WES MATTHEWS, Sr
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

O Klahoma City
MEDIA GUIDE O M A A H C L I K T Y O T R H U N D E 2 0 1 4 2 0 1 5 THUNDER.NBA.COM TABLE OF CONTENTS GENERAL INFORMATION ALL-TIME RECORDS General Information .....................................................................................4 Year-By-Year Record ..............................................................................116 All-Time Coaching Records .....................................................................117 THUNDER OWNERSHIP GROUP Opening Night ..........................................................................................118 Clayton I. Bennett ........................................................................................6 All-Time Opening-Night Starting Lineups ................................................119 2014-2015 OKLAHOMA CITY THUNDER SEASON SCHEDULE Board of Directors ........................................................................................7 High-Low Scoring Games/Win-Loss Streaks ..........................................120 All-Time Winning-Losing Streaks/Win-Loss Margins ...............................121 All times Central and subject to change. All home games at Chesapeake Energy Arena. PLAYERS Overtime Results .....................................................................................122 Photo Roster ..............................................................................................10 Team Records .........................................................................................124 Roster ........................................................................................................11 -

CONGRESSIONAL RECORD—SENATE, Vol. 152, Pt. 9 June 21
June 21, 2006 CONGRESSIONAL RECORD—SENATE, Vol. 152, Pt. 9 12231 The PRESIDING OFFICER. Without The resolution, with its preamble, vided as follows: Senator WARNER in objection, it is so ordered. reads as follows: control of 30 minutes, Senator LEVIN in Mr. CHAMBLISS. Mr. President, first S. RES. 519 control of 15 minutes, Senator KERRY I ask unanimous consent that a mem- Whereas on Tuesday, June 20, 2006, the in control of 15 minutes. ber of my staff, Beth Sanford, be grant- Miami Heat defeated the Dallas Mavericks I further ask unanimous consent that ed floor privileges during the remain- by a score of 95 to 92, in Dallas, Texas; following the 60 minutes, the Demo- der of this bill. Whereas that victory marks the first Na- cratic leader be recognized for up to 15 The PRESIDING OFFICER. Without tional Basketball Association (NBA) Cham- minutes to close, to be followed by the objection, it is so ordered. pionship for the Miami Heat franchise; majority leader for up to 15 minutes to Whereas after losing the first 2 games of f the NBA Finals, the Heat came back to win close. Finally, I ask consent that fol- lowing that time, the Senate proceed CONGRATULATING THE MIAMI 4 games in a row, which earned the team an to the vote on the Levin amendment, HEAT overall record of 69-37 and the right to be named NBA champions; to be followed by a vote in relation to Mr. TALENT. Mr. President, I ask Whereas Pat Riley, over his 11 seasons the Kerry amendment, with no amend- unanimous consent that the Senate with the Heat, has maintained a standard of ment in order to the Kerry amend- now proceed to the consideration of S. -

Remembrances and Thank Yous by Alan Cotler, W'72
Remembrances and Thank Yous By Alan Cotler, W’72, WG’74 When I told Mrs. Spitzer, my English teacher at Flushing High in Queens, I was going to Penn her eyes welled up and she said nothing. She just smiled. There were 1,100 kids in my graduating class. I was the only one going to an Ivy. And if I had not been recruited to play basketball I may have gone to Queens College. I was a student with academic friends and an athlete with jock friends. My idols were Bill Bradley and Mickey Mantle. My teams were the Yanks, the New York football Giants, the Rangers and the Knicks, and, 47 years later, they are still my teams. My older cousin Jill was the first in my immediate and extended family to go to college (Queens). I had received virtually no guidance about college and how life was about to change for me in Philadelphia. I was on my own. I wanted to get to campus a week before everyone. I wanted the best bed in 318 Magee in the Lower Quad. Steve Bilsky, one of Penn’s starting guards at the time who later was Penn’s AD for 25 years and who helped recruit me, had that room the year before, and said it was THE best room in the Quad --- a large room on the 3rd floor, looked out on the entire quad, you could see who was coming and going from every direction, and it had lots of light. It was the control tower of the Lower Quad. -

