Flashforward Procedure”: Confronting the Catastrophe
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

2.3 Flash-Forward: the Future Is Now
2.3 Flash-Forward: The Future is Now BY PATRICIA PISTERS 1. The Death of the Image is Behind Us Starting with the observation that “a certain idea of fate and a certain idea of the image are tied up in the apocalyptic discourse of today’s cultural climate,” Jacques Rancière investigates the possibilities of “imageness,” or the future of the image that can be an alternative to the often-heard complaint in contemporary culture that there is nothing but images, and that therefore images are devoid of content or meaning (1). This discourse is particularly strong in discussions on the fate of cinema in the digital age, where it is commonly argued that the cinematographic image has died either because image culture has become saturated with interactive images, as Peter Greenaway argues on countless occasions, or because the digital has undermined the ontological photographic power of the image but that film has a virtual afterlife as either information or art (Rodowick 143). Looking for the artistic power of the image, Rancière offers in his own way an alternative to these claims of the “death of the image.” According to him, the end of the image is long behind us. It was announced in the modernist artistic discourses that took place between Symbolism and Constructivism between the 1880s and 1920s. Rancière argues that the modernist search for a pure image is now replaced by a kind of impure image regime typical for contemporary media culture. | 1 2.3 Flash-Forward: The Future is Now Rancière’s position is free from any technological determinism when he argues that there is no “mediatic” or “mediumistic” catastrophe (such as the loss of chemical imprinting at the arrival of the digital) that marks the end of the image (18). -

Writing Steps
PREWRITING ● gather your thoughts and ideas ○ read, research, interview, experience, discuss, reflect ○ brainstorm, list, journal, freewrite, cluster ● direct your writing ○ determine your purpose (what you want your paper to do) ○ focus and direct your ideas to address your purpose ○ topic, thesis, capsule summary ● tailor your writing ○ determine your audience ○ choose vocabulary, syntax, formality, appeal, organization, approach ○ capture essence and flavor of paper ● plan your writing ○ organize your ideas into an outline or plan ○ chronological, spatial, topical, priority ○ inductive (exploratory), deductive (argumentative) DRAFTING ● get situated ○ comfortable, stimulating, no distractions ● express your ideas without worrying about mechanical details ○ let thoughts flow ○ do not struggle with words, spelling, punctuation, other details ○ do not follow urge to reread, restructure, rewrite ○ write quickly, informally ○ concentrate on main ideas and message ● stick to subject ○ avoid digression into interesting examples ○ follow outline or plan (with minor modifications) ○ use transitions to connect and show relationships between and among ideas ● write draft in one sitting ○ consistent tone, smooth continuity ● consider writing a second, independent draft ○ compare the independent drafts and pull out best parts of each ● take a break when your draft is complete REVISING ● re-envision what you have written ○ ensure your paper fulfills its purpose (what you want the paper to do) ○ consider alternative ways to more effectively, efficiently -

143 the Flashforward Facility at DESY Abstract 1. Introduction
DESY 15-143 The FLASHForward Facility at DESY A. Aschikhin1, C. Behrens1, S. Bohlen1, J. Dale1, N. Delbos2, L. di Lucchio1, E. Elsen1, J.-H. Erbe1, M. Felber1, B. Foster3,4,*, L. Goldberg1, J. Grebenyuk1, J.-N. Gruse1, B. Hidding3,5, Zhanghu Hu1, S. Karstensen1, A. Knetsch3, O. Kononenko1, V. Libov1, K. Ludwig1, A. R. Maier2, A. Martinez de la Ossa3, T. Mehrling1, C. A. J. Palmer1, F. Pannek1, L. Schaper1, H. Schlarb1, B. Schmidt1, S. Schreiber1, J.-P. Schwinkendorf1, H. Steel1,6, M. Streeter1, G. Tauscher1, V. Wacker1, S. Weichert1, S. Wunderlich1, J. Zemella1, J. Osterhoff1 1 Deutsches Elektronen-Synchrotron (DESY), Notkestrasse 85, 22607 Hamburg, Germany 2 Center for Free-Electron Laser Science & Department of Physics, University of Hamburg, Luruper Chaussee 149, 22761 Hamburg, Germany 3 Department of Physics, University of Hamburg, Luruper Chaussee 149, 22761 Hamburg, Germany 4 also at DESY and University of Oxford, UK 5 also at University of Strathclyde, UK 6 also at University of Sydney, Australia * Corresponding author Abstract The FLASHForward project at DESY is a pioneering plasma-wakefield acceleration experiment that aims to produce, in a few centimetres of ionised hydrogen, beams with energy of order GeV that are of quality sufficient to be used in a free-electron laser. The plasma wave will be driven by high- current density electron beams from the FLASH linear accelerator and will explore both external and internal witness-beam injection techniques. The plasma is created by ionising a gas in a gas cell with a multi-TW laser system, which can also be used to provide optical diagnostics of the plasma and electron beams due to the <30 fs synchronisation between the laser and the driving electron beam. -

