Department of Dermatology, Hospital das Clínicas, Faculdade de Medicina, Universidade de São Paulo, São Paulo, SP, Brazil b Dermatology Discipline, Faculdade de Medicina do ABC, Santo André, SP, Brazil Received 8 December 2019; accepted 28 April 2020 Available online 24 May 2020 Abstract Vasculitis is a group of several clinical conditions in which the main histopathological KEYWORDS finding is fibrinoid necrosis in the walls of blood vessels. This article assesses the main derma- Anti-neutrophil tological aspects relevant to the clinical and laboratory diagnosis of small- and medium-vessel cytoplasmic cutaneous and systemic vasculitis syndromes. The most important aspects of treatment are also antibodies; discussed. Churg-Strauss © 2020 Sociedade Brasileira de Dermatologia. Published by Elsevier Espana,˜ S.L.U. This is an syndrome; open access article under the CC BY license (http://creativecommons.org/licenses/by/4.0/). Henoch-Schönlein purple; Leukocytoclastic cutaneous vasculitis; Systemic vasculitis; Vasculitis; Vasculitis associated with lupus of the central nervous system ଝ How to cite this article: Morita TCAB, Criado PR, Criado RFJ, Trés GFS, Sotto MN. Update on vasculitis: overview and relevant dermato- logical aspects for the clinical and histopathological diagnosis --- Part II. An Bras Dermatol. 2020;95:493---507. ଝଝ Study conducted at the Department of Dermatology, Faculdade de Medicina, Universidade de São Paulo, São Paulo, SP, Brazil. -

Update on Vasculitis: Overview and Relevant
An Bras Dermatol. 2020;95(4):493---507 Anais Brasileiros de Dermatologia www.anaisdedermatologia.org.br REVIEW Update on vasculitis: overview and relevant dermatological aspects for the clinical and ଝ,ଝଝ histopathological diagnosis --- Part II a,∗ b Thâmara Cristiane Alves Batista Morita , Paulo Ricardo Criado , b a a Roberta Fachini Jardim Criado , Gabriela Franco S. Trés , Mirian Nacagami Sotto a Department of Dermatology, Hospital das Clínicas, Faculdade de Medicina, Universidade de São Paulo, São Paulo, SP, Brazil b Dermatology Discipline, Faculdade de Medicina do ABC, Santo André, SP, Brazil Received 8 December 2019; accepted 28 April 2020 Available online 24 May 2020 Abstract Vasculitis is a group of several clinical conditions in which the main histopathological KEYWORDS finding is fibrinoid necrosis in the walls of blood vessels. This article assesses the main derma- Anti-neutrophil tological aspects relevant to the clinical and laboratory diagnosis of small- and medium-vessel cytoplasmic cutaneous and systemic vasculitis syndromes. The most important aspects of treatment are also antibodies; discussed. Churg-Strauss © 2020 Sociedade Brasileira de Dermatologia. Published by Elsevier Espana,˜ S.L.U. This is an syndrome; open access article under the CC BY license (http://creativecommons.org/licenses/by/4.0/). Henoch-Schönlein purple; Leukocytoclastic cutaneous vasculitis; Systemic vasculitis; Vasculitis; Vasculitis associated with lupus of the central nervous system ଝ How to cite this article: Morita TCAB, Criado PR, Criado RFJ, Trés GFS, Sotto MN. Update on vasculitis: overview and relevant dermato- logical aspects for the clinical and histopathological diagnosis --- Part II. An Bras Dermatol. 2020;95:493---507. ଝଝ Study conducted at the Department of Dermatology, Faculdade de Medicina, Universidade de São Paulo, São Paulo, SP, Brazil. -

Dermatological Indications of Disease - Part II This Patient on Dialysis Is Showing: A