FOR IMMEDIATE RELEASE: August 2, 2017
FOR IMMEDIATE RELEASE: August 2, 2017 Ronnie Lester will Host Event for Kenny Arnold Foundation During Labor Day Weekend; Fans Have a Chance to Meet the Stars of Iowa’s 1980 Final Four Team IOWA CITY, IA – Ronnie Lester, widely regarded as the best basketball player in Hawkeye history, will be making one of his all-time greatest assists this Labor Day weekend in Iowa City. Lester, along with almost the entire 1980 Final Four basketball team, will be accessible to Hawk fans at a special fundraising event in Iowa City in support of the Kenny Arnold Foundation. Kenny Arnold, who led that Hawkeye team in points and assists, was diagnosed with brain cancer in 1984 and has been fighting health issues ever since. The brain tumor and several subsequent strokes have limited Arnold’s mobility, robbed him of his ability to speak and left him in a state of chronic pain. Arnold’s former Iowa teammates and coaches, and the entire Hawkeye Basketball Family, have stayed in contact with Arnold throughout his medical and financial challenges. Today, Arnold’s Hawkeye Basketball Family – his “Teammates For Life” – have dedicated their efforts to provide support for Arnold and others in need through this foundation. “We know that what happened to Kenny could happen to any of us,” said Lester, a Hawkeye All- American on Iowa’s 1979 Big Ten championship team. “All the guys have rallied around him and I’m so proud of my teammates for that. Kenny is very appreciative of all the love and support that his teammates and the Iowa fans have shown him.” Meet and Greet at the Marriott Hotel The event will be a “Meet and Greet” on Friday, September 1 at the Marriott Hotel in Coralville from 7 p.m. -

65 Orlando Magic Magazine Photo Frames (Green Tagged and Numbered)
65 Orlando Magic Magazine Photo Frames (Green Tagged and Numbered) 1. April 1990 “Stars Soar Into Orlando” 2. May 1990 “Ice Gets Hot” 3. May 1990 “The Rookies” 4. June 1990 Magic Dancers “Trying Tryouts” 5. October 1990 “Young Guns III” 6. December 1990 Greg Kite “BMOC” 7. January 1991 “Battle Plans” 8. February 1991 “Cat Man Do” 9. April 1991 “Final Exam” 10. May 1991 Dennis Scott “Free With The Press” 11. June 1991 Scott Skiles “A Star on the Rise” 12. October 1991 “Brian Williams: Renaissance Man” 13. December 1991 “Full Court Press” 14. January 1992 Scott Skiles “The Fitness Team” 15. February 1992 TV Media “On The Air” 16. All-Star Weekend 1992 “Orlando All Star” 17. March 1992 Magic Johnson “Magic Memories” 18. April 1992 “Star Search” 19. June 1992 Shaq “Shaq, Rattle and Roll” 20. October 1992 Shaq “It’s Shaq Time” (Autographed) 21. December 1992 Shaq “Reaching Out” 22. January 1993 Nick Anderson “Flying in Style” 23. May 1993 Shaq “A Season to Remember” 24. Summer 1993 Shaq “The Shaq Era” 25. November 1993 Shaq “Great Expectations” 26. December 1993 Scott Skiles “Leader of the Pack” 27. January 1994 Larry Krystkowiak “Big Guy From Big Sky” 28. February 1994 Anthony Bowie “The Energizer” 29. March 1994 Anthony Avant “Avant’s New Adventure” 30. June 1994 Shaq “Ouch” 31. July 1994 Dennis Scott “The Comeback Kid” 32. August 1994 Shaq “Shaq’s Dream World” 33. September 1994 “Universal Appeal” 34. October 1994 Horace Grant “Orlando’s Newest All-Star” 35. November 1994 “The New Fab Five” 36. -

