COVID-19 Immunization Screening and Consent Form* Recipient Name (Please Print) Preferred Name
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

What Do We Know About India's Covaxin Vaccine?
FEATURE Tamil Nadu, India COVID-19 VACCINES [email protected] BMJ: first published as 10.1136/bmj.n997 on 20 April 2021. Downloaded from Cite this as: BMJ 2021;373:n997 http://dx.doi.org/10.1136/bmj.n997 What do we know about India’s Covaxin vaccine? Published: 20 April 2021 India has rapidly approved and rolled out Covaxin, its own covid-19 vaccine. Kamala Thiagarajan examines what we know so far. Kamala Thiagarajan freelance journalist Who developed Covaxin? cheapest purchased by any country in the world at 206 rupees per shot for the 5.5 million doses the Covaxin was developed by Indian pharmaceutical government currently has on order. The government company Bharat Biotech in collaboration with the has capped the price of the vaccine sold in the private Indian Council of Medical Research, a government market, with private hospitals able to charge up to funded biomedical research institute, and its 250 rupees.13 subsidiary the National Institute of Virology. Covaxin does not require storage at sub-zero Bharat Biotech has brought to market 16 original temperatures, which would be hard to maintain in vaccines, including for rotavirus, hepatitis B, Zika India’s climate and with the frequent power cuts in virus, and chikungunya.1 The company reportedly rural areas. Covaxin is available in multi-dose vials spent $60-$70m (£43-£50m; €50-€58m) developing and is stable at the 2-8°C that ordinary refrigeration Covaxin.2 can achieve. How does Covaxin work? Bharat Biotech says it has a stockpile of 20 million The vaccine is similar to CoronaVac (the Chinese doses of Covaxin for India and is in the process of vaccine developed by Sinovac)3 in that it uses a manufacturing 700 million doses at its four facilities complete infective SARS-CoV-2 viral particle in two cities by the end of the year. -

COVID-19 Vaccination Programme: Information for Healthcare Practitioners
COVID-19 vaccination programme Information for healthcare practitioners Republished 6 August 2021 Version 3.10 1 COVID-19 vaccination programme: Information for healthcare practitioners Document information This document was originally published provisionally, ahead of authorisation of any COVID-19 vaccine in the UK, to provide information to those involved in the COVID-19 national vaccination programme before it began in December 2020. Following authorisation for temporary supply by the UK Department of Health and Social Care and the Medicines and Healthcare products Regulatory Agency being given to the COVID-19 Vaccine Pfizer BioNTech on 2 December 2020, the COVID-19 Vaccine AstraZeneca on 30 December 2020 and the COVID-19 Vaccine Moderna on 8 January 2021, this document has been updated to provide specific information about the storage and preparation of these vaccines. Information about any other COVID-19 vaccines which are given regulatory approval will be added when this occurs. The information in this document was correct at time of publication. As COVID-19 is an evolving disease, much is still being learned about both the disease and the vaccines which have been developed to prevent it. For this reason, some information may change. Updates will be made to this document as new information becomes available. Please use the online version to ensure you are accessing the latest version. 2 COVID-19 vaccination programme: Information for healthcare practitioners Document revision information Version Details Date number 1.0 Document created 27 November 2020 2.0 Vaccine specific information about the COVID-19 mRNA 4 Vaccine BNT162b2 (Pfizer BioNTech) added December 2020 2.1 1. -