“Cutaneous Manifestations of Disease” ACOI - Las Vegas FR Darrow, DO, MACOI Burrell College of Osteopathic Medicine This 56 year old man has a history of headaches, jaw claudication and recent onset of blindness in his left eye. Sed rate is 110. He has: A. Ergot poisoning. B. Cholesterol emboli. C. Temporal arteritis. D. Scleroderma. E. Mucormycosis. Varicella associated. GCA complex = Cranial arteritis; Aortic arch syndrome; Fever/wasting syndrome (FUO); Polymyalgia rheumatica. This patient missed his vaccine due at age: A. 45 B. 50 C. 55 D. 60 E. 65 He must see a (an): A. neurologist. B. opthalmologist. C. cardiologist. D. gastroenterologist. E. surgeon. Medscape This 60 y/o male patient would most likely have which of the following as a pathogen? A. Pseudomonas B. Group B streptococcus* C. Listeria D. Pneumococcus E. Staphylococcus epidermidis This skin condition, erysipelas, may rarely lead to septicemia, thrombophlebitis, septic arthritis, osteomyelitis, and endocarditis. Involves the lymphatics with scarring and chronic lymphedema. *more likely pyogenes/beta hemolytic Streptococcus This patient is susceptible to: A. psoriasis. B. rheumatic fever. C. vasculitis. D. Celiac disease E. membranoproliferative glomerulonephritis. Also susceptible to PSGN and scarlet fever and reactive arthritis. Culture if MRSA suspected. This patient has antithyroid antibodies. This is: • A. alopecia areata. • B. psoriasis. • C. tinea. • D. lichen planus. • E. syphilis. Search for Hashimoto’s or Addison’s or other B8, Q2, Q3, DRB1, DR3, DR4, DR8 diseases. This patient who works in the electronics industry presents with paresthesias, abdominal pain, fingernail changes, and the below findings. He may well have poisoning from : A. lead. B. -

Conflict of Interest Cutaneous Vasculitis
Cutaneous Vasculitis: Texas Dermatologic Society 2018 Joseph L. Jorizzo, MD Professor, Former and Founding Chair Department of Dermatology Wake Forest School of Medicine Winston-Salem, NC – USA Professor of Clinical Dermatology Department of Dermatology Weill Cornell Medical College New York, NY - USA Conflict of Interest Amgen – Advisory Board – Honoraria Cutaneous Vasculitis Key Features Cutaneous signs of vasculitis are a reflection of the size of the vessels involved Vasculitis can be limited to the small vessels of the skin or it can be a sign of life-threatening internal organ invovlement The clinical diagnosis of cutaneous vasculitis requires histopathologic confirmation and multiple biopsies may be required 1 Vasculitis: 2018 Classification Problems: The example of the ACR Criteria Age at disease onset > 16 years Medication at disease onset Palpable purpura Biopsy including arteriole and venule with histologic change showing granulocytes in perivascular or extravascular location Three criteria are required ARTHRITIS & RHEUMATISM Vol. 65, No.1, Jan 2013, pp1-11 DOI 10.1002/art37715 2013, American College of Rheumatology Arthritis & Rheumatism An Official Journal of the American College of Rheumatology www.arthritisheum.org and wileyonlinelibrary.com SPECIAL ARTICLE 2012 Revised International Chapel Hill Consensus Conference Nomenclature of Vasculitides J.C. Jennette, 1 R.J. Falk, 1, P.A. Bacon,2 N. Basu,3 M.C. Cid,4 F. Ferrario, 5 L.F. Flores-Suarez,6 W.L. Gross,7 L. Guillevin,8 E.C. Hagen,9 G.S. Hoffman,10 D.R. Jayne,11 C.G.M. Kallenberg,12 P. Lamprecht,13 C.A. Langford,10 R. A. Luqmani,14 A. D. Mahr, 15 E.L. -

Striae Distensae
COMPARATIVE STUDY BETWEEN INTENSE PULSED LIGHT "IPL" AND PULSED DYE LASER IN THE TREATMENT OF STRIAE DISTENSAE Thesis Submitted for the Fulfillment of (Ph.D) Degree in Medical Applications of Laser By By Ghada Mohamed Kamal El-Din Ahmed El-Khalafawy (M.B.B.Ch., M.Sc.) & Diploma in Medical Laser Applications Under the supervision of Prof. Dr. Hisham Ali Shokeir Professor of Dermatology National Institute of Laser Enhanced Sciences – Cairo University Ass. Prof. Dr. Ahmed Fathy El-Bedewi Associate Professor of Dermatology Atomic Energy Authority Ass. Prof. Dr. Safinaz Salah El-Din Sayed Associate Professor of Histology Faculty of Medicine – Cairo University National Institute of Laser Enhanced Sciences Cairo University 2013 Approval Sheet COMPARATIVE STUDY BETWEEN INTENSE PULSED LIGHT "IPL" AND PULSED DYE LASER IN THE TREATMENT OF STRIAE DISTENSAE Thesis Submitted for the Fulfillment of (Ph.D) Degree in Medical Applications of Laser By By Ghada Mohamed Kamal El-Din Ahmed El-Khalafawy (M.B.B.Ch., M.Sc.) & Diploma in Medical Laser Applications Under the supervision of Prof. Dr. Hisham Ali Shokeir Ass. Prof. Dr. Ahmed Fathy El-Bedewi Ass. Prof. Dr. Safinaz Salah El-Din Sayed National Institute of Laser Enhanced Sciences Cairo University 2013 ﷲ ا ا ُ ْ ََ ُاا ُُ ْْ ََ َ َ ََ ََ ِِ ْ ََََ ََ ﱠﱠ ﱠﱠ ﱠﱠ ََ ْْ ِ ِ إإ ََ َ َ ْْ َ َ َ َ ََِِإإ ََأأ ََ ِِ ُُاا ْْ ََ ِِ ُاا ُ ق ﷲ ا رة اة ا ( 32) Acknowledgment I am deeply thankful to GODGOD, by the grace of whom, the present work was possible. -

