Identifying at Risk Populations and Hiv/Aids Referral Services
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Districts of Ethiopia
Region District or Woredas Zone Remarks Afar Region Argobba Special Woreda -- Independent district/woredas Afar Region Afambo Zone 1 (Awsi Rasu) Afar Region Asayita Zone 1 (Awsi Rasu) Afar Region Chifra Zone 1 (Awsi Rasu) Afar Region Dubti Zone 1 (Awsi Rasu) Afar Region Elidar Zone 1 (Awsi Rasu) Afar Region Kori Zone 1 (Awsi Rasu) Afar Region Mille Zone 1 (Awsi Rasu) Afar Region Abala Zone 2 (Kilbet Rasu) Afar Region Afdera Zone 2 (Kilbet Rasu) Afar Region Berhale Zone 2 (Kilbet Rasu) Afar Region Dallol Zone 2 (Kilbet Rasu) Afar Region Erebti Zone 2 (Kilbet Rasu) Afar Region Koneba Zone 2 (Kilbet Rasu) Afar Region Megale Zone 2 (Kilbet Rasu) Afar Region Amibara Zone 3 (Gabi Rasu) Afar Region Awash Fentale Zone 3 (Gabi Rasu) Afar Region Bure Mudaytu Zone 3 (Gabi Rasu) Afar Region Dulecha Zone 3 (Gabi Rasu) Afar Region Gewane Zone 3 (Gabi Rasu) Afar Region Aura Zone 4 (Fantena Rasu) Afar Region Ewa Zone 4 (Fantena Rasu) Afar Region Gulina Zone 4 (Fantena Rasu) Afar Region Teru Zone 4 (Fantena Rasu) Afar Region Yalo Zone 4 (Fantena Rasu) Afar Region Dalifage (formerly known as Artuma) Zone 5 (Hari Rasu) Afar Region Dewe Zone 5 (Hari Rasu) Afar Region Hadele Ele (formerly known as Fursi) Zone 5 (Hari Rasu) Afar Region Simurobi Gele'alo Zone 5 (Hari Rasu) Afar Region Telalak Zone 5 (Hari Rasu) Amhara Region Achefer -- Defunct district/woredas Amhara Region Angolalla Terana Asagirt -- Defunct district/woredas Amhara Region Artuma Fursina Jile -- Defunct district/woredas Amhara Region Banja -- Defunct district/woredas Amhara Region Belessa -- -
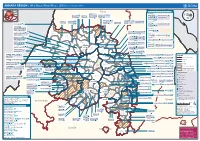
AMHARA REGION : Who Does What Where (3W) (As of 13 February 2013)
AMHARA REGION : Who Does What Where (3W) (as of 13 February 2013) Tigray Tigray Interventions/Projects at Woreda Level Afar Amhara ERCS: Lay Gayint: Beneshangul Gumu / Dire Dawa Plan Int.: Addis Ababa Hareri Save the fk Save the Save the df d/k/ CARE:f k Save the Children:f Gambela Save the Oromia Children: Children:f Children: Somali FHI: Welthungerhilfe: SNNPR j j Children:l lf/k / Oxfam GB:af ACF: ACF: Save the Save the af/k af/k Save the df Save the Save the Tach Gayint: Children:f Children: Children:fj Children:l Children: l FHI:l/k MSF Holand:f/ ! kj CARE: k Save the Children:f ! FHI:lf/k Oxfam GB: a Tselemt Save the Childrenf: j Addi Dessie Zuria: WVE: Arekay dlfk Tsegede ! Beyeda Concern:î l/ Mirab ! Concern:/ Welthungerhilfe:k Save the Children: Armacho f/k Debark Save the Children:fj Kelela: Welthungerhilfe: ! / Tach Abergele CRS: ak Save the Children:fj ! Armacho ! FHI: Save the l/k Save thef Dabat Janamora Legambo: Children:dfkj Children: ! Plan Int.:d/ j WVE: Concern: GOAL: Save the Children: dlfk Sahla k/ a / f ! ! Save the ! Lay Metema North Ziquala Children:fkj Armacho Wegera ACF: Save the Children: Tenta: ! k f Gonder ! Wag WVE: Plan Int.: / Concern: Save the dlfk Himra d k/ a WVE: ! Children: f Sekota GOAL: dlf Save the Children: Concern: Save the / ! Save: f/k Chilga ! a/ j East Children:f West ! Belesa FHI:l Save the Children:/ /k ! Gonder Belesa Dehana ! CRS: Welthungerhilfe:/ Dembia Zuria ! î Save thedf Gaz GOAL: Children: Quara ! / j CARE: WVE: Gibla ! l ! Save the Children: Welthungerhilfe: k d k/ Takusa dlfj k -

Using Geospatial Techniques in the Selection of Potential Ecotourism Sites in Menz-Geramidir District, Ethiopia
