Views on Flight Safety Check Six from the Flight Surgeon
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

A-Cr-Ccp-803/Pf-001 Chapter 11 Po 320
A-CR-CCP-803/PF-001 CHAPTER 11 PO 320 – PARTICIPATE IN CANADIAN FORCES (CF) FAMILIARIZATION ACTIVITIES A-CR-CCP-803/PF-001 ROYAL CANADIAN AIR CADETS PROFICIENCY LEVEL THREE INSTRUCTIONAL GUIDE SECTION 1 EO M320.01 – DESCRIBE THE ROLE OF CANADA’S AIR FORCE Total Time: 30 min PREPARATION PRE-LESSON INSTRUCTIONS Resources needed for the delivery of this lesson are listed in the lesson specification located in A-CR-CCP- 803/PG-001, Chapter 4. Specific uses for said resources are identified throughout the instructional guide within the TP for which they are required. Review the lesson content and become familiar with the material prior to delivering the lesson. Update the information sheets located at Annexes A to D using the reference. Photocopy the updated information sheets, ensuring there is one copy at the learning stations for each cadet in the largest group. Photocopy the worksheet located at Annex E for each cadet in the class. PRE-LESSON ASSIGNMENT N/A. APPROACH An in-class activity was chosen for TP 1 as it is an interactive way to present the role of Canada’s air force and stimulate interest among cadets. A group discussion was chosen for TP 2 as it allows the cadets to interact with their peers and share their knowledge, experiences, opinions, and feelings about Canada’s air force. INTRODUCTION REVIEW N/A. OBJECTIVES By the end of this lesson the cadet shall have described the role of Canada’s air force. IMPORTANCE It is important for cadets to know the role of Canada’s air force. -
RSAF Best UNITS OTHER FEATURES : SAF DAY 2017 | Ex Maple Flag ISSUE NO
Republic of Singapore FULL SPECTRUM . INTEGRATED . READY Issue No. 146 2017 RSAF bEST UNITS OTHER FEATURES : SAF DAY 2017 | ex maple flag ISSUE NO. 146 / 2017 AFN MANAGEMENT COMMITTEE Chairman COL Lim Kok Siong Members LTC Cindy Chua LTC Lily Foo LTC Koh Boon Tih RSAF Best Unit Competition LTC Cecilia Ong PG 4 LTC Tan Giam LTC Michael Wong Ms Heng Ai Buay Ms Loh Seok Chen Editors LTC Melvyn Tan LTC Charles Chua Assistant Editor CPT Seow Feng Chang Staff Writers & Photographers CPL Christopher Tan CPL Ivan Chua CPL Samuel Chua PG 12 SAF Day 2017 REC Bradley Gerard REC Sng Qiyang REC Darren Tan The opinions and views herein are those expressed by the writers and do not necessarily reflect the Pg 4 — 11 official views of the Republic of Singapore Air Force (RSAF) or the Ministry of Defence. The material in Pg 12 — 13 Air Force News is not to be reproduced in whole or Pg 14 — 16 in part without the written consent of the RSAF. Pg 17 We Value Your Feedback! Pg 18 — 19 If you have any feedback or comments about Air Force News, please email Pg 19 — 25 [email protected] Pg 26 — 30 Like Us on Facebook! Pg 31 Facebook.com/TheRSAF Pg 32 Follow Us on Pg 33 Twitter & Instagram! EX Maple Flag Pg 34 — 35 @TheRSAF | #TheRSAF PG 14 Pg 35 2 FEATURED WRITERS Sultan of Brunei CDF Visit to 1 AELG Pg 18 Visit Pg 19 – CPL Samuel Chua – s an aviation enthusiast, being able to Adocument the RSAF in action has been a dream come true to me. -