Reticulate Dermatoses
[Downloaded free from http://www.e-ijd.org on Tuesday, April 08, 2014, IP: 111.93.251.154] || Click here to download free Android application for this journal CME Article Reticulate Dermatoses Keshavmurthy A Adya, Arun C Inamadar, Aparna Palit From the Department of Dermatology, Venereology and Leprosy, SBMP Medical College, Hospital and Research Center, BLDE University, Bijapur, Karnataka, India Abstract The term “reticulate” is used for clinical description of skin lesions that are configured in a net-like pattern. Many primary and secondary dermatoses present in such patterns involving specific body sites. Certain cutaneous manifestations of systemic diseases or genodermatoses also present in such manner. This review classifies and describes such conditions with reticulate lesions and briefly, their associated features. Key Words: Mottling, net-like, reticulate, retiform What was known? 3. Poikilodermatous Reticulate configuration of lesions is seen in many primary dermatoses and a. Inherited also as cutaneous reaction patterns consequent to internal pathology. • Rothmund–Thomson syndrome • Dyskeratosis congenita Reticulate Dermatoses • Xeroderma pigmentosum • Cockayne syndrome The term “reticulate” is commonly used for clinical • Fanconi anemia description of “net-like”, “sieve-like,” or “chicken wire” • Mendes da Costa syndrome configuration of the skin lesions. Various congenital • Kindler syndrome and acquired dermatoses present with this pattern of • Degos–Touraine syndrome skin lesions. Many systemic diseases also present with • Hereditary sclerosing poikiloderma of Weary such cutaneous manifestations providing useful clues to • Hereditary acrokeratotic poikiloderma of Weary diagnosis. • Werner’s syndrome (adult progeria) Classification • Chanarin–Dorfman syndrome • Diffuse and macular atrophic dermatosis 1. Vascular b. Acquired a. Cutis marmorata • Poikiloderma of Civatte b. -

Atrophic Erythematous Facial Plaques
Photo Challenge Atrophic Erythematous Facial Plaques What’s the diagnosis? A 26-year-old woman presented with a 2-year his- tory of facial lesions that had gradually increased in size and number. Initially they were tender and pruritic but eventually became asymptomatic. She denied aggravation with sun exposure and did not use regular sun protection. Multiple pulsed dye laser treatments to the lesions had not resulted in appreciable improvement. Review of systems revealed occasional blurred vision and joint pain in her wrist and fingers of her right hand. Physical examination revealed a healthy- CUTISappearing woman. On the forehead and bilateral cheeks there were multiple atrophic, erythematous, sunken plaques with discrete borders. Each plaque measured more than 5 mm. Similar plaques were scattered across the frontal scalp, trunk, and upper extremities, though fewer in number and less atrophic with mild hyperpigmentation. There was diffuse hair thinning of the scalp. Laboratory test results included a normal complete metabolic panel, anti- nuclear antibody profile, and complete blood cell count. DoHistopathology revealed Not a superficial and mid perivascular Copy and perifollicular inflammatory infiltrate composed of lymphocytes, histiocytes, and melanophages. Vacuolar changes in the dermoepidermal junction were present. There were few dyskeratotic keratinocytes and mucin deposition present in the dermis. Direct immunofluorescence was not performed. William S. Kaufman, MD; Elizabeth K. McNamara, MD; Rita Pichardo-Geisinger, MD From Wake Forest University Baptist Medical Center, Winston-Salem, North Carolina. The authors report no conflict of interest. Correspondence: William S. Kaufman, MD, Wake Forest University Baptist Medical Center, Department of Dermatology, Medical Center Boulevard, Winston-Salem, NC 27157 ([email protected]). -

