Care and Social Services Inspectorate Wales
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Denbighshire Record Office
GB 0209 DD/BE Denbighshire Record Office This catalogue was digitised by The National Archives as part of the National Register of Archives digitisation project NRA 30556 The National Archives CLWYD RECORD OFFICE L ARO S.P.BEVON MSS. Schedule of documents deposited on indefinite loan by the County Librarian per Wrexham Area Library. 20 July 1976 (Ref: DD/BE) Clwyd Record Office 46, Clwyd Street, Ruthin, Clwyd A.N. 321 July 1987 S.P.BEVON MSS. This collection consists of material received from a Wrexham solicitor, relating to his personal and business affairs, and to some of his clients. The bulk of S.P.Bevon's personal papers consist of correspondence about properties he owned in Wrexham, and reports and prospectuses of various mining and plantation concerns abroad, in which he owned shares. There is no autobiographical material. The rest of the collection has been sorted into sequence by parish, with separate sections for court cases and election papers, as there is no large quantity of material relating to an individual client. Perhaps the most interesting item is a photograph showing the range of products made by Ewloe Potteries, Buckley, in the 1920s. Other interesting subjects include Ffos-y-go Colliery, Gwersyllt, 1901-4; the appointment of a receiver for the New Llangollen Slate and Slab Company. 1898-1903; prospectus of Broughton Hall Iron Company, c.1890; complaints about conditions at Croesnewydd Military Hospital, Wrexham, 1917; and a dispute over building costs of a new church at Brynteg, 1894-5. There are also some files of papers relating to S.P.Bevon's clients, 1920-40, in the Wrexham Library collection. -

Denbighshire Record Office
GB 0209 DD/W Denbighshire Record Office This catalogue was digitised by The National Archives as part of the National Register of Archives digitisation project NRA 30234 The National Archives CLWYD RECORD OFFICE WREXHAM SOLICITORS' MSS. (Schedule of documen^sdeposited indefinite loan bvM Bff and Wrexham. 26 November 1976, 28 September 1977, 15 February 1980). (Ref: DD/W) Clwyd Record Office, 46, Clwyd Street, A.N. 376, 471, 699 RUTHIN December 1986 WREXHAM SOLICITORS MSS. CONTENTS A.N. 471 GROVE PARK SCHOOL, WREXHAM: Governors 1-5 General 6-56 Miscellaneous 57 65 ALICE PARRY'S PAPERS 66 74 DENBIGHSHIRE EDUCATION AUTHORITY 75 80 WREXHAM EDUCATION COMMITTEE 81-84 WREXHAM AREA DIVISIONAL EXECUTIVE 85 94 WREXHAM BOROUGH COUNCIL: Treasurer 95 99 Medical Officer's records 100 101 Byelaws 102 Electricity 103 - 108 Rating and valuation 109 - 112 Borough extension 113 - 120 Miscellaneous 121 - 140 WREXHAM RURAL DISTRICT COUNCIL 140A DENBIGHSHIRE COUNTY COUNCIL 141 142 CALVINISTIC METHODIST RECORDS: SeioSeionn CM.Chapel,, RegenRegentt StreeStreett 143 - 153 CapeCapell yy M.CM.C.. Adwy'Adwy'rr ClawdClawddd 154 - 155 Henaduriaeth Dwyrain Dinbych 156 - 161 Henaduriaeth Dyffryn Clwyd 162 - 164 Henaduriaeth Dyffryn Conwy 165 Cyfarfod misol Sir Fflint 166 North Wales Association of the 167 - 171 Presbyterian Church Cymdeithasfa chwaterol 172 - 173 Miscellaneous 174 - 180 PRESBYTERIAN CHURCH OF WALES: Lancashire, Cheshire, Flintshire and 181 - 184 Denbighshire Presbyterian Church Lancashire and Cheshire Presbytery 185 - 186 Cheshire, Denbighshire -