The Writing Center @ JSCC Literary Terms
The Writing Center @ JSCC Literary Terms When you write or talk about literature, you will need to use literary terms. In this handout, you’ll find a list of some common terms, with definitions. If you come across a term in this handout or in your readings that is not on this sheet, be sure to look it up in the dictionary. Abstract (vs. concrete) – descriptions of ideas or of general qualities of people or things; concrete refers to specific ideas, qualities, people, or things. For example, the statement “Omar loves Sally” is con- crete; the statement “Love is a feeling most people crave” is abstract. Alliteration – the repeating of a specific sound. For example, in “Peter Piper picked a peck of pickled peppers,” the sound /p/ is repeated 8 times and the sound /k/ is repeated 3 times. Alliteration can be used to evoke images in the reader. For example, the /s/ sounds in this passage about the sea in Kate Chopin’s The Awakening might make you think of the sounds the ocean makes: “The voice of the sea is seductive; never ceasing, whispering, clamoring, murmuring, inviting the soul to wander for a spell in abysses of solitude.” Antagonist (vs. protagonist) – the character in a story who works against the hero. Sometimes, but not always, the antagonist is the villain, or the “bad guy.” For example, in the wicked stepmother in Cinderella, Darth Vader in the old Star Wars movies, and the narrator’s mother in Amy Tan’s Two Kinds are all antagonists, even though some (like Tan’s narrator’s mother) are not villains. -

Toward Figural Fantasy
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Helsingin yliopiston digitaalinen arkisto Toward Figural Fantasy The Representation of Consciousness in Modern American Fantasy Literature Master’s Thesis Department of English, University of Helsinki Supervisors: Bo Pettersson, Mark Shackleton 5 December 2006 Timo Lagus 011535360 Contents 1. Introduction 1 1.1. Aims and Methods 2 1.2. Defining Modern Fantasy 6 1.3. Fritz Leiber and George R. R. Martin 10 1.4. The Inward Turn 15 1.5. Note on Terminology 18 2. From Authorial to Figural Perception 20 2.1. Preliminaries: Consciousness and Focalization 20 2.2. Story Space and Story Time 22 2.2.1. Space 22 2.2.2. Time 31 2.3. Knowledge and Reflection 40 2.3.1. Leiber 41 2.3.2. Martin 55 2.4. Conclusion 69 2.5. Afterword: Emotion and Ideology 71 3. Figural Language and Voice 73 3.1. The Three Techniques 73 3.2. Psychonarration 76 3.3. Interior Monologue 85 3.4. Free Indirect Discourse 90 3.5. Narrative Discourse 99 3.6. Conclusion 102 4. The Inward Turn in Modern Fantasy 104 4.1. Before the 1970s: The Modern Classics 105 4.2. 1977: Brooks and Donaldson 111 4.3. From the 1980s to the 2000s: Toward Figural Fantasy 116 4.4. Conclusion 131 5. Conclusion 134 5.1. Leiber, Martin, and Modern American Fantasy 134 5.2. Problems and Future Considerations 136 References 139 i 1. INTRODUCTION Hisvin’s house had in its top floor a small room, the door and window shutters of which were all tightly barred from the inside so that a witness, if there could have been one, would have wondered how this barring had been accomplished in such fashion as to leave the room empty. -