1 Title: Interim Report of a Phase 2 Randomized Trial of a Plant
medRxiv preprint doi: https://doi.org/10.1101/2021.05.14.21257248; this version posted May 17, 2021. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. All rights reserved. No reuse allowed without permission. 1 Title: Interim Report of a Phase 2 Randomized Trial of a Plant-Produced Virus-Like Particle 2 Vaccine for Covid-19 in Healthy Adults Aged 18-64 and Older Adults Aged 65 and Older 3 Authors: Philipe Gobeil1, Stéphane Pillet1, Annie Séguin1, Iohann Boulay1, Asif Mahmood1, 4 Donald C Vinh 2, Nathalie Charland1, Philippe Boutet3, François Roman3, Robbert Van Der 5 Most4, Maria de los Angeles Ceregido Perez3, Brian J Ward1,2†, Nathalie Landry1† 6 Affiliations: 1 Medicago Inc., 1020 route de l’Église office 600, Québec, QC, Canada, G1V 7 3V9; 2 Research Institute of the McGill University Health Centre, 1001 Decarie St, Montreal, 8 QC H4A 3J1; 3 GlaxoSmithKline Biologicals SA (Vaccines), Avenue Fleming 20, 1300 Wavre, 9 Belgium; 4 GlaxoSmithKline Biologicals SA (Vaccines), rue de l’Institut 89, 1330 Rixensart, 10 Belgium; † These individuals are equally credited as senior authors. 11 * Corresponding author: Nathalie Landry, 1020 Route de l’Église, Bureau 600, Québec, Qc, 12 Canada, G1V 3V9; Tel. 418 658 9393; Fax. 418 658 6699; [email protected] 13 Abstract 14 The rapid spread of SARS-CoV-2 globally continues to impact humanity on a global scale with 15 rising morbidity and mortality. Despite the development of multiple effective vaccines, new 16 vaccines continue to be required to supply ongoing demand. -
Immunogenicity and Safety of a Third Dose, and Immune Persistence Of
medRxiv preprint doi: https://doi.org/10.1101/2021.07.23.21261026; this version posted July 25, 2021. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. All rights reserved. No reuse allowed without permission. 1 Immunogenicity and safety of a third dose, and immune persistence of 2 CoronaVac vaccine in healthy adults aged 18-59 years: interim results 3 from a double-blind, randomized, placebo-controlled phase 2 clinical 4 trial 5 6 Hongxing Pan MSc1*, Qianhui Wu MPH2*, Gang Zeng Ph.D.3*, Juan Yang Ph.D.1, Deyu 7 Jiang MSc4, Xiaowei Deng MSc2, Kai Chu MSc1, Wen Zheng BSc2, Fengcai Zhu M.D.5†, 8 Hongjie Yu M.D. Ph.D.2,6,7†, Weidong Yin MBA8† 9 10 Affiliations 11 1. Vaccine Evaluation Institute, Jiangsu Provincial Center for Disease Control and 12 Prevention, Nanjing, China 13 2. School of Public Health, Fudan University, Key Laboratory of Public Health Safety, 14 Ministry of Education, Shanghai, China 15 3. Clinical Research Department, Sinovac Biotech Co., Ltd., Beijing, China 16 4. Covid-19 Vaccine Department, Sinovac Life Sciences Co., Ltd., Beijing, China 17 5. Jiangsu Provincial Center for Disease Control and Prevention, Nanjing, China 18 6. Shanghai Institute of Infectious Disease and Biosecurity, Fudan University, 19 Shanghai, China 20 7. Department of Infectious Diseases, Huashan Hospital, Fudan University, 21 Shanghai, China 22 8. Sinovac Biotech Co., Ltd., Beijing, China NOTE: This preprint reports new research that has not been certified by peer review and should not be used to guide clinical practice. -

Periodic Update on AEFI
CONSOLIDATED REGIONAL AND GLOBAL INFORMATION ON ADVERSE EVENTS FOLLOWING IMMUNIZATION (AEFI) AGAINST COVID-19 AND OTHER UPDATES Thirteenth report WASHINGTON, DC Updated: 10 May 2021 1 OFFICIAL REPORTS ON PHARMACOVIGILANCE PROGRAMS CANADA • As of 30 April 2021, 13,420,198 doses of the COVID-19 vaccines of Pfizer-BioNTech, Moderna, Oxford- AstraZeneca, and the vaccine Covishield (AstraZeneca manufactured by the Serum Institute of India), had been administered. • A total of 4,548 individual reports of one or more adverse events (0.034% of doses administered) were received. Of these, 748 were considered serious events (0.006% of doses administered), with anaphylaxis being the one most frequently reported. • Of total reports, there were 2,072 non-serious and 520 serious events associated with the Pfizer-BioNTech vaccine. For the Moderna vaccine, 1,457 non-serious and 103 serious events were reported; for Covishield, there were 201 non-serious and 48 serious events, and for Oxford-AstraZeneca, 65 non-serious events and 62 serious events. • A total of 13,596 adverse events following immunization (AEFI) were reported, with 4,548 reports with one or more events. The most frequently reported non-serious adverse events were injection-site reactions, paresthesia, itching, hives, headache, hypoesthesia, and nausea. There were 61 reports of anaphylaxis. • Although 55% of vaccine doses were administered to women as of 30 April, and 45% to men, most of the reported adverse events were in women (84.3% of total doses). At the same time, 43.0% of total events were reported for people between the ages of 18 and 49, who account for 24% of people vaccinated. -