Resident's Page
Resident’s Page SScarscars iinn ddermatology:ermatology: CClinicallinical signisignifi ccanceance BB.. AAnitha,nitha, SS.. RRagunatha,agunatha, AArunrun CC.. IInamadarnamadar Department of Dermatology, Venereology and Leprosy, BLDEA’s SBMP Medical College, Hospital and Research Centre, Bijapur, Karnataka, India AAddressddress fforor ccorrespondenceorrespondence : Dr. Arun C. Inamadar, Professorand Head, Department of Dermatology, Venereology and Leprosy, BLDEA’s SBMP Medical College, Hospital and Research Centre, Bijapur - 586103, Karnataka, India. E-mail:[email protected] [2] A scar is a scar is a scar and only a scar if you don’t ask ß1 protects the collagen from degradation. why” - Shelly and Shelly CCLASSIFICATIONLASSIFICATION OOFF SSCARSCARS[[3]3] A scar is a fibrous tissue replacement that develops as a 1. Fine line scars: Surgical scars consequence of healing at the site of a prior ulcer or 2. Wide (stretched) scars: These develop when fine wound. Cutaneous scarring is a macroscopic disturbance of line surgical scars gradually become stretched the normal structure and function of the skin architecture and widened. They are typically flat, pale, soft, manifesting itself as an elevated or depressed area, with an symptomless scars. Abdominal striae of pregnancy alteration of skin texture, color, vascularity, nerve supply can be considered as variants of these. [1] and biomechanical properties. 3. Atrophic scars: These are flat or depressed below the surrounding skin. They are generally small and Histologically, dermal scars are characterized by thickened often round with an indented or inverted centre. epidermis with a flattened dermo-epidermal junction and They commonly arise after acne or chickenpox. an abnormal organization of the dermal matrix into parallel 4. -
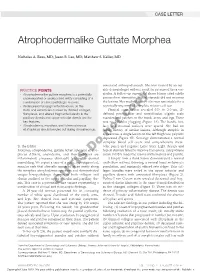
Atrophodermalike Guttate Morphea
CASE LETTER Atrophodermalike Guttate Morphea Nicholas A. Ross, MD; Jason B. Lee, MD; Matthew S. Keller, MD associated arthropod assault. She was treated by an out- PRACTICE POINTS side dermatologist without result for presumed tinea ver- • Atrophodermalike guttate morphea is a potentially sicolor. A follow-up superficial shave biopsy cited subtle underreported or undescribed entity consisting of a psoriasiform dermatitis. Topical steroids did not improve combination of clinicopathologic features. the lesions. Her medical history also was remarkable for a • Widespread hypopigmented macules on the reportedly unprovoked complete rotator cuff tear. trunk and extremities marked by thinned collagen, Physical examination revealed 0.5- to 2.0-cm, ill- fibroplasia, and altered fragmented elastin in the defined, perifollicular and nonfollicular, slightly scaly papillary dermis and upper reticular dermis are the macules and patchescopy on the trunk, arms, and legs. There key features. was no follicular plugging (Figure 1A). The hands, feet, • Atrophoderma, morphea, and lichen sclerosus face, and mucosal surfaces were spared. She had no et atrophicus should be ruled out during clinical workup. family history of similar lesions. Although atrophic in appearance, a single lesion on the left thigh was palpably depressednot (Figure 1B). Serology demonstrated a normal complete blood cell count and comprehensive meta- To the Editor: bolic panel, and negative Lyme titers. Light therapy and Morphea, atrophoderma, guttate lichen sclerosus et atro- topical steroids failed to improve the lesions; calcipotriene phicus (LS&A), anetoderma, and their subtypesDo are cream 0.005% made the lesions erythematous and pruritic. inflammatory processes ultimately leading to dermal A biopsy from a flank lesion demonstrated a normal remodeling. -