WES MATTHEWS, Sr
Spring Break Basketball Camp Boys and girls grades 3rd to 8th (as of Sept. 2015) with 2-Time NBA Champion WES MATTHEWS, Sr. @ Derby Veterans Community Center 35 Fifth St. Derby, CT 06418 April 13th – 17th M – F 9am – 12pm April 13th – 17th M – F 1pm – 4pm Come learn, have fun and be coached by the best! Groups: Players grouped by JJV (3rd/4th g), JV (5th/6th g) and Varsity (7th/8th g) Schedule: Lecture; Stations; Team concepts/practice; Games Stations: includes customized skills development drills based on grade with individualized evaluation and instruction on all aspects of the game including leadership, team work, emotional preparation. discipline, work ethic and core conditioning Team concepts: Development of: knowledge, rules, language of the game, high basketball IQ, team offenses and defenses Games: Competitive scrimmages and games using indoor and outdoor courts $195 per player per session (includes camp shirt; discounts for siblings and double session registration) To register please visit: dribbledrivebasketball.net or complete this form Contact: Dennis Kelly 203-926-1365 phone Email: [email protected] Wes Matthews, Sr. Summary 2x NBA champion with the Lakers (1987 and 1988) Drafted 14th overall by the Washington Bullets in the 1980 NBA Draft Played with NBA standouts Michael Jordan, Kareem Abdul-Jabbar and Magic Johnson among others Best Import Award winner for the Ginebra San Miguel of the PBA (1991) Father of current NBA shooting guard Wes Matthews Jr. Bio Wes Matthews Sr. is a retired NBA guard who has played for six different NBA teams and in five professional basketball leagues throughout his career. -

University of Cincinnati News Record. Thursday, January 26, 1967. Vol
State· Affiliation Proposed; ,UC: To Benefit Financially by Peter Franklin "The UC students.would be bene- fitted because of Iower fees coup- A plan proposin-g state affilia- led' with broader graduate and tion for UC has 'received the sup- professional offerings. The bene- port of the Ohio Board of Regents. fit to' the University would come The University would continue I from the acquisition ,of a broader under local control and retain its fina~cial base without the loss of' municipal status, but the accept- local ties and support." ance of the- proposal would result Dr.: Langsam explained that in greatly expanded financial aid ' "the City of Cincinnati would reap or the University. benefit from the proposal because l:owerTu.itlonFees of \ the lower instructional fees The most immediate benefit. to made available to its citizens as . ,,', . i '. .~'i 1...b .•...;;0. i " 'U\e uc student would be a drop in well as the millions of new -dollars that would flow into the. city ec- ,ordie Beats AII-Ameri~ci1" es:JtO?M~~~;sa~:6~iOcr.i~~i~~n.a:~:onomy., The city also would bene- r- G ,-, " . \i ~~- ~~ commenting on the proposed - fit from having a University that _ --"" " " ....• . •..•• plan Dr. Walter G. Langsam, UC was - better able to respond to f '" .. - '._, .' . ': '.~ . President, explained that the plan community. needs for 'expanded Later Drops No ..2..Lou. vOre ,. for state affiliation would-benefit and newprograms." , the students, the university, the "The state itself also would by Mike Kelly city and -the state. benefit because it means imple- University of Louisville's Cardi- menting the Regents' master plan nals could, take a tip from the in Southwestern Ohio at consider- Pinkerton police agency: the ,way F~iday/s Concert ably less expense than the· es- to cover Gordie Smith is to put tablishment of a new state uni- three men on him. -

Cardinal Tradition Louisville Basketball
Cardinal Tradition Louisville Basketball Louisville Basketball Tradition asketball is special to Kentuckians. The sport B permeates everyday life from offices to farm- lands, from coal mines to neighborhood drug stores. It is more than just a sport played in the cold winter months. It is a source of pride filled year-round with anticipation, hope and celebration. Kentuckians love their basketball, and the tradition-rich University of Louisville program has supplied its fans with one of the nation’s finest products for decades. Legendary coach Bernard “Peck” Hickman, a Basketball Hall of Fame nominee, arrived on the UofL campus in 1944 to begin a remarkable string of 46 consecutive winning seasons. For 23 seasons, Hickman laid an impressive foundation for UofL. John Dromo, an assistant coach under Hickman for 19 years, continued the Louisville program in outstanding fashion following Hickman’s retirement. For 30 years, Denny Crum followed the same path of success that Hickman and Dromo both walked, guiding the Cardinals to even higher acclaim. Now, Coach Rick Pitino energized a re-emergence in building upon the rich UofL tradition in his 16 years, guiding the Cardinals to the 2013 NCAA championship, NCAA Final Fours in 2005 and 2012 and the NCAA Elite Eight five of the past 10 sea- sons. Among the Cardinals’ past successes include national championships in the NCAA (1980,1986, 2013), NIT (1956) and the NAIB (1948). UofL is Taquan Dean kisses the Freedom Hall floor Tremendous pride is taken in the tradition the only school in the nation to have claimed the after his final game as a Cardinal. -