Wrexham Social Care Workforce Development Partnership Communication Plan
Workforce Development Wrexham Social Care Workforce Development Partnership Communication Plan 2020/21 The Communication Plan for 2020/21 is as follows:- All stakeholders will be sent copies of all training events across all relevant qualifications. These events will be circulated by means of the training brochure (both electronically and hard copy). The brochure is on the Wrexham County Borough Council website & has details of all courses, how to apply and an application form. Dates will be sent out by flyer to all stakeholders. The current method of booking places on courses is electronically via e-mail or phone call. All Partnership meetings are open to all stakeholders and the agendas and minutes are circulated in advance electronically. All such courses are free to all stakeholders in Wrexham. The council reserves the right to charge for non-attendance. The list of all stakeholders is attached as Appendix 1. This includes: a) All registered care homes, domiciliary providers in Wrexham. b) All registered children’s homes, fostering and adoption agencies in Wrexham. c) Foster carers’ views are currently represented via the fostering agencies. d) Further and higher education is represented by Glyndŵr University, Academic Lead, Social and Community and Coleg Cambria, Assessor, Internal Verifier and Tutor of Health and Social Care Employer Engagement. The views of service users and carers are currently sought using a range of existing forums. In addition to these key stakeholders, membership also includes:- Voluntary independent organisations that employ either social care or Social Workers. Association of Voluntary Organisations in Wrexham. BCHUB. Jobcentre Plus. Early Years via. Wrexham Family Information Services. -

A Caring Place to Call Home
Stansty House A CARING PLACE TO CALL HOME care group Welcome to Stansty House... Welcome to Stansty House, a home that provides an excellent standard of care 24 hours a day. Whether you are looking for residential, nursing, dementia, day care, respite or end of life care, Stansty House has all the facilities and expertise to meet your needs. Our fully trained caring staff are committed to helping residents maintain good health, dignity and respect at all times. Stansty House aims to provide a happy, relaxed and friendly setting in which the well being, care and comfort of our residents is of prime importance. We encourage residents to continue to live as independently as possible while maintaining their chosen lifestyle in an environment, which provides the highest standard of quality care. You are very welcome to visit us so you can see the high standard of care we have to offer and experience what life is like here. To arrange a visit, or simply to have a chat with our Home Manager, please call 01978 290373 ext 5. “Stansty House, so much to look forward to...” Yo u r su r r o u n d i n gs ... Stansty House is a high quality care home where the majority of the accommodation was purpose built in 2005. Residents can pursue their hobbies in our communal and quiet lounges where they can watch television, listen to music or perhaps have some reading time. Outside the residential and nursing unit there is a garden with a lawn surrounded by plants, patio and seating area. -
A483 Wrexham Local Model Validation Report
A483 Wrexham Local Model Validation Report March 2020 NMWTRA Mott MacDonald 2 Callaghan Square Cardiff CF10 5BT United Kingdom T +44 (0)29 2046 7800 mottmac.com NMWTRA A483 Wrexham 402166 0017 A P:\Cardiff\ERA\ITD\Projects\402495 A483 Wrexham KS2\6.0 Local ModelReports\LMVR\402495_A483 Validation WrexhamLMVR_v1.7 Report accepting changes.docx Mott MacDonald March 2020 Mott MacDonald Limited. Registered in England and Wales no. 1243967. Registered office: Mott MacDonald House, 8-10 Sydenham Road, Croydon CR0 2EE, NMWTRA United Kingdom Mott MacDonald | A483 Wrexham Local Model Validation Report Issue and Revision Record Revision Date Originator Checker Approver Description A November W Davies/N Johnson/ S Arthur/C N/A DRAFT 2019 A Shaw Currie B January W Davies / A Shaw S Arthur C Currie FINAL 2020 C March 2020 W Davies / A Shaw S Arthur C Currie FINAL Document reference: 402166 | 0017_C Information class: Standard This document is issued for the party which commissioned it and for specific purposes connected with the above-captioned project only. It should not be relied upon by any other party or used for any other purpose. We accept no responsibility for the consequences of this document being relied upon by any other party, or being used for any other purpose, or containing any error or omission which is due to an error or omission in data supplied to us by other parties. This document contains confidential information and proprietary intellectual property. It should not be shown to other parties without consent from us and from the party which commissioned it. -