Literary Elements.Pdf
LITERARY ELEMENTS Below is a list of Literary Elements, or the parts of a story. When you examine and analyze your literary work for class presentation, ask the following questions. They will help you find the literary elements of your story. Theme The story's ideas? Author's attitude towards those ideas? Author's "statement" about those ideas? The story's message or main point? Your attitude? Conflict What people/forces/ideas/interests/values/institutions oppose each other? What decisions must the characters make? Between what two things is he/she deciding? What do these things represent? Characterization What kinds of person/people are the character(s)? Their beliefs/hopes/dreams/ideals/ values/morals/fears/strengths/weaknesses/vices/virtues/talents? How do they conduct themselves? What do they say and do to reval themselves? What do others say and do about the? What are your opinions or feelings about them? Classifications of types of characters include: protagonist, antagonist, foil, stereotype, flat, round, static, dynamic. Symbolism What concrete, specific objects have been used to represent abstract ideas? What colors, names, settings, recurring objects have been referred to? What ideas do these represent? Setting Setting refers to TIME and PLACE: Time: of day, year, era/age? Place: city, country? Outside, inside? Rich and opulent or poor and simple? Stark and barren landscape? Rainy or sunny? Beautiful or adversarial? Dark or light? Dangerous or safe? The weather? how does all this affect meaning? What feelings (atmosphere) are evoked just by the setting? Style The way the writer chooses to arrange his sentence structure (syntax) as well as the words (diction) he chooses. -

