Meeting of the Board of Directors in Public
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
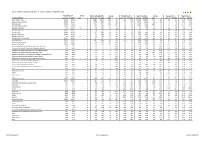
Hallett Arendt Rajar Topline Results - Wave 3 2019/Last Published Data
HALLETT ARENDT RAJAR TOPLINE RESULTS - WAVE 3 2019/LAST PUBLISHED DATA Population 15+ Change Weekly Reach 000's Change Weekly Reach % Total Hours 000's Change Average Hours Market Share STATION/GROUP Last Pub W3 2019 000's % Last Pub W3 2019 000's % Last Pub W3 2019 Last Pub W3 2019 000's % Last Pub W3 2019 Last Pub W3 2019 Bauer Radio - Total 55032 55032 0 0% 18083 18371 288 2% 33% 33% 156216 158995 2779 2% 8.6 8.7 15.3% 15.9% Absolute Radio Network 55032 55032 0 0% 4743 4921 178 4% 9% 9% 35474 35522 48 0% 7.5 7.2 3.5% 3.6% Absolute Radio 55032 55032 0 0% 2151 2447 296 14% 4% 4% 16402 17626 1224 7% 7.6 7.2 1.6% 1.8% Absolute Radio (London) 12260 12260 0 0% 729 821 92 13% 6% 7% 4279 4370 91 2% 5.9 5.3 2.1% 2.2% Absolute Radio 60s n/p 55032 n/a n/a n/p 125 n/a n/a n/p *% n/p 298 n/a n/a n/p 2.4 n/p *% Absolute Radio 70s 55032 55032 0 0% 206 208 2 1% *% *% 699 712 13 2% 3.4 3.4 0.1% 0.1% Absolute 80s 55032 55032 0 0% 1779 1824 45 3% 3% 3% 9294 9435 141 2% 5.2 5.2 0.9% 1.0% Absolute Radio 90s 55032 55032 0 0% 907 856 -51 -6% 2% 2% 4008 3661 -347 -9% 4.4 4.3 0.4% 0.4% Absolute Radio 00s n/p 55032 n/a n/a n/p 209 n/a n/a n/p *% n/p 540 n/a n/a n/p 2.6 n/p 0.1% Absolute Radio Classic Rock 55032 55032 0 0% 741 721 -20 -3% 1% 1% 3438 3703 265 8% 4.6 5.1 0.3% 0.4% Hits Radio Brand 55032 55032 0 0% 6491 6684 193 3% 12% 12% 53184 54489 1305 2% 8.2 8.2 5.2% 5.5% Greatest Hits Network 55032 55032 0 0% 1103 1209 106 10% 2% 2% 8070 8435 365 5% 7.3 7.0 0.8% 0.8% Greatest Hits Radio 55032 55032 0 0% 715 818 103 14% 1% 1% 5281 5870 589 11% 7.4 7.2 0.5% -

Bauer Media Group Phase 1 Decision
Completed acquisitions by Bauer Media Group of certain businesses of Celador Entertainment Limited, Lincs FM Group Limited and Wireless Group Limited, as well as the entire business of UKRD Group Limited Decision on relevant merger situation and substantial lessening of competition ME/6809/19; ME/6810/19; ME/6811/19; and ME/6812/19 The CMA’s decision on reference under section 22(1) of the Enterprise Act 2002 given on 24 July 2019. Full text of the decision published on 30 August 2019. Please note that [] indicates figures or text which have been deleted or replaced in ranges at the request of the parties or third parties for reasons of commercial confidentiality. SUMMARY 1. Between 31 January 2019 and 31 March 2019 Heinrich Bauer Verlag KG (trading as Bauer Media Group (Bauer)), through subsidiaries, bought: (a) From Celador Entertainment Limited (Celador), 16 local radio stations and associated local FM radio licences (the Celador Acquisition); (b) From Lincs FM Group Limited (Lincs), nine local radio stations and associated local FM radio licences, a [] interest in an additional local radio station and associated licences, and interests in the Lincolnshire [] and Suffolk [] digital multiplexes (the Lincs Acquisition); (c) From The Wireless Group Limited (Wireless), 12 local radio stations and associated local FM radio licences, as well as digital multiplexes in Stoke, Swansea and Bradford (the Wireless Acquisition); and (d) The entire issued share capital of UKRD Group Limited (UKRD) and all of UKRD’s assets, namely ten local radio stations and the associated local 1 FM radio licences, interests in local multiplexes, and UKRD’s 50% interest in First Radio Sales (FRS) (the UKRD Acquisition). -