Item No Corporate Governance and Policy
ITEM NO CORPORATE GOVERNANCE AND POLICY SCRUTINY COMMITTEE WEDNESDAY 28 NOVEMBER 2007 REPORT OF CHIEF ECONOMIC DEVELOPMENT OFFICER ALCOHOL CONTROL ZONES 1. PURPOSE OF THE REPORT 1.1 To provide Members with information on the Local Government (Alcohol Consumption in Designated Public Places) Regulation 2001/2007, details of expressed support and consideration of options to recommend how this could be progressed in the County Borough 2. INFORMATION a) Background 2.1 According to the 2006/07 British Crime Survey (BCS), victims believed the offender or offenders to be under the influence of alcohol in 46% of all violent incidents in England and Wales. For ‘stranger violence’, this figure rises to 58%. Operational intelligence from the three Territorial Inspectors policing the county borough advises that alcohol and in particular under age drinking is a significant contributing factor to incidents of anti-social behaviour and disorder. 2.2 In tackling alcohol related crime and disorder, many Local Authorities in England and Wales have recognised the value in using the Local Government (Alcohol Consumption in Designated Public Places) Regulation 2001, revised in Regulation 2007. The use of the Regulation has three broad objectives, to: • reduce the problems arising from under-age drinking; • reduce public drunkenness; and • prevent alcohol related violence. 2.3 According to Home Office figures, up to May 2007, five hundred Designated Public Places Orders (DPPOs), sometimes known as Alcohol Control Zones, had been applied for in England and Wales. Two of these relate to areas within Wrexham including: Llwyn Isaf (since June 2002) and the Town Centre including Bellevue Park (since January 2005). -
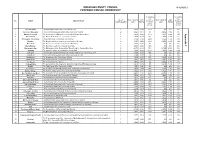
Appendix 2 of Draft Proposals
WREXHAM COUNTY COUNCIL APPENDIX 3 PROPOSED COUNCIL MEMBERSHIP % variance % variance from from No. OF ELECTORATE 2018 ELECTORATE 2023 No. NAME DESCRIPTION Proposed Proposed COUNCILLORS 2018 RATIO 2023 RATIO County County average average 1 Acrefair North The Plas Madoc ward of the Community of Cefn 1 1,639 1,639 -11% n/a n/a n/a 2 Acton and Maesydre The Acton and Maesydre wards of the Community of Acton 2 3,824 1,912 4% 3,932 1,966 3% Appendix 3 Appendix 3 Bangor Is-y-Coed The Communities of Bangor Is-y-Coed and Willington Worthenbury 1 1,628 1,628 -11% 1,628 1,628 -15% 4 Borras Park The Borras Park ward of the Community of Acton 1 1,964 1,964 7% 1,964 1,964 3% 5 Bronington and Hanmer The Communities of Bronington and Hanmer 1 1,466 1,466 -20% 1,466 1,466 -23% 6 Brymbo The Brymbo and Vron wards of the Community of Brymbo 2 3,107 1,554 -15% 3,274 1,637 -14% 7 Bryn Cefn The Bryn Cefn ward of the Community of Broughton 1 1,966 1,966 7% n/a n/a n/a 8 Brynyffynnon The Brynffynon ward of the Community of Offa 1 2,026 2,026 10% n/a n/a n/a 9 Burton and Llay The Burton ward of the Community of Rossett and the Community of Llay. 2 4,378 2,189 19% 5,125 2,563 34% 10 Cartrefle The Cartrefle ward of the Community of Caia Park 1 1,636 1,636 -11% 1,636 1,636 -14% 11 Cefn East The Cefn and, Rhosymedre and Cefn Bychan wards of the Community of Cefn 1 1,669 1,669 -9% n/a n/a n/a 12 Cefn West The Acrefair and Penybryn ward of the Community of Cefn 1 1,703 1,703 -7% n/a n/a n/a 13 Chirk North The North ward of the Community of Chirk 1 1,836 1,836 0% 1,836 1,836 -4% 14 Chirk South The South ward of the Community of Chirk 1 1,552 1,552 -15% 1,552 1,552 -19% 15 Coedpoeth The Community of Coedpoeth 2 3,532 1,766 -4% 3,532 1,766 -7% 16 Ceiriog Valley The Communities of Ceiriog Ucha, Glyntraian and Llansantffraid Glyn Ceiriog 1 1,679 1,679 -8% 1,679 1,679 -12% 17 Erddig The Erddig ward of the Community of Offa 1 1,801 1,801 -2% n/a n/a n/a 18 Esclusham The Bersham and Rhostyllen wards of the Community of Esclusham. -