Death Studiesy
JNDAE7 19(4) 205-272 (2001) ISSN 0891-4494 http://www.wkap.nl/journalhome.htm/0891-4494 Journal nof Lear -Death Studies Y s*4 Editor's Foreword * Bruce Greyson, M.D. The Near-Death Experience as a Shamanic Initiation: A Case Study ' J. Timothy Green, Ph.D. Near-Death Experience: Knowledge and Attitudes of College Students * Kay E. Ketzenberger, Ph.D., and Gina L. Keim, B.A. Prophetic Revelations in Near-Death Experiences* Craig R. Lundahl, Ph.D. Book Reviews: The Physics of Immortality: Modern Cosmology, God and the Resurrection of the Dead, by Frank J. Tipler * Reviewed by John Wren-Lewis Children of the New Millenium: Children's Near-Death Experiences and the Evolution of Humankind, by P .M. H. Atwater* Reviewed by Thomas A. Angerpointner, M.D., Ph.D. Children of the New Millenium: Children's Near-Death Experiences and the Evolution of Humankind, by P .M. H. Atwater* Reviewed by Harold A. Widdison, Ph.D. Letters to the Editor ' V Krishnan and Bogomir Golobi, Volume 19, Number 4, Summer 2001 Editor Bruce Greyson, M.D., University of Virginia, Charlottesville, VA Consulting Editors James E. Alcock, Ph.D., C.Psych., York University, Toronto, Ont. Carlos Alvarado, Ph.D., ParapsychologyFoundation, New York, NY Boyce Batey, Academy of Religion and Psychical Research, Bloomfield, CT Carl B. Becker, Ph.D., Kyoto University, Kyoto, Japan Paul Bernstein, Ph.D., Chelsea, MA Diane K. Corcoran, R.N., Ph.D., Senior University, Richmond, B.C. Elizabeth W. Fenske, Ph.D., Spiritual Frontiers Fellowship International, Philadelphia,PA John C. Gibbs, Ph.D., The Ohio State University, Columbus, OH Stanislav Grof, M.D., Ph.D., CaliforniaInstitute of Integral Studies, San Francisco, CA Michael Grosso, Ph.D., New Jersey City University, Jersey City, NJ Bruce J. -
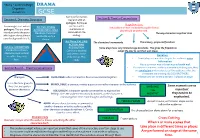
Cross-Cutting When 2 Or More Scenes That Take Place in Different Times Or Places Are Performed on Stage at the Same Time
Year 9 + 10 Knowledge DRAMA Organiser Autumn 2 GCSE Some performances Section A: Dramatic Structure may end with an Section B: Theatre Conventions epilogue. Epilogues Stage Directions: Some might start with a can be used to Act Two: RISING Instructions written in a script to explain how a prologue. This is a short summarise or ACTION AND CLIMAX play should be performed. introduction to the story Develops characters comment on the The way characters say their lines which gives the audience and builds up to a ending. some background details. climax. Act Three: FALLING The characters’ movements The scenery, props and furniture ACTION AND Act One: EXPOSITION RESOLUTION Some plays have very limited stage directions. This gives the freedom to Introduction of main Conflict is resolved adapt the play to suit their own ideas. characters and hints at and settled, loose Narrators: a conflict they may ends tied up. Play • Some plays use narrators to give the audience extra face. ends. information. • Also a common way of breaking the fourth wall. Section B cont… Theatre Conventions • If someone comments on the action without taking part, they are omniscient and are able to tell the audience what the characters are thinking. BLOOD BROTHERS Dialogue: DUOLOGUE: when 2 characters have a conversation together. • Always consider where a narrator is placed on stage This is the term given to MONOLOGUE: a character makes a speech to another character or the audience. lines that are spoken MARKING Some moments are so between characters. SOLILOQUY: a character speaks to themselves to express their THE important feelings. -
An Exploration of the Applicability of Linda Aronson's Flashback Theory
Title An exploration of the applicability of Linda Aronson's flashback theory as a framework for the practice of screenwriting Type Thesis URL http://ualresearchonline.arts.ac.uk/6515/ Date 2011 Citation Scott-Webb, Shirley (2011) An exploration of the applicability of Linda Aronson's flashback theory as a framework for the practice of screenwriting. PhD thesis, University of the Arts London. Creators Scott-Webb, Shirley Usage Guidelines Please refer to usage guidelines at http://ualresearchonline.arts.ac.uk/policies.html or alternatively contact [email protected]. License: Creative Commons Attribution Non-commercial No Derivatives Unless otherwise stated, copyright owned by the author An exploration of the applicability of Linda Aronson's flashback theory as a framework for the practice of screen writing Practice-based PhD by Shirley Scott-Webb University of the Arts London February 2011 Supervisors Phil Parker & Professor Jon Cook ABSTRACT An exploration of the applicability of Linda Aronson's flashback theory as a framework for the practice of screenwriting. This practice-based PhD comprises an original screenplay for a biopic of the life and trial of zo" century Scottish medium Helen Duncan, entitled Hellish Nell, and a thesis which reflects the process of writing the script using Linda Aronson's flashback narrative structures. The central focus of this thesis is to explore the applicability of Aronson's theoretical frameworks first circulated in Screen writing Updated in 2000 through the various stages of script development. The Introduction examines what a flashback is and its uses. It sets out Linda Aronson's theoretical framework on flashback narrative structure, in particular her theory on case history and thwarted dream. -