Air & Space Power Journal
Chief of Staff, US Air Force Gen John P. Jumper Commander, Air Education and Training Command Gen Donald G. Cook http://www.af.mil Commander, Air University Lt Gen John F. Regni Commandant, College of Aerospace Doctrine, Research and Education Col David S. Fadok Editor Lt Col Paul D. Berg Senior Editor Lt Col Malcolm D. Grimes http://www.aetc.randolph.af.mil Associate Editor Maj Donald R. Ferguson Editor and Military Defense Analyst Col Larry Carter, USAF, Retired Professional Staff Marvin W. Bassett, Contributing Editor Philip S. Adkins, Contributing Editor Debbie Banker, Editorial Assistant Sherry Terrell, Editorial Assistant Steven C. Garst, Director of Art and Production Daniel M. Armstrong, Illustrator http://www.au.af.mil L. Susan Fair, Illustrator Ann Bailey, Prepress Production Manager Air and Space Power Chronicles Luetwinder T. Eaves, Managing Editor The Air and Space Power Journal, published quarterly, is the professional flagship publication of the United States Air Force. It is designed to serve as an open forum for the presentation and stimulation of innova tive thinking on military doctrine, strategy, tactics, http://www.cadre.maxwell.af.mil force structure, readiness, and other matters of na tional defense. The views and opinions expressed or implied in the Journal are those of the authors and should not be construed as carrying the official sanc tion of the Department of Defense, Air Force, Air Education and Training Command, Air University, or other agencies or departments of the US government. Articles in this edition may be reproduced in whole or Visit Air and Space Power Journal online in part without permission. -

AIR FORCE RENAISSANCE? Canada Signals a Renewed Commitment to Military Funding THINK CRITICAL MISSIONS
an MHM PUBLisHinG MaGaZine 2017 edition Canada’s air ForCe review BroUGHt to yoU By www.skiesMaG.CoM [INSIDE] RCAF NEWS YEAR IN REVIEW RETURN TO THE “BIG 2” BAGOTVILLE’S 75TH FLYING RED AIR VINTAGE WINGS RESET AIR FORCE RENAISSANCE? CANADA SIGNALS A RENEWED COMMITMENT TO MILITARY FUNDING THINK CRITICAL MISSIONS Equipped with cutting edge technology, all weather capability and unrivaled precision and stability in the harshest environments. Armed with the greatest endurance, longest range and highest cruise speed in its class. With maximum performance and the highest levels of quality, safety and availability to ensure success for demanding search and rescue operations - anywhere, anytime. H175 - Deploy the best. Important to you. Essential to us. RCAF Today 2017 1 Mike Reyno Photo 32 A RENAISSANCE FOR THE RCAF? The Royal Canadian Air Force appears to be headed for a period of significant renewal, with recent developments seeming to signal a restored commitment to military funding. By Martin Shadwick 2 RCAF Today 2017 2017 Edition | Volume 8 42 IN THIS ISSUE 62 20 2016: MOMENTS AND 68 SETTING HIGH STANDARDS MILESTONES The many important “behind the scenes” elements of the Canadian Forces The RCAF met its operational Snowbirds include a small group of 431 commitments and completed a number Squadron pilots known as the Ops/ of important functions, appearances and Standards Cell and the Tutor SET. historical milestones in 2016. Here, we revisit just a few of the year’s happenings. By Mike Luedey 30 MEET THE CHIEF 72 PLANES AND PASSION RCAF Chief Warrant Officer Gérard Gatineau’s Vintage Wings is soaring Poitras discusses his long and satisfying to new heights, powered by one of its journey to the upper ranks of the greatest assets—the humble volunteer. -

IPMS Canada RT
IPMS Canada RT (Random Thoughts) Index Maintained by: Fred Hutcheson C5659 List by Category and Subject snail: Box 626, Station B, Ottawa, ON K1P 5P7 e-mail: [email protected] Saturday, April 2, 2016 web: www.ipmscanada.com Page 1 of 51 IPMS Canada - RT Index - List by Category and Subject Volume Subject Designation Country Comments Category: aircraft 1603 184 Shorts Type 184r UK Airframe vf kit @1:72 3104 40B Boeing40B-4a USA build CMR 1:72 resin kit 0028 504 Avro 504a UK Cdn mkgs (Golden Centennaires) 0412 504 Avro 504a UK Nightfighter mkgs 0606 504 Avro 504Ka UK Swedish mkgs - 1919 0606 504 Avro504a UK Cdn mkgs, 1920-28 0611 504 Avro 504Ka UK Civil mkgs - 1918 0905 504 Avro 504a UK 0906 504 Avro 504a UK 0909 552 Avro 552a UK 2305 707 Boeing707r Canada Leading Edge decals & refuel pod 1:72 0809 707/720 Boeing 720a USA Civil mkgs 0202 707/C-135 Boeing C-135a USA Civil Federal Aviation Adm mkgs 2306 707/C-135 Boeing KC-135r USA Detail & Scale book 2603 707/E-3 Boeing E-3 Sentrya USA building Airfix kit @1/72 0612 727 Boeing727a USA Cdn civil mkgs 0612 737 Boeing737a USA Cdn civil mkgs 0711 737 Boeing T-43a USA USAF trainer mkgs 1504 737 Boeing 737r USA Maquettes M&B kit @1:100 2303 737 Boeing 737-300a USA markings for several airliners 2706 737 Boeing 737-200r USA JBOT decals for ZIP Air @ 1:200 1704 747 Boeing 747r USA book on history & photos of the type 0210 A 143 Amiot143a France Int dwg 1901 A-1 Morane A-1a France Formaplane vacuform 0702 A-2 Spad A-2a UK Conv Spad S 7 to A 2 0704 A-7 Anotov A-7a USSR Detail dwgs, 2002 Access -