Wrexham Town Centre and Grosvenor Road
Urbanwalks town centre 2.qxp 09/03/2006 16:18 Page 2 urbanwalks® six urbanwalksTM Grosvenor Road & Wrexham Town Centre Urbanwalks town centre 2.qxp 09/03/2006 16:18 Page 3 Welcome to Urbanwalks™ Urbanwalks is a vehicle to get communities moving again. The company has a simple philosophy to get people enjoying more activity more often in their everyday environment. Urbanwalks in partnership with the Welsh Assembly Government are promoting a nationwide walking initiative. This Urbanwalks leaflet helps to encourage people in Wrexham to get out there and walk. The leaflet’s unique format promotes a variety of circular routes of differing lengths that encompass typical everyday journeys within the local area. Urbanwalks is working with the Transport Directorate to help deliver the aims set out within the Walking and Cycling strategy document for Wales. Health benefits of walking Significant health benefits can be obtained by taking the right amount of physical activity. The current adult recommendation is at least 30 minutes of moderate intensity activity on five or more days of the week. Alarmingly, only about 37% of men and 25% of women currently achieve the recommended levels. Brisk walking is the perfect activity to help you meet the current recommendations. Benefits of regular physical activity Reduce high blood pressure – Moderate intensity activity, such as brisk walking, appears to be at least as effective in reducing blood pressure as more vigorous activity. Prevention of Diabetes – Exercise greatly reduces the risk of developing Type 2 Diabetes. Helps reduce weight – Physical activity in combination with a healthy diet can help to reduce weight and maintain weight loss. -

Wrexham Table: Welsh Language Skills KS207WA0009 (No Skills in Welsh)
Wrexham Table: Welsh language skills KS207WA0009 (No skills in Welsh) Rossett Llay Marford and Hoseley Gwersyllt North Bryn CefnGwersyllt East and SouthGresford East and West Brymbo Gwersyllt WestBorras Park Little Acton Gwenfro Acton Rhosnesni New Broughton Garden Village Minera StanstyCartrefle Holt Grosvenor Smithfield Maesydre Coedpoeth Wynnstay Brynyffynnon Offa Queensway Whitegate HermitageErddig PonciauEsclusham Pant Penycae Johnstown Marchwiel Penycae and Ruabon South Ruabon Cefn Plas Madoc Llangollen Rural Bronington Chirk North Overton Chirk South Dyffryn Ceiriog/Ceiriog Valley %, 2011 Census under 53 53 to 62 62 to 69 69 to 76 76 to 81 81 to 85 over 85 The maps show percentages within Census 2011 output areas, within electoral divisions Map created by Hywel Jones. Variables KS208WA0022−27 corrected Contains National Statistics data © Crown copyright and database right 2013; Contains Ordnance Survey data © Crown copyright and database right 2013 Wrexham Table: Welsh language skills KS207WA0010 (Can understand spoken Welsh only) Rossett Llay Marford and Hoseley Gwersyllt North Brymbo Gwersyllt East and SouthGresford East and West Little Acton Bryn Cefn Garden Village GwenfroStansty Acton Gwersyllt West Grosvenor Borras Park Minera New BroughtonMaesydre Rhosnesni Holt Wynnstay Coedpoeth CartrefleWhitegate Brynyffynnon Smithfield Queensway Offa Ponciau ErddigHermitage Esclusham Pant Johnstown Marchwiel Penycae Ruabon Penycae and Ruabon South Cefn Plas Madoc Llangollen Rural Bronington Chirk North Overton Chirk South Dyffryn Ceiriog/Ceiriog -

Applying for Housing Local Connection
HOUSING AND ECONOMY APPLYING FOR HOUSING Local Connection We will use the following criteria to assess whether you have a Local Connection. If you do not have a Local Connection, your application will be placed in Band 4, regardless of any housing need:- Borough Connection An applicant will be assessed as having a Borough Connection if they have: • � Lived continually in the Borough for at least 3 years in the last 5 years of their own choice. An applicant will not establish a connection with the Borough by residing in a prison or bail hostel. • � Family members living in the Borough. For the purpose of this policy, a family member will be a mother, father, sister, brother, children, grandparents or any adult who acted as the applicant’s parent and who has lived continually in the Borough for the last 5 years. • � Been in continual employment in the Borough area for at least 3 years in the last 5 years. This must be confirmed in a letter from your employer. • � Asylum seekers dispersed to Wrexham without any choice and granted refugee status will have a Borough connection at the point of application. • � Applicants living in refuge accommodation (e.g. women’s refuge) in Wrexham County, will have a Borough connection at the point of application. HOUSING AND ECONOMY APPLYING FOR HOUSING Community Connection An applicant will be assessed as having a Community Connection if:- • � They have lived continually in the Community for at least 3 years in the last 5 years of their own choice. • � They have family associations within the Community. -