Using Geospatial Techniques in the Selection of Potential Ecotourism Sites in Menz-geramidir District, Ethiopia Baykedagn Taye 1 Sintayehu Legesse Gebre2,3* Dessalegn Obsi Gemeda2 Kefelegn Getahun1 Abstract Ecotourism is expressed as when tourists are attracted to a given geographic area (i.e. space) which has its own available natural, environmental, and socioeconomic resources by considering environmental sustainability, local benefit, and promotion. Space is an elementary part of ecotourism activities. Hence, the aim of this study is to identify potential ecotourism sites in Menz-geramidir district mainly by considering the natural features. Using weighting of each factor, three criteria and five-factor maps are identified, namely: landscape (land use land cover map), topography (elevation and slope map) and accessibility (road and river map). Those identified factor maps first ranked based on expert opinion, and then the weight of influence ofeach factor was computed by pair-wise comparison technique which is one of AHP method. The image classification was carried out in ERDAS imagine software using supervised image classification method. The image classification accuracy assessment indicates that the overall accuracy is 84% and the overall Kappa coefficient is 0.80. The final ecotourism potential sites model map was created based on the linear combination of factors with their respective weights in ArcGIS overlay extension and presented using FAO`s suitability scheme into four classes. The result showed that11% is highly suitable and lies to the eastern part of the study area. Generally,major suitable and moderately suitable area accounts for 75.6 % and marginally suitable area for 13.5 % and the not suitable area is 0.06 %. -

Census Data/Projections, 1999 & 2000
Census data/Projections, 1999 & 2000 Jan - June and July - December Relief Bens., Supplementary Feeding Bens. TIGRAY Zone 1994 census 1999 beneficiaries - May '99 2000 beneficiaries - Jan 2000 July - Dec 2000 Bens Zone ID/prior Wereda Total Pop. 1999 Pop. 1999 Bens. 1999 bens % 2000 Pop. 2000 Bens 2000 bens Bens. Sup. July - Dec Bens July - Dec Bens ity Estimate of Pop. Estimate % of Pop. Feeding % of pop 1 ASEGEDE TSIMBELA 96,115 111,424 114,766 1 KAFTA HUMERA 48,690 56,445 58,138 1 LAELAY ADIYABO 79,832 92,547 5,590 6% 95,324 7,800 8% 11,300 12% Western 1 MEDEBAY ZANA 97,237 112,724 116,106 2,100 2% 4,180 4% 1 TAHTAY ADIYABO 80,934 93,825 6,420 7% 96,639 18,300 19% 24,047 25% 1 TAHTAY KORARO 83,492 96,790 99,694 2,800 3% 2,800 3% 1 TSEGEDE 59,846 69,378 71,459 1 TSILEMTI 97,630 113,180 37,990 34% 116,575 43,000 37% 15,050 46,074 40% 1 WELKAIT 90,186 104,550 107,687 Sub Total 733,962 850,863 50,000 6% 876,389 74,000 8% 15,050 88,401 10% *2 ABERGELE 58,373 67,670 11,480 17% 69,700 52,200 75% 18,270 67,430 97% *2 ADWA 109,203 126,596 9,940 8% 130,394 39,600 30% 13,860 58,600 45% 2 DEGUA TEMBEN 89,037 103,218 7,360 7% 106,315 34,000 32% 11,900 44,000 41% Central 2 ENTICHO 131,168 152,060 22,850 15% 156,621 82,300 53% 28,805 92,300 59% 2 KOLA TEMBEN 113,712 131,823 12,040 9% 135,778 62,700 46% 21,945 67,700 50% 2 LAELAY MAYCHEW 90,123 104,477 3,840 4% 107,612 19,600 18% 6,860 22,941 21% 2 MEREB LEHE 78,094 90,532 14,900 16% 93,248 57,500 62% 20,125 75,158 81% *2 NAEDER ADET 84,942 98,471 15,000 15% 101,425 40,800 40% 14,280 62,803 62% 2 -

English-Full (0.5