Uva-DARE (Digital Academic Repository)
UvA-DARE (Digital Academic Repository) Flashforward: the future is now Pisters, P. DOI 10.3366/dls.2011.0039 Publication date 2011 Document Version Final published version Published in Deleuze Studies Link to publication Citation for published version (APA): Pisters, P. (2011). Flashforward: the future is now. Deleuze Studies, 5(suppl.), 98-115. https://doi.org/10.3366/dls.2011.0039 General rights It is not permitted to download or to forward/distribute the text or part of it without the consent of the author(s) and/or copyright holder(s), other than for strictly personal, individual use, unless the work is under an open content license (like Creative Commons). Disclaimer/Complaints regulations If you believe that digital publication of certain material infringes any of your rights or (privacy) interests, please let the Library know, stating your reasons. In case of a legitimate complaint, the Library will make the material inaccessible and/or remove it from the website. Please Ask the Library: https://uba.uva.nl/en/contact, or a letter to: Library of the University of Amsterdam, Secretariat, Singel 425, 1012 WP Amsterdam, The Netherlands. You will be contacted as soon as possible. UvA-DARE is a service provided by the library of the University of Amsterdam (https://dare.uva.nl) Download date:28 Sep 2021 Flashforward: The Future is Now Patricia Pisters University of Amsterdam Abstract In The Future of the Image (2007) Jacques Rancière states that the end of images is behind us. He argues for an aesthetics of the image that acknowledges the continuing power of images as educating documentations of traces of history, as directly affecting interruptions, and as open-to-combining signs of the visible and the sayable ad infinitum. -

Literary and Rhetorical Elements
Literary and Rhetorical Elements Word choice is the deliberate selection of specific words in order to accomplish the writer’s intention to convey specific ideas and a more precise meaning to the readers. In Close Reading for word choice, we need to focus on why an author chose to use the words he or she did. We also need to focus on how using those words affects the meaning of the selection as a whole. This process involves looking at both the individual words in the selection and the way the author uses them. In Close Reading for word choice, you will need to identify connotations, denotations, jargon, figures of speech, literary devices, and rhetorical devices and decide why the author uses them. The following charts will help you identify these aspects of word choice. Figures of speech include, but are not limited to, the following. Figure of Speech Explanation Example Allusion a reference to a well-known work of art, John enjoyed his role as the literature, or music within another work good Samaritan until he of art, literature or music received the bill for repairing Joyce’s car. Apostrophe directly addressing someone who is not O Juliet, what is the secret of present or who is not real true love? Euphemism using a mild, offensive word in place of using “pass away” in place of one that might evoke a stronger reaction “die” Hyperbole extreme exaggeration That suggestion to include a wooden spoon with the ice cream is a million dollar idea! Metaphor an imaginative comparison of two unlike Her mother’s love was a things that does not use either like or as lighthouse in the storm of disappointment. -

Flashforward: the Future Is Now
Flashforward: The Future is Now Patricia Pisters University of Amsterdam Abstract In The Future of the Image (2007) Jacques Rancière states that the end of images is behind us. He argues for an aesthetics of the image that acknowledges the continuing power of images as educating documentations of traces of history, as directly affecting interruptions, and as open-to-combining signs of the visible and the sayable ad infinitum. But does Rancière’s claim also concern the future of cinema? His cinematic references, in a Deleuzian sense, are mostly to modern time-images. Is the future of film indeed a form of the time-image, or has the ‘heart’ of cinema moved beyond this image-type? This paper proposes to look at a third category of cinematographic images, based in the third synthesis of time as developed by Deleuze in Difference and Repetition. This filmic image, that could be called the neuro-image, is connected to the impure regime of images typical for the database logic of the digital age. By comparing Alain Resnais’s Hiroshima Mon Amour (1959) to the television seriesFlashForward (2009), I will analyse the temporal operations of the image of the time-image to these images of a new regime of images, the image of and from the future.1 Keywords: time-image, neuro-image, brain is screen, database logic, flashback, flashforward, future of the image I. The Death of the Image is Behind Us Starting with the observation that ‘a certain idea of fate and a certain idea of the image are tied up in the apocalyptic discourse of today’s cultural climate’, Jacques Rancière investigates the possibilities of ‘imageness’ or the future of the image that can be an alternative to Deleuze Studies Volume 5: 2011 supplement: 98–115 DOI: 10.3366/dls.2011.0039 © Edinburgh University Press www.eupjournals.com/dls Flashforward: The Future is Now 99 the often heard complaint in contemporary culture that there is nothing but images, and that therefore images are devoid of content or meaning (Rancière 2007: 1).