QUARTERLY SUMMARY of RADIO LISTENING Survey Period Ending 25Th June 2017
QUARTERLY SUMMARY OF RADIO LISTENING Survey Period Ending 25th June 2017 PART 1 - UNITED KINGDOM (INCLUDING CHANNEL ISLANDS AND ISLE OF MAN) Adults aged 15 and over: population 54,466,000 Survey Weekly Reach Average Hours Total Hours Share in Period '000 % per head per listener '000 TSA % All Radio Q 49206 90 19.0 21.0 1033226 100.0 All BBC Radio Q 34945 64 9.9 15.5 539982 52.3 All BBC Radio 15-44 Q 14249 56 5.7 10.2 144999 38.0 All BBC Radio 45+ Q 20696 71 13.6 19.1 394983 60.6 All BBC Network Radio1 Q 32136 59 8.5 14.5 464642 45.0 BBC Local Radio Q 8632 16 1.4 8.7 75340 7.3 All Commercial Radio Q 35881 66 8.5 13.0 464812 45.0 All Commercial Radio 15-44 Q 18510 73 8.8 12.0 222329 58.3 All Commercial Radio 45+ Q 17371 60 8.3 14.0 242483 37.2 All National Commercial1 Q 19905 37 3.2 8.7 172369 16.7 All Local Commercial (National TSA) Q 27277 50 5.4 10.7 292443 28.3 Other Radio Q 3903 7 0.5 7.3 28431 2.8 Source: RAJAR/Ipsos MORI/RSMB 1 See note on back cover. For survey periods and other definitions please see back cover. Please note that the information contained within this quarterly data release has yet to be announced or otherwise made public Embargoed until 00.01 am and as such could constitute relevant information for the purposes of section 118 of FSMA and non-public price sensitive 3rd August 2017 information for the purposes of the Criminal Justice Act 1993. -

QUARTERLY SUMMARY of RADIO LISTENING Survey Period Ending 3Rd April 2016
QUARTERLY SUMMARY OF RADIO LISTENING Survey Period Ending 3rd April 2016 PART 1 - UNITED KINGDOM (INCLUDING CHANNEL ISLANDS AND ISLE OF MAN) Adults aged 15 and over: population 53,575,000 Survey Weekly Reach Average Hours Total Hours Share in Period '000 % per head per listener '000 TSA % All Radio Q 47823 89 18.8 21.0 1006462 100.0 All BBC Radio Q 34869 65 10.2 15.6 544682 54.1 All BBC Radio 15-44 Q 14423 57 5.8 10.2 147513 39.1 All BBC Radio 45+ Q 20446 72 14.1 19.4 397169 63.1 All BBC Network Radio1 Q 32014 60 8.8 14.7 469102 46.6 BBC Local Radio Q 8793 16 1.4 8.6 75580 7.5 All Commercial Radio Q 34277 64 8.1 12.7 434436 43.2 All Commercial Radio 15-44 Q 18057 71 8.6 12.0 217166 57.5 All Commercial Radio 45+ Q 16221 57 7.7 13.4 217270 34.5 All National Commercial1 Q 18220 34 2.7 8.1 147175 14.6 All Local Commercial (National TSA) Q 26884 50 5.4 10.7 287261 28.5 Other Radio Q 3816 7 0.5 7.2 27344 2.7 Source: RAJAR/Ipsos MORI/RSMB 1 See note on back cover. For survey periods and other definitions please see back cover. Please note that the information contained within this quarterly data release has yet to be announced or otherwise made public Embargoed until 00.01 am and as such could constitute relevant information for the purposes of section 118 of FSMA and non-public price sensitive 19th May 2016 information for the purposes of the Criminal Justice Act 1993. -
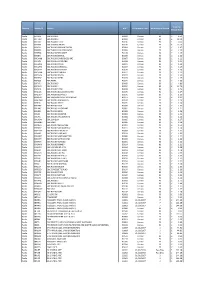
Domain Stationid Station UDC Performance Date Number of Days
Number of days Total Per Amount Amount Performance Domain StationId Station UDC processed Minute from from Public Date for Rate Broadcast Reception distribution RADIO BR ONE BBC RADIO 1 B0001 CENSUS 92 £12.2471 £7.3036 £4.9435 RADIO BR TWO BBC RADIO 2 B0002 CENSUS 92 £25.4860 £25.3998 £0.0862 RADIO BR1EXT BBC 1XTRA CENSUS B0106 CENSUS 92 £2.8113 £2.7199 £0.0914 RADIO BRASIA BBC ASIAN NETWORK (CENSUS) B0064 CENSUS 92 £3.6951 £3.3058 £0.3892 RADIO BRBEDS BBC THREE COUNTIES RADIO (CENSUS) B0065 CENSUS 92 £0.2445 £0.2442 £0.0003 RADIO BRBERK BBC RADIO BERKSHIRE (CENSUS) B0103 CENSUS 92 £0.1436 £0.1435 £0.0002 RADIO BRBRIS BBC RADIO BRISTOL (CENSUS) B0066 CENSUS 92 £0.1532 £0.1531 £0.0002 RADIO BRCAMB BBC RADIO CAMBRIDGESHIRE (CENSUS) B0067 CENSUS 92 £0.1494 £0.1493 £0.0002 RADIO BRCLEV BBC RADIO TEES (CENSUS) B0068 CENSUS 92 £0.1478 £0.1477 £0.0002 RADIO BRCMRU BBC RADIO CYMRU B0011 CENSUS 92 £0.5707 £0.5690 £0.0017 RADIO BRCORN BBC RADIO CORNWALL (CENSUS) B0069 CENSUS 92 £0.1535 £0.1534 £0.0002 RADIO BRCOVN BBC RADIO COVENTRY AND WATWICKSHIRE(CENSUS) B0070 CENSUS 92 £0.1023 £0.1022 £0.0001 RADIO BRCUMB BBC RADIO CUMBRIA (CENSUS) B0071 CENSUS 92 £0.1085 £0.1084 £0.0001 RADIO BRCYMM BBC RADIO CYMRU 2 B0114 CENSUS 92 £0.5707 £0.5690 £0.0017 RADIO BRDEVN BBC RADIO DEVON (CENSUS) B0072 CENSUS 92 £0.2421 £0.2419 £0.0003 RADIO BRDRBY BBC RADIO DERBY (CENSUS) B0073 CENSUS 92 £0.1535 £0.1534 £0.0002 RADIO BRESSX BBC ESSEX (CENSUS) B0074 CENSUS 92 £0.2091 £0.2089 £0.0002 RADIO BRFIVE BBC FIVE LIVE B0005 CENSUS 92 £10.0855 £10.0811 £0.0044 RADIO BRFOYL -

“Reaching 79% of Commercial Radio's Weekly Listeners…” National Coverage
2019 GTN UK is the British division of Global Traffic Network; the leading provider of custom traffic reports to commercial radio and television stations. GTN has similar operations in Australia, Brazil and Canada. GTN is the largest Independent radio network in the UK We offer advertisers access to over 240 radio stations across the country, covering every major conurbation with a solus opportunity enabling your brand to stand out with up to 48% higher ad recall than that of a standard ad break. With both a Traffic & Travel offering, as well as an Entertainment News package, we reach over 28 million adults each week, 80% of all commercial radio’s listeners, during peak listening times only, 0530- 0000. Are your brands global? So are we. Talk to us about a global partnership. Source: Clark Chapman research 2017 RADIO “REACHING 79% OF COMMERCIAL RADIO’S WEEKLY LISTENERS…” NATIONAL COVERAGE 240 radio stations across the UK covering all major conurbations REACH & FREQUENCY Reaching 28 million adults each week, 620 ratings. That’s 79% of commercial radio’s weekly listening. HIGHER ENGAGEMENT With 48% higher ad recall this is the stand-out your brand needs, directly next to “appointment-to-listen” content. BREAKFAST, MORNING, AFTERNOON, DRIVE All advertising is positioned within key radio listening times for maximum reach. 48% HIGHER AD RECALL THAN THAT OF A STANDARD AD BREAK Source: Clark Chapman research NATIONAL/DIGITAL LONDON NORTH EAST Absolute Radio Absolute Radio Capital North East Absolute Radio 70s Kiss Classic FM (North) Absolute -

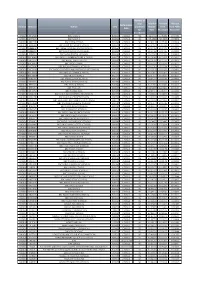
Independent Radio (Alphabetical Order) Frequency Finder
Independent Radio (Alphabetical order) Frequency Finder Commercial and community radio stations are listed together in alphabetical order. National, local and multi-city stations A ABSOLUTE RADIO CLASSIC ROCK are listed together as there is no longer a clear distinction Format: Classic Rock Hits Broadcaster: Bauer between them. ABBEY 104 London area, Surrey, W Kent, Herts, Luton (Mx 3) DABm 11B For maps and transmitter details see: Mixed Format Community Swansea, Neath Port Talbot and Carmarthenshire DABm 12A • Digital Multiplexes Sherborne, Dorset FM 104.7 Shropshire, Wolverhampton, Black Country b DABm 11B • FM Transmitters by Region Birmingham area, West Midlands, SE Staffs a DABm 11C • AM Transmitters by Region ABC Coventry and Warwickshire DABm 12D FM and AM transmitter details are also included in the Mixed Format Community Stoke-on-Trent, West Staffordshire, South Cheshire DABm 12D frequency-order lists. Portadown, County Down FM 100.2 South Yorkshire, North Notts, Chesterfield DABm 11C Leeds and Wakefield Districts DABm 12D Most stations broadcast 24 hours. Bradford, Calderdale and Kirklees Districts DABm 11B Stations will often put separate adverts, and sometimes news ABSOLUTE RADIO East Yorkshire and North Lincolnshire DABm 10D and information, on different DAB multiplexes or FM/AM Format: Rock Music Tees Valley and County Durham DABm 11B transmitters carrying the same programmes. These are not Broadcaster: Bauer Tyne and Wear, North Durham, Northumberland DABm 11C listed separately. England, Wales and Northern Ireland (D1 Mux) DABm 11D Greater Manchester and North East Cheshire DABm 12C Local stations owned by the same broadcaster often share Scotland (D1 Mux) DABm 12A Central and East Lancashire DABm 12A overnight, evening and weekend, programming. -
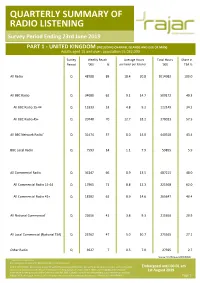
QUARTERLY SUMMARY of RADIO LISTENING Survey Period Ending 23Rd