Enhancing the Role of Forestry in Building Climate Resilient Green Economy in Ethiopia Strategy for scaling up effective forest management practices in Amhara National Regional State with particular emphasis on smallholder plantations Wubalem Tadesse Alemu Gezahegne Teshome Tesema Bitew Shibabaw Berihun Tefera Habtemariam Kassa Center for International Forestry Research Ethiopia Office Addis Ababa October 2015 Copyright © Center for International Forestry Research, 2015 Cover photo by authors FOREWORD This regional strategy document for scaling up effective forest management practices in Amhara National Regional State, with particular emphasis on smallholder plantations, was produced as one of the outputs of a project entitled “Enhancing the Role of Forestry in Ethiopia’s Climate Resilient Green Economy”, and implemented between September 2013 and August 2015. CIFOR and our ministry actively collaborated in the planning and implementation of the project, which involved over 25 senior experts drawn from Federal ministries, regional bureaus, Federal and regional research institutes, and from Wondo Genet College of Forestry and Natural Resources and other universities. The senior experts were organised into five teams, which set out to identify effective forest management practices, and enabling conditions for scaling them up, with the aim of significantly enhancing the role of forests in building a climate resilient green economy in Ethiopia. The five forest management practices studied were: the establishment and management of area exclosures; the management of plantation forests; Participatory Forest Management (PFM); agroforestry (AF); and the management of dry forests and woodlands. Each team focused on only one of the five forest management practices, and concentrated its study in one regional state. -

Ethiopia: Amhara Region Administrative Map (As of 05 Jan 2015)
Ethiopia: Amhara region administrative map (as of 05 Jan 2015) ! ! ! ! ! ! ! ! ! ! Abrha jara ! Tselemt !Adi Arikay Town ! Addi Arekay ! Zarima Town !Kerakr ! ! T!IGRAY Tsegede ! ! Mirab Armacho Beyeda ! Debark ! Debarq Town ! Dil Yibza Town ! ! Weken Town Abergele Tach Armacho ! Sanja Town Mekane Berhan Town ! Dabat DabatTown ! Metema Town ! Janamora ! Masero Denb Town ! Sahla ! Kokit Town Gedebge Town SUDAN ! ! Wegera ! Genda Wuha Town Ziquala ! Amba Giorges Town Tsitsika Town ! ! ! ! Metema Lay ArmachoTikil Dingay Town ! Wag Himra North Gonder ! Sekota Sekota ! Shinfa Tomn Negade Bahr ! ! Gondar Chilga Aukel Ketema ! ! Ayimba Town East Belesa Seraba ! Hamusit ! ! West Belesa ! ! ARIBAYA TOWN Gonder Zuria ! Koladiba Town AMED WERK TOWN ! Dehana ! Dagoma ! Dembia Maksegnit ! Gwehala ! ! Chuahit Town ! ! ! Salya Town Gaz Gibla ! Infranz Gorgora Town ! ! Quara Gelegu Town Takusa Dalga Town ! ! Ebenat Kobo Town Adis Zemen Town Bugna ! ! ! Ambo Meda TownEbinat ! ! Yafiga Town Kobo ! Gidan Libo Kemkem ! Esey Debr Lake Tana Lalibela Town Gomenge ! Lasta ! Muja Town Robit ! ! ! Dengel Ber Gobye Town Shahura ! ! ! Wereta Town Kulmesk Town Alfa ! Amedber Town ! ! KUNIZILA TOWN ! Debre Tabor North Wollo ! Hara Town Fogera Lay Gayint Weldiya ! Farta ! Gasay! Town Meket ! Hamusit Ketrma ! ! Filahit Town Guba Lafto ! AFAR South Gonder Sal!i Town Nefas mewicha Town ! ! Fendiqa Town Zege Town Anibesema Jawi ! ! ! MersaTown Semen Achefer ! Arib Gebeya YISMALA TOWN ! Este Town Arb Gegeya Town Kon Town ! ! ! ! Wegel tena Town Habru ! Fendka Town Dera -

AMHARA Demography and Health