Ball Hockey on the Jetty
173043 Monday, August 26, 2019 Volume 53, Issue 17 www.tridentnewspaper.com Ball hockey on the jetty Sailors from HMCS Halifax made time for a game of ball hockey during a recent port visit to Lisbon, Portugal. The ship is currently deployed to Op REASSUR- ANCE as the flagship of SNMG2. CPL BRADEN TRUDEAU, FIS New exhibit at Naval National Peacekeepers' HMCS Goose Bay back Highlights from Op Museum Pg. 3 Day ceremony Pg. 7 from Caribbean Pg. 10 REASSURANCE Pg. 14 We have all your shopping needs. VISIT WINDSOR PARK Now Open SUNDAYS 1200 - 1700 CANEX.ca 173039 2 TRIDENT NEWS AUGUST 26, 2019 Vice Admiral’s flag hoist signal S I assume command from my After all, you, today’s sailors, are an Our status as a long-time shipmate, Vice impressive lot to command: inspired Forbes-recognized best Admiral Ron Lloyd, I am equally by a rich history and the bright Canadian employer humbled and honoured to future that the ongoing largest peace- depends upon it. followA in the wake of the admirals that time fleet recapitalization in our history Our shipmates preceded me upon being chosen as your ensures. depend upon it. 36th commander. You are equal parts warrior and dip- Those whom we serve lomat as you inspire with the depth depend upon it. and breadth of your successes alongside As we look to the partners and allies at home and around future, shipmates, the the globe; as you routinely combat cri- “how” behind what ses - man-made or naturally occurring; as we do will continue to you ensure that you remain ready to help, matter enormously. -

An Examination of the RCAF's Simulation Strategy 2025
AN EXAMINATION OF THE RCAF’S SIMULATION STRATEGY 2025 Maj J.A. Bowser JCSP 42 PCEMI 42 Service Paper Étude militaire Disclaimer Avertissement Opinions expressed remain those of the author and Les opinons exprimées n’engagent que leurs auteurs do not represent Department of National Defence or et ne reflètent aucunement des politiques du Canadian Forces policy. This paper may not be used Ministère de la Défense nationale ou des Forces without written permission. canadiennes. Ce papier ne peut être reproduit sans autorisation écrite. © Her Majesty the Queen in Right of Canada, as © Sa Majesté la Reine du Chef du Canada, représentée par represented by the Minister of National Defence, 2016. le ministre de la Défense nationale, 2016. CANADIAN FORCES COLLEGE – COLLÈGE DES FORCES CANADIENNES JCSP 42 – PCEMI 42 2015 – 2016 JCSP SERVICE PAPER – PCEMI ÉTUDE MILITAIRE AN EXAMINATION OF THE RCAF’S SIMULATION STRATEGY 2025 Maj J.A. Bowser “This paper was written by a student “La présente étude a été rédigée par un attending the Canadian Forces College stagiaire du Collège des Forces in fulfilment of one of the requirements canadiennes pour satisfaire à l'une des of the Course of Studies. The paper is a exigences du cours. L'étude est un scholastic document, and thus contains document qui se rapporte au cours et facts and opinions, which the author contient donc des faits et des opinions alone considered appropriate and que seul l'auteur considère appropriés et correct for the subject. It does not convenables au sujet. Elle ne reflète pas necessarily reflect the policy or the nécessairement la politique ou l'opinion opinion of any agency, including the d'un organisme quelconque, y compris le Government of Canada and the gouvernement du Canada et le ministère Canadian Department of National de la Défense nationale du Canada. -