Polling Places and Polling Districts Wrexham
Wrexham County Borough Council - Wrexham Constituency Polling Districts and Polling Places (2019) Polling District Electors Polling Station Scheme BBA - Isycoed 346 Isycoed Village Hall, Bowling Bank, Wrexham BBB - Holt 1,280 Holt Community Centre - Rear Room Access, Chapel Street, Holt BBD - Abenbury 958 Pentre Gwyn and Tanycoed Community Centre, Abenbury Road CAA - Allington 1,831 St Peter's Church In Wales Primary School, Chapel Lane, Rossett CAB - Burton 776 Rossett & Burton Village Hall, Station Road CBA - Marford/Hoseley 1,833 Gresford Methodist Church Hall, Chester Road, Gresford CCA - Gresford West 1,358 Gresford Memorial Hall, Off High Street, Gresford CCB - Gresford East 953 Gresford Memorial Hall, Off High Street, Gresford DAA - Bryn 1,183 Church of the Nazarene, Nant-Y-Gaer Road, Llay DAB - Park 2,369 St Martin's Church Hall, Market Square,Llay EAA001 - Gwersyllt - North 321 Cefn-Y-Bedd Community Centre, Sydallt Lane, Cefn-Y-Bedd EAA002 - Gwersyllt - North 684 Ysgol Heulfan Junior School Hall, Sunny View, Gwersyllt EAA003 - Gwersyllt - North 983 The Institute, New Road, Summerhill EBA001 - Gwersyllt - South 171 Bradley Village Hall, Glanllyn Road, Bradley EBA002 - Gwersyllt - South 1,254 Gwersyllt Congregational Church, 3 Dodds Lane EBA003 - Gwersyllt - South 455 Gresford Colliery Sports and Social Club, Bluebell Lane, Pandy EBB001 - Gwersyllt - East 888 Bradley Village Hall, Glanllyn Road, Bradley EBB002 - Gwersyllt - East 890 Gwersyllt Congregational Church, 3 Dodds Lane ECA - Gwersyllt - West 2,310 Gwersyllt Community Resource -

DENBIGH COUNTY COUNCIL. Local Government Act, 1888, 51 & 52 Vict
12 DENBIGHSHIRE. [SLATER'S DENBIGH COUNTY COUNCIL. Local Government Act, 1888, 51 & 52 Vict. c. 41. Under the above Act, Denbighshire, after the 1st standing joint committee of the Quarter Sessions and April 1889, for the purposes of the Act, became a the County Council, to be appointed as therein men separate and distinct administrative county (sec. 461b), tioned (sec. 9). governed by a County Council, consisting of chair- The coroners for the county are elected by the County man, aldermen & councillors (the number of coun- Council, and the clerk of the peace appointed by such .cillors being determined by the Local Government joint committee, and may be removed by them Board), to be elected in manner prescribed by the (sec. 83-2). Act (sec. 2). · The clerk of the peace for the county is also the clerk ~The chairman shall, by virtue of his office, be a of the County Council (sec. 83-1). justice of the peace for the county, without qualifica- The administrative business of the county (which tion (sec. 46). would, if this Act had not been passed, have been trans- The police for the country are under the control of a acted by the justices) is transacted by the County Council. Meet at Denbigh. CHAIRMAN-Samuel Moss, Broad Oak, Rossett. VICE-CHAIRMAN-Sir Herbert Lloyd Watkin Williams-Wynn hart. Wynnstay, Rnabon. ALDERMEN. Retire in March 1898. Henry Dennis, New hall, Ruabon William Lester, Bran Offa, Wrexham William Douglas Wynne Griffith, Garn Trcfnant R.S.O John Watkin Lumley, Brynhyfryd, Ruthin John Jones, St. John's, Wrexham T.