Boards' Fodder
boards’ fodder Sound-alikes in dermatology by Jeffrey Kushner, DO, and Kristen Whitney, DO Disease Entity Description Actinic granuloma/ Annular elastolytic Variant of granuloma annulare on sun-damaged skin; annular erythematous giant cell granuloma plaques with slightly atrophic center in sun-exposed areas, which may be precipi- tated by actinic damage. Actinic prurigo PMLE-like disease with photodistributed erythematous papules or nodules and hemorrhagic crust and excoriation. Conjunctivitis and cheilitis are commonly found. Seen more frequently in Native Americans (especially Mestizos). Actinomycetoma “Madura Foot”; suppurative infection due to Nocaria, Actinomadura, or Streptomyces resulting in tissue tumefaction, draining sinuses and extrusion of grains. Actinomycosis “Lumpy Jaw”; Actinomyces israelii; erythematous nodules at the angle of jaw leads to fistulous abscess that drain purulent material with yellow sulfur granules. Acrokeratosis verruciformis Multiple skin-colored, warty papules on the dorsal hands and feet. Often seen in conjunction with Darier disease. Acrodermatitis enteropathica AR; SLC39A4 mutation; eczematous patches on acral, perineal and periorificial skin; diarrhea and alopecia; secondary to zinc malabsorption. Atrophoderma 1) Atrophoderma vermiculatum: Pitted atrophic scars in a honeycomb pattern around follicles on the face; associated with Rombo, Nicolau-Balus, Tuzun and Braun-Falco-Marghescu syndromes. 2) Follicular atrophoderma: Icepick depressions at follicular orifices on dorsal hands/feet or cheeks; associated with Bazex-Dupré-Christol and Conradi- Hünermann-Happle syndromes. 3) Atrophoderma of Pasini and Pierini: Depressed patches on the back with a “cliff-drop” transition from normal skin. 4) Atrophoderma of Moulin: Similar to Pasini/Pierini, except lesions follow the lines of Blaschko. Anetoderma Localized area of flaccid skin due to decreased or absent elastic fibers; exhibits “buttonhole” sign. -
2014 Slide Library Case Summary Questions & Answers With
2014 Slide Library Case Summary Questions & Answers with Discussions 51st Annual Meeting November 6-9, 2014 Chicago Hilton & Towers Chicago, Illinois The American Society of Dermatopathology ARTHUR K. BALIN, MD, PhD, FASDP FCAP, FASCP, FACP, FAAD, FACMMSCO, FASDS, FAACS, FASLMS, FRSM, AGSF, FGSA, FACN, FAAA, FNACB, FFRBM, FMMS, FPCP ASDP REFERENCE SLIDE LIBRARY November 2014 Dear Fellows of the American Society of Dermatopathology, The American Society of Dermatopathology would like to invite you to submit slides to the Reference Slide Library. At this time there are over 9300 slides in the library. The collection grew 2% over the past year. This collection continues to grow from member’s generous contributions over the years. The slides are appreciated and are here for you to view at the Sally Balin Medical Center. Below are the directions for submission. Submission requirements for the American Society of Dermatopathology Reference Slide Library: 1. One H & E slide for each case (if available) 2. Site of biopsy 3. Pathologic diagnosis Not required, but additional information to include: 1. Microscopic description of the slide illustrating the salient diagnostic points 2. Clinical history and pertinent laboratory data, if known 3. Specific stain, if helpful 4. Clinical photograph 5. Additional note, reference or comment of teaching value Teaching sets or collections of conditions are especially useful. In addition, infrequently seen conditions are continually desired. Even a single case is helpful. Usually, the written submission requirement can be fulfilled by enclosing a copy of the pathology report prepared for diagnosis of the submitted case. As a guideline, please contribute conditions seen with a frequency of less than 1 in 100 specimens.