Mission Ready: Canada's Role in the Kosovo Air Campaign
by Lieutenant-Colonel David L. Bashow, Colonel Dwight Davies, Colonel André Viens, Lieutenant-Colonel John Rotteau, Major Norman Balfe, Major Ray Stouffer, Captain James Pickett and Dr. Steve Harris Canadian Forces Photo by: MCpl Danielle Bernier MISSION READY: CANADA’S ROLE IN THE KOSOVO AIR CAMPAIGN n 24 March, 1999, just before midnight ning of the most extensive Canadian Air Force combat Adriatic time, four CF 18 Hornets operation since the Persian Gulf War of 1991. Over the launched from Aviano Air Base in Italy en- ensuing 78 days and nights, the six, then twelve, then route to a pre-planned target located in eighteen Canadian CF 18s from Aviano flew a total of Kosovo. These Canadian tactical fighters 678 combat sorties over nearly 2600 flying hours. They Owere four of sixteen dedicated bombing aircraft situated delivered 532 bombs — nearly half a million pounds of in the centre of a much larger strike package of NATO high explosive munitions — including 361 of the laser- aircraft — Electronic Warfare (EW), Suppression of guided five-hundred and two-thousand-pound variants Enemy Air Defences (SEAD) and fighter escort aircraft. on a variety of targets throughout Kosovo and the Communications jammers, Airborne Command, Control Federal Republic of Yugoslavia, all without loss to par- and Communications (ABCCC), air-to-air refueling ticipating Canadian aircrew and aircraft.1 This article tankers and Airborne Warning and Control (AWACS) will highlight the Canadian air operations over Kosovo, aircraft provided additional vital support. The Canadian along with the lessons learned during the air campaign Hornets of Task Force Aviano successfully navigated to and their implications for future planning and operations. -
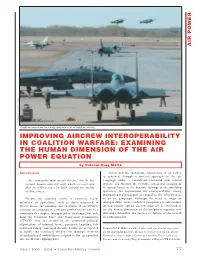
Improving Aircrew Interoperability in Coalition Warfare: Examining the Human Dimension of the Air Power Equation
AIR POWER DND photo CK2004-0179-13d Coalition operations frequently generate a lot of flightline activity. IMPROVING AIRCREW INTEROPERABILITY IN COALITION WARFARE: EXAMINING THE HUMAN DIMENSION OF THE AIR POWER EQUATION by Colonel Greg Matte Introduction Given that the maximum exploitation of air power is achieved through a unified approach to the air ...the commander must accept the fact that he has campaign under a centralized command and control certain human material with which to work and system, and through the flexible, integrated assignment that everything must be built around the reality of tactical forces to the dynamic taskings of the unfolding of these forces...1 operation, the requirement for interoperability among multinational participants is crucial to the effectiveness Despite the stunning results of relatively recent of an air campaign. Although the need to focus on offensive air operations, such as those witnessed in interoperability from a technical perspective is self-evident, Desert Storm, the planning and execution of an effective interoperability among aircrew must not be overlooked, coalition air campaign in a modern combat theatre can be a for the human dimension of the air power equation will tremendously complex interoperability challenge. Not only ultimately determine the success or failure of the overall must the Coalition Force Air Component Commander air campaign plan. (CFACC) bear the weight of the combined political expectations of minimal losses, precision targeting, low collateral damage and rapid decisive results, he is expected Colonel G.C.P. Matte is a CF-18 pilot with operational experience to rapidly and seamlessly integrate the disparate elements on UN and NATO missions. -