Comparative Characteristics of the Main Coronavirus Vaccines
Acta Scientific MICROBIOLOGY (ISSN: 2581-3226) Volume 4 Issue 9 September 2021 Editorial Comparative Characteristics of the Main Coronavirus Vaccines Pavel F Zabrodskii* Received: June 23, 2021 Saratov Medical University "REAVIZ", Saratov, Russian Federation Published: August 01, 2021 *Corresponding Author: Pavel F Zabrodskii, Saratov Medical University "REAVIZ", © All rights are reserved by Pavel F Saratov, Russian Federation. Zabrodskii. Since the beginning of the epidemic, vaccine development has been a priority for all developed countries. According to WHO (26 adenovirus rather than human adenovirus should reduce the risk virus. The fact that the vaccine was developed using chimpanzee January 2021), more than 60 vaccines worldwide are already in of allergic reactions and severe side-effects. However, the disadvan- clinical trials. More than 170 are being tested on animals. There tage of this product, as with all vector vaccines, is that the technol- ogy itself is new and has not previously been used in health care. One of the pluses for vector drug manufacturers is their speed of are 22 vaccines that have made it through the final phase of testing. creation. The vaccine is registered for use in the European Union. It The vaccine, developed by US company “Pfizer” and its German is licensed for emergency use in another 20 countries. clinical trials ended on 9 November 2020. In addition to EU coun- partner “BioNTech”, has been registered first in the EU. Phase III - ceutical company Sinovac Biotech, which has shown controversial tries, the vaccine is used in Australia, Saudi Arabia, Switzerland, “CoronaVac” is an inactivated vaccine from Chinese biopharma - Norway, Iceland, Serbia and some other countries. -

Iran Hopes to Defeat COVID with Home-Grown Crop of Vaccines
Q&A Iran hopes to defeat COVID with home-grown crop of vaccines Iran is one of few Middle Eastern nations to transfer money is restricted, it is difficult with the capacity to develop vaccines. It to buy drugs and medicines. And we have has been doing so in earnest: more than the technology to produce vaccines, so why ten are in development, but little is known not use it? To ensure the safety of Iranians, it about them outside Iran. Nature speaks makes sense to develop a variety of vaccines to Kayhan Azadmanesh, head of the using different research and development virology division at the Pasteur Institute of strategies, as China has done. Iran in Tehran, about the nation’s vaccine landscape. Azadmanesh also advises the Why are Iranian researchers reluctant to Iranian government and is developing publicize their work internationally? vaccines through his spin-off company This could be another effect of the sanctions. Humimmune Biotech. Researchers in Iran might not want to draw too much attention to their work in case they How badly has the pandemic affected Iran? put potential partnerships in jeopardy or they Since January 2020, we’ve had five waves. run the risk of losing access to raw materials. We’re currently experiencing the highest Researchers are also extremely busy number of new cases reported so far, with during the pandemic. But some have started MAJID ASGARIPOUR/WANA VIA REUTERS MAJID ASGARIPOUR/WANA around 40,000 a day, and the most common to share results. In June, the researchers variant we detect is Delta. -