1 AMHARA Demography and Health Aynalem Adugna January 1, 2021 www.EthioDemographyAndHealth.Org 2 Amhara Suggested citation: Amhara: Demography and Health Aynalem Adugna January 1, 20201 www.EthioDemographyAndHealth.Org Landforms, Climate and Economy Located in northwestern Ethiopia the Amhara Region between 9°20' and 14°20' North latitude and 36° 20' and 40° 20' East longitude the Amhara Region has an estimated land area of about 170000 square kilometers . The region borders Tigray in the North, Afar in the East, Oromiya in the South, Benishangul-Gumiz in the Southwest and the country of Sudan to the west [1]. Amhara is divided into 11 zones, and 140 Weredas (see map at the bottom of this page). There are about 3429 kebeles (the smallest administrative units) [1]. "Decision-making power has recently been decentralized to Weredas and thus the Weredas are responsible for all development activities in their areas." The 11 administrative zones are: North Gonder, South Gonder, West Gojjam, East Gojjam, Awie, Wag Hemra, North Wollo, South Wollo, Oromia, North Shewa and Bahir Dar City special zone. [1] The historic Amhara Region contains much of the highland plateaus above 1500 meters with rugged formations, gorges and valleys, and millions of settlements for Amhara villages surrounded by subsistence farms and grazing fields. In this Region are located, the world- renowned Nile River and its source, Lake Tana, as well as historic sites including Gonder, and Lalibela. "Interspersed on the landscape are higher mountain ranges and cratered cones, the highest of which, at 4,620 meters, is Ras Dashen Terara northeast of Gonder. -

Periodic Monitoring Report Working 2016 Humanitarian Requirements Document – Ethiopia Group
DRMTechnical Periodic Monitoring Report Working 2016 Humanitarian Requirements Document – Ethiopia Group Covering 1 Jan to 31 Dec 2016 Prepared by Clusters and NDRMC Introduction The El Niño global climactic event significantly affected the 2015 meher/summer rains on the heels of failed belg/ spring rains in 2015, driving food insecurity, malnutrition and serious water shortages in many parts of the country. The Government and humanitarian partners issued a joint 2016 Humanitarian Requirements Document (HRD) in December 2015 requesting US$1.4 billion to assist 10.2 million people with food, health and nutrition, water, agriculture, shelter and non-food items, protection and emergency education responses. Following the delay and erratic performance of the belg/spring rains in 2016, a Prioritization Statement was issued in May 2016 with updated humanitarian requirements in nutrition (MAM), agriculture, shelter and non-food items and education.The Mid-Year Review of the HRD identified 9.7 million beneficiaries and updated the funding requirements to $1.2 billion. The 2016 HRD is 69 per cent funded, with contributions of $1.08 billion from international donors and the Government of Ethiopia (including carry-over resources from 2015). Under the leadership of the Government of Ethiopia delivery of life-saving and life- sustaining humanitarian assistance continues across the sectors. However, effective humanitarian response was challenged by shortage of resources, limited logistical capacities and associated delays, and weak real-time information management. This Periodic Monitoring Report (PMR) provides a summary of the cluster financial inputs against outputs and achievements against cluster objectives using secured funding since the launch of the 2016 HRD. -

North Shewa Delegation November, 2019