Canadian Air Power and Censorship During the Kosovo War
University of Calgary PRISM: University of Calgary's Digital Repository University of Calgary Press University of Calgary Press Open Access Books 2019-02 Scattering Chaff: Canadian Air Power and Censorship during the Kosovo War Bergen, Bob University of Calgary Press http://hdl.handle.net/1880/109501 book https://creativecommons.org/licenses/by-nc-nd/4.0 Attribution Non-Commercial No Derivatives 4.0 International Downloaded from PRISM: https://prism.ucalgary.ca SCATTERING CHAFF: Canadian Air Power and Censorship during the Kosovo War by Bob Bergen ISBN 978-1-77385-031-3 THIS BOOK IS AN OPEN ACCESS E-BOOK. It is an electronic version of a book that can be purchased in physical form through any bookseller or on-line retailer, or from our distributors. Please support this open access publication by requesting that your university purchase a print copy of this book, or by purchasing a copy yourself. If you have any questions, please contact us at [email protected] Cover Art: The artwork on the cover of this book is not open access and falls under traditional copyright provisions; it cannot be reproduced in any way without written permission of the artists and their agents. The cover can be displayed as a complete cover image for the purposes of publicizing this work, but the artwork cannot be extracted from the context of the cover of this specific work without breaching the artist’s copyright. COPYRIGHT NOTICE: This open-access work is published under a Creative Commons licence. This means that you are free to copy, distribute, display or perform the work as long as you clearly attribute the work to its authors and publisher, that you do not use this work for any commercial gain in any form, and that you in no way alter, transform, or build on the work outside of its use in normal academic scholarship without our express permission. -

F-22 Raptor Team Checks out Cold Lake Air Show Site
Welcome to Cold Lake STEAK NIGHT Fridays at the Cold Lake Branch 211 Call 780-639-3579 Volume 51 Number 24 www.couriernews.ca June 19, 2018 F-22 Raptor team checks out Cold Lake Air Show site JEFF GAYE Three members of the United States Air Force F-22 Raptor demonstration team were in Cold Lake last week to do a site survey before their performance at this summer’s Cold Lake Air Show. They checked in with air show organizers, and inspected 4 Wing’s security and service infrastructure. Maj Paul “Loco” Lopez, Tech Sgt Yamil Reyes Sanchez and Master Sgt Jamie Fleming were pleased with what they saw in Cold Lake. Maj Lopez, the F-22 pilot, said air show audiences can expect an exciting experience from the Raptor demonstration. “I think the audience experience is very exhilarating,” he said. “There’s just a sense of pride and joy at seeing how far technology has come and how the F-22 Raptor essentially defies the laws of gravity and aerodynamics for some of the manoeuvres we perform. I mean, we can do this now. Imagine what we can do in 10, 15, 20 years from now.” Maj Lopez caught the aviation bug Jeff Gaye Master Sgt Jamie Fleming, Maj “Loco” Lopez and Tech Sgt Yamil Reyes Sanchez came for a look at 4 Wing in early in his life. “It was growing up as a advance of July’s Cold Lake Air Show. little kid,” he said. “I grew up near a military base what my goals were, to help me get on six months now, and to this day it’s like “Whether you live right down similar to the local Cold Lake the path to becoming a fighter pilot. -

December 2016 - Edition 11 Wing Commander’S Message
December 2016 - Edition 11 Wing Commander’s Message Now that the holiday season is upon us, we can concentrate on spending time with our friends and loved ones. It is a much deserved rest after an extremely busy and challenging year. I will be taking the time provided to enjoy a few moments with my family and friends and hope you find time to do the same. As I am sure you are aware, there have been many incredible achievements this year. We conducted yet another successful Exercise MAPLE FLAG, with great Canadian participation and a strong showing from our international partners, including France, the United States and the Royal Air Force. We also conducted a host of successful exercises both here at home and abroad. There’s been a great deal to be proud of this year. We were honoured to host Major-General Christian Drouin while he presented 4 Wing with the Royal Canadian Air Force Commander’s Unit Commendation for our excep- tional responsiveness to, and effectiveness in support of our 24/7 NORAD mission. Although a distinct honour, this isn’t the only award worth mentioning in 2016, as 417 Combat Support Squadron received the JTF-W Command Team Commendation for their outstanding contributions to the Canadian Armed Forces’ 2013 flood relief operations in Calgary, Alberta. There were also a variety of other individ- ual and unit awards handed out throughout the year to members of 4 Wing Cold Lake, both at the local and national levels. We also began what I hope is the first of many workshops for our leadership team here in Cold Lake.