Renormalizing Individual Performance Metrics for Cultural Heritage Management of Sports Records
Renormalizing individual performance metrics for cultural heritage management of sports records Alexander M. Petersen1 and Orion Penner2 1Management of Complex Systems Department, Ernest and Julio Gallo Management Program, School of Engineering, University of California, Merced, CA 95343 2Chair of Innovation and Intellectual Property Policy, College of Management of Technology, Ecole Polytechnique Federale de Lausanne, Lausanne, Switzerland. (Dated: April 21, 2020) Individual performance metrics are commonly used to compare players from different eras. However, such cross-era comparison is often biased due to significant changes in success factors underlying player achievement rates (e.g. performance enhancing drugs and modern training regimens). Such historical comparison is more than fodder for casual discussion among sports fans, as it is also an issue of critical importance to the multi- billion dollar professional sport industry and the institutions (e.g. Hall of Fame) charged with preserving sports history and the legacy of outstanding players and achievements. To address this cultural heritage management issue, we report an objective statistical method for renormalizing career achievement metrics, one that is par- ticularly tailored for common seasonal performance metrics, which are often aggregated into summary career metrics – despite the fact that many player careers span different eras. Remarkably, we find that the method applied to comprehensive Major League Baseball and National Basketball Association player data preserves the overall functional form of the distribution of career achievement, both at the season and career level. As such, subsequent re-ranking of the top-50 all-time records in MLB and the NBA using renormalized metrics indicates reordering at the local rank level, as opposed to bulk reordering by era. -

Shooting Guard Day 9:00-10:00: Warmups ● 9:00-9:15: Stretch/Roll Call O Spread the Children out Across the Court
Day 2: Shooting Guard Day 9:00-10:00: Warmups ● 9:00-9:15: Stretch/Roll Call o Spread the children out across the court. 8 lines. ● 9:15-9:30: Explain the camp o Introduce coaches, curriculum, and schedule ● 9:30-9:45: Form six lines on the baseline. o Regular: Running, Back pedal, high knee, power skip, karaoke, defense slide, Frankenstein, lunges, bear-crawl ● 9:45-10:00: Ball Warm-up o Right hand, left hand, V dribble, backpedal dribble 10:00-11:00: Drill Stations ● Drill Station 1: V-Cut/L-Cut/backdoor o The coach will stand at the top of the 3-point line to start. Two lines will form on both wings of the 3-point line. Players from each line will take turns cutting for the ball. Once the cut is complete, the coach will pass to the player for a spot-up shot or lay-up. Emphasize agility and quick changes of direction. ● Drill Station 2: Help defense (One pass away) o 3 offensive players will line up around the 3-point line, within passing distance. 2 players will stand between them in defensive stance. The offensive players will pass to one-another around the perimeter. The defensive players will practice switching and help defense. Emphasize the fundamentals of 1 or 2 passes away. ● Drill Station 3: Elbow to elbow shot challenge o Set up two cones at each end of the free-throw line. The coach will stand under the basket, while the player begins at either cone. The drill begins when the coach passes to the player. -
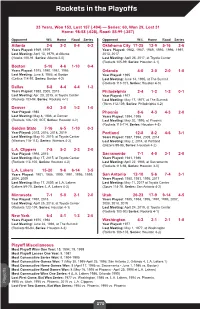
Rockets in the Playoffs
Rockets in the Playoffs 33 Years, Won 153, Lost 157 (.494) — Series: 60, Won 29, Lost 31 Home: 98-58 (.628), Road: 55-99 (.357) Opponent W-L Home Road Series Opponent W-L Home Road Series Atlanta 2-6 2-2 0-4 0-2 Oklahoma City 17-25 12-9 5-16 2-6 Years Played: 1969, 1979 Years Played: 1982, 1987, 1989, 1993, 1996, 1997, Last Meeting: April 13, 1979, at Atlanta 2013, 2017 (Hawks 100-91, Series: Atlanta 2-0) Last Meeting: April 25, 2017, at Toyota Center (Rockets 105-99, Series: Houston 4-1) Boston 5-16 4-6 1-10 0-4 Years Played: 1975, 1980, 1981, 1986 Orlando 4-0 2-0 2-0 1-0 Last Meeting: June 8, 1986, at Boston Year Played: 1995 (Celtics 114-97, Series: Boston 4-2) Last Meeting: June 14, 1995, at The Summit (Rockets 113-101, Series: Houston 4-0) Dallas 8-8 4-4 4-4 1-2 Years Played: 1988, 2005, 2015 Philadelphia 2-4 1-2 1-2 0-1 Last Meeting: Apr. 28, 2015, at Toyota Center Year Played: 1977 (Rockets 103-94, Series: Rockets 4-1) Last Meeting: May 17, 1977, at The Summit (76ers 112-109, Series: Philadelphia 4-2) Denver 4-2 3-0 1-2 1-0 Year Played: 1986 Phoenix 8-6 4-3 4-3 2-0 Last Meeting: May 8, 1986, at Denver Years Played: 1994, 1995 (Rockets 126-122, 2OT, Series: Houston 4-2) Last Meeting: May 20, 1995, at Phoenix (Rockets 115-114, Series: Houston 4-3) Golden State 7-16 6-5 1-10 0-3 Year Played: 2015, 2016, 2018, 2019 Portland 12-8 8-2 4-6 3-1 Last Meeting: May 10, 2019, at Toyota Center Years Played: 1987, 1994, 2009, 2014 (Warriors 118-113), Series: Warriors 4-2) Last Meeting: May 2, 2014, at Portland (Blazers 99-98, Series: Houston 4-2) L.A. -