COVID-19 Vaccine Weekly Intel Report
COVID-19 Vaccine Weekly Intel Report Science, trial forecast, production and news analysis April 23rd - Prepared for BIO, DCVMN, IFPMA © 2021 Airfinity Ltd | Private & Confidential. © 2021 Airfinity Ltd | Private & Confidential Over 9 billion doses could be produced this year An analysis of forecasted production of vaccine candidates ForecasteD proDuction 9,889,406,370 8,478,587,508 7,206,503,589 5,982,385,185 4,871,966,540 3,815,817,604 2,870,502,904 2,080,496,478 1,388,902,344 830,218,085 200,715,588 425,929,684 Jan-21 Feb-21 Mar-21 Apr-21 May-21 Jun-21 Jul-21 Aug-21 Sep-21 Oct-21 Nov-21 Dec-21 © 2021 Airfinity Ltd | Private & Confidential 2 Over 9 billion doses could be produced this year An analysis of forecasted production of vaccine candidates split by candidate Ad26COVS1 (J&J) mRNA-1273 (MoDerna) Ad5-nCoV (CanSino) MVC-COV1901 (MeDigen/Dynavax) AZD1222 (University of OxforD/AstraZeneca) NasoVAX (Altimmune) BBIBP-CorV (Beijing/Sinopharm) NVX-CoV2373 (Novavax) BNT162b2 (Pfizer/BioNTech) S-268019 (UMN Pharma) CoronaVac (Sinovac) SCB-2019 (Clover/Dynavax) COVAXIN (Bharat/ICMR/NIV) Sputnik V (Gamaleya Research Institute) CoviVac (Chumakov FeDeral Scientific Center) UB-612 (Covaxx) CVnCoV (Curevac) Vaccine (Anhui Zhifei) 9,889,406,370 EpiVacCorona (VECTOR) Vaccine (MeDicago/GSK) GRAD-COV2 (Reithera/LeukoCare/Univercells ) Vaccine (Sanofi/GSK) 8,478,587,508 INO-4800 (Inovio Pharma) VLA2001 (Valneva/Dynavax) LUNAR-COV19 (Arcturus) ZyCoV-D (ZyDus Cadila) 7,206,503,589 5,982,385,185 4,871,966,540 3,815,817,604 2,870,502,904 2,080,496,478 -
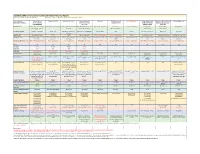
Candidate SARS-Cov-2 Vaccines in Advanced Clinical Trials: Key Aspects Compiled by John D
Candidate SARS-CoV-2 Vaccines in Advanced Clinical Trials: Key Aspects Compiled by John D. Grabenstein, RPh, PhD All dates are estimates. All Days are based on first vaccination at Day 0. Vaccine Sponsor Univ. of Oxford ModernaTX USA BioNTech with Pfizer Johnson & Johnson Novavax Sanofi Pasteur with CureVac with Bayer CanSino Biologics with Sinopharm (China National Sinovac Biotech Co. [with Major Partners] (Jenner Institute) (Janssen Vaccines & GlaxoSmithKline Academy of Military Biotec Group) (Beijing IBP, with AstraZeneca Prevention) Medical Sciences Wuhan IBP) Headquarters Oxford, England; Cambridge, Cambridge, Massachusetts Mainz, Germany; New York, New Brunswick, New Jersey Gaithersburg, Maryland Lyon, France; Tübingen, Germany Tianjin, China; Beijing, China; Beijing, China England, Gothenburg, New York (Leiden, Netherlands) Brentford, England Beijing, China Wuhan, China Sweden Product Designator ChAdOx1 or AZD1222 mRNA-1273 BNT162b2, tozinameran, Ad26.COV2.S, JNJ-78436735 NVX-CoV2373 TBA CVnCoV Ad5-nCoV, Convidecia BBIBP-CorV CoronaVac Comirnaty Vaccine Type Adenovirus 63 vector mRNA mRNA Adenovirus 26 vector Subunit (spike) protein Subunit (spike) protein mRNA Adenovirus 5 vector Inactivated whole virus Inactivated whole virus Product Features Chimpanzee adenovirus type Within lipid nanoparticle Within lipid nanoparticle Human adenovirus type 26 Adjuvanted with Matrix-M Adjuvanted with AS03 or Adjuvanted with AS03 Human adenovirus type 5 Adjuvanted with aluminum Adjuvanted with aluminum 63 vector dispersion dispersion vector AF03 -