North Shewa Development Program Proposal ` North Shewa Delegation November, 2019 1 North Shewa Development Program Proposal Contents Contents ____________________________________________________________________ 2 • Introduction ______________________________________________________________ 3 • Itinerary _________________________________________________________________ 5 • Tour of Addis _____________________________________________________________ 8 • Preparations and recommendations __________________________________________ 9 • Overview of Zone ________________________________________________________ 11 • The Gedams _____________________________________________________________ 12 • Organizations and Stakeholders ____________________________________________ 16 • Fields of development _____________________________________________________ 20 • Part I: Community Development Program _____________________________________ 21 • Part II: Agricultural Development program ____________________________________ 22 • Part III: Artisan Craft Development Program __________________________________ 24 Contact info: Tomer Malchi IL number +972528021140 / Ethio number 0985487853 Yair Keinan IL number +972545805972 / Ethio number 0944058130 Belayneh Tazebku Ethio number 0913770375 Michael Demsse Ethio number 0911640486 2 North Shewa Development Program Proposal Introduction The Zone of North Shewa in the Amhara region of Ethiopia has been proposed for establishing a community-based development program focusing on agricultural and artisan craft. The communities -

Guidelines and Proposal for Food Security Assessment in North and South Gonder Zones
EMERGENCIES UNIT FOR UNITED NATIONS ETHIOPIA (UN-EUE) Cheffa Valley: refuge for 50,000 pastoralists and 200,000 animals Present humanitarian situation and livestock conditions in selected areas in and around Afar region Assessment Mission: 21- 26 July 2002 By Francois Piguet, UN-Emergencies Unit for Ethiopia 1 Introduction and background The mission’s major objective was to assess the humanitarian situation and livestock condition in selected surrounding areas of Afar region and in the Cheffa valley (Oromiya zone, Amhara region). The mission also cross-checked the situation in Afar region zone 5 and the Argobba special woreda (Afar region zone 3), from where unusual pastoralists movements started in January 2002. The assessment focused on animal condition, migration, marketing conditions and terms of trade, food availability and the nutritional situation in pastoralist settlements, particularly availability of milk. The mission hoped to get a better understanding of pastoralist stress migration and coping mechanisms in the western border zones with the Amhara highlands. During the field trip the following areas were visited: Adadlehangeg Sinkinamelket kebele in Simurobi Gele’Alo woreda (zone 5, Afar region), Cheffa Valley with temporary Afar settlements (Photo by Yves Guinand, UN- EUE, June 1999) Bati woreda (Oromiya zone, Amhara region), Telalak and Dewe woredas (zone 5, Afar region), Dalifage in Artuma woreda (zone 5, Afar region) Kemise (Oromiya zone, Amhara region), Showa Robit (North Showa, Amhara region) and Gacheni in Argobba special woreda (zone 3, Afar Region). Except Fursi woreda still located off-road, the four other woredas of zone 5, Afar region were visited. South-western areas in Afar Region: zone 5 as well as Dulecha close to Argobba woreda in zone 3, Afar pastoralists are usually moving to the western escarpment (Oromiya zone in Amhara Region and North Showa) and/or to Zone 3, along the Awash River. -

Ethnobotanical Study of Medicinal Plants Used to Treat Livestock Ailments in Ensaro District, North Shewa Zone, Amhara Region, Ethiopia
Ethnobotanical Study of Medicinal Plants Used To Treat Livestock Ailments In Ensaro District, North Shewa Zone, Amhara Region, Ethiopia Asaye Asfaw ( [email protected] ) Debre Brehan University Ermias Lulekal Addis Ababa University Tamrat Bekele Addis Ababa University Asfaw Debella Ethiopian Public Health Institute Eyob Debebe Ethiopian Public Health Institute Bihonegn Ssisay Ethiopian Public Health Institute Research Article Keywords: Ethiopia, Ethnoveterinary medicine, livestock diseases, indigenous knowledge Posted Date: August 17th, 2021 DOI: https://doi.org/10.21203/rs.3.rs-733200/v1 License: This work is licensed under a Creative Commons Attribution 4.0 International License. Read Full License Page 1/24 Abstract Introduction: In Ethiopia, the majority of animal owners throughout the country depend on traditional healthcare practices to manage their animals’ health. Ethnoveterinary practices play signicantly greater roles in livestock health care as an alternative or integral part of modern veterinary practices. This is because traditional medicines have remained the most economically affordable and easily available form of therapies for resource-poor communities. Even although, ethnoveterinary medicine is the most important and has higher acceptance and trust by the community in Ethiopia, ethnoveterinary medicinal plants and associated indigenous practices are not adequately documented. This study aimed to identify and document ethnoveterinary medicinal plants with their associated indigenous practices along with the habitats of these plants in Ensaro district. Methods: This ethnobotanical survey included 389 informants (283 males and 106 females) from all 14 kebeles of Ensaro district, which is the smallest administrative unit in Amhara Regional State's North Shewa Zone. Systematic random and intentional sampling techniques have been used to obtain representative informants. -

Coleoptera: Carabidae: Harpalinae) from Ethiopia Author(S): Francisco Novoa, Israel Gañán, and Andrés Baselga Source: the Coleopterists Bulletin, 69(4):713-722
Descriptions of Two New Species of Calathus Bonelli (Coleoptera: Carabidae: Harpalinae) from Ethiopia Author(s): Francisco Novoa, Israel Gañán, and Andrés Baselga Source: The Coleopterists Bulletin, 69(4):713-722. Published By: The Coleopterists Society DOI: http://dx.doi.org/10.1649/0010-065X-69.4.713 URL: http://www.bioone.org/doi/full/10.1649/0010-065X-69.4.713 BioOne (www.bioone.org) is a nonprofit, online aggregation of core research in the biological, ecological, and environmental sciences. BioOne provides a sustainable online platform for over 170 journals and books published by nonprofit societies, associations, museums, institutions, and presses. Your use of this PDF, the BioOne Web site, and all posted and associated content indicates your acceptance of BioOne’s Terms of Use, available at www.bioone.org/page/ terms_of_use. Usage of BioOne content is strictly limited to personal, educational, and non-commercial use. Commercial inquiries or rights and permissions requests should be directed to the individual publisher as copyright holder. BioOne sees sustainable scholarly publishing as an inherently collaborative enterprise connecting authors, nonprofit publishers, academic institutions, research libraries, and research funders in the common goal of maximizing access to critical research. The Coleopterists Bulletin, 69(4): 713–722. 2015. DESCRIPTIONS OF TWO NEW SPECIES OF CALATHUS BONELLI (COLEOPTERA: CARABIDAE:HARPALINAE) FROM ETHIOPIA FRANCISCO NOVOA,ISRAEL GAÑÁN, AND ANDRÉS BASELGA Departamento de Zoología y Antropología Facultad de Biología, Universidad de Santiago de Compostela E-15782 Santiago de Compostela, A Coruña, SPAIN [email protected] ABSTRACT Two new species of Calathus Bonelli are described from the Ethiopian Highlands, Ethiopa: Calathus kebedei Novoa, Gañán and Baselga [type locality = Ethiopia, Gojjam, Debre Markos at Danghle, near Robu Gebeya, Mt.