2012-13 BOSTON CELTICS Media Guide
2012-13 BOSTON CELTICS SEASON SCHEDULE HOME AWAY NOVEMBER FEBRUARY Su MTWThFSa Su MTWThFSa OCT. 30 31 NOV. 1 2 3 1 2 MIA MIL WAS ORL MEM 8:00 7:30 7:00 7:30 7:30 4 5 6 7 8 9 10 3 4 5 6 7 8 9 WAS PHI MIL LAC MEM MEM TOR LAL MEM MEM 7:30 7:30 8:30 1:00 7:30 7:30 7:00 8:00 7:30 7:30 11 12 13 14 15 16 17 10 11 12 13 14 15 16 CHI UTA BRK TOR DEN CHA MEM CHI MEM MEM MEM 8:00 7:30 8:00 12:30 6:00 7:00 7:30 7:30 7:30 7:30 7:30 18 19 20 21 22 23 24 17 18 19 20 21 22 23 DET SAN OKC MEM MEM DEN LAL MEM PHO MEM 7:30 7:30 7:30 7:AL30L-STAR 7:30 9:00 10:30 7:30 9:00 7:30 25 26 27 28 29 30 24 25 26 27 28 ORL BRK POR POR UTA MEM MEM MEM 6:00 7:30 7:30 9:00 9:00 7:30 7:30 7:30 DECEMBER MARCH Su MTWThFSa Su MTWThFSa 1 1 2 MIL GSW MEM 8:30 7:30 7:30 2 3 4 5 6 7 8 3 4 5 6 7 8 9 MEM MEM MEM MIN MEM PHI PHI MEM MEM PHI IND MEM ATL MEM 7:30 7:30 7:30 7:30 7:30 7:00 7:30 7:30 7:30 7:00 7:00 7:30 7:30 7:30 9 10 11 12 13 14 15 10 11 12 13 14 15 16 MEM MEM MEM DAL MEM HOU SAN OKC MEM CHA TOR MEM MEM CHA 7:30 7:30 7:30 8:00 7:30 8:00 8:30 1:00 7:30 7:00 7:30 7:30 7:30 7:30 16 17 18 19 20 21 22 17 18 19 20 21 22 23 MEM MEM CHI CLE MEM MIL MEM MEM MIA MEM NOH MEM DAL MEM 7:30 7:30 8:00 7:30 7:30 7:30 7:30 7:30 8:00 7:30 8:00 7:30 8:30 8:00 23 24 25 26 27 28 29 24 25 26 27 28 29 30 MEM MEM BRK MEM LAC MEM GSW MEM MEM NYK CLE MEM ATL MEM 7:30 7:30 12:00 7:30 10:30 7:30 10:30 7:30 7:30 7:00 7:00 7:30 7:30 7:30 30 31 31 SAC MEM NYK 9:00 7:30 7:30 JANUARY APRIL Su MTWThFSa Su MTWThFSa 1 2 3 4 5 1 2 3 4 5 6 MEM MEM MEM IND ATL MIN MEM DET MEM CLE MEM 7:30 7:30 7:30 8:00