SARS-Cov-2 Vaccines in Kidney Transplant Recipients: Will They Be Safe and Effective and How Will We Know?
PERSPECTIVES www.jasn.org SARS-CoV-2 Vaccines in Kidney Transplant Recipients: Will They Be Safe and Effective and How Will We Know? Madeleine R. Heldman and Ajit P. Limaye Division of Allergy and Infectious Diseases, Department of Medicine, University of Washington, Seattle, Washington JASN 32: ccc–ccc, 2021. doi: https://doi.org/10.1681/ASN.2021010023 Coronavirus disease 2019 (COVID-19) will far outweigh risks of vaccination. viral vector–based vaccines could be- has had a major effect on kidney and Accordingly, current guidance from come replication competent and cause other solid organ transplant recipients.1 multiple professional organizations disease, especially in immunocompro- In addition to public health measures, recommend vaccination for all eligible mised individuals. For example, in cells improved access to testing, and thera- organ transplant recipients.2,4,5 concurrently infected with two different peutic developments, vaccination has Each vaccine platform has distinct AdVes, homologous recombination of emerged as a key tool for controlling safety considerations for kidney transplant genetic elements could occur and result the ongoing pandemic. In December recipients. Live (replication-competent) in the emergence of new, pathogenic, 2020, multiple regulatory agencies vaccines are generally contraindicated in replication-competent AdV types.9 This worldwide authorized the use of two immunocompromised individuals be- has been observed in patients with ad- mRNAvaccines for severe acute respiratory cause of a risk of vaccine-acquired -

Download Preprint
1 Title: Comparing COVID-19 vaccines for their characteristics, efficacy and effectiveness against 2 SARS-CoV-2 and variants of concern 3 4 Authors: Thibault Fiolet1*, Yousra Kherabi2,3, Conor-James MacDonald1, Jade Ghosn2,3, Nathan 5 Peiffer-Smadja2,3,4 6 7 1Paris-Saclay University, UVSQ, INSERM, Gustave Roussy, "Exposome and Heredity" team, CESP 8 UMR1018, Villejuif, France 9 2Université de Paris, IAME, INSERM, Paris, France 10 11 3Infectious and Tropical Diseases Department, Bichat-Claude Bernard Hospital, AP-HP, Paris, France 12 13 4National Institute for Health Research Health Protection Research Unit in Healthcare Associated 14 Infections and Antimicrobial Resistance, Imperial College, London, UK 15 16 *Corresponding author: 17 Email: [email protected] 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 1 48 Abstract 49 Vaccines are critical cost-effective tools to control the COVID-19 pandemic. However, the emergence 50 of more transmissible SARS-CoV-2 variants may threaten the potential herd immunity sought from 51 mass vaccination campaigns. 52 The objective of this study was to provide an up-to-date comparative analysis of the characteristics, 53 adverse events, efficacy, effectiveness and impact of the variants of concern (Alpha, Beta, Gamma and 54 Delta) for fourteen currently authorized COVID-19 vaccines (BNT16b2, mRNA-1273, AZD1222, 55 Ad26.COV2.S, Sputnik V, NVX-CoV2373, Ad5-nCoV, CoronaVac, BBIBP-CorV, COVAXIN, 56 Wuhan Sinopharm vaccine, QazCovid-In, Abdala and ZF200) and two vaccines (CVnCoV and NVX- 57 CoV2373) currently in rolling review in several national drug agencies. -

(COVID-19) Vaccination for Seafarers and Shipping Companies: a Practical Guide Your Questions Answered
This first edition was withdrawn in September 2021 and replaced with Coronavirus (COVID-19): Vaccination for Seafarers and Shipping Companies: A Practical Guide, Second Edition Coronavirus (COVID-19) Vaccination for Seafarers and Shipping Companies: A Practical Guide Your Questions Answered Withdrawn In collaboration with This first edition was withdrawn in September 2021 and replaced with Coronavirus (COVID-19): Vaccination for Seafarers and Shipping Companies: A Practical Guide, Second Edition COVID-19 Vaccination for Seafarers and Shipping Companies: A Practical Guide 2 Acknowledgements Thanks are extended to Professor Pierre van Damme, from the University of Antwerp, for some of the information used in this Guide. Background There have been over 100 million cases of Coronavirus (COVID-19) and more than two million COVID-19 deaths recorded worldwide. To date, nearly 200 million people have received one dose of the COVID-19 vaccine. COVID-19 is spread primarily through droplets. A person with COVID-19 coughs or sneezes, spreading droplets into the air and onto objects and surfaces in close proximity. Other people breathe in the droplets or touch the objects or surfaces and then touch their eyes, nose or mouth. COVID-19 vaccines reduce the severity of symptoms or prevent symptoms completely in a vaccinated person. However it is currently unknown if they prevent an individual carrying the virus and passing it on to others. Physical distancing, washing hands with soap and water or the use of hand sanitiser, good respiratory hygiene, and use of a mask remain the main methods to prevent spread of COVID-19 and seafarers should continue these practices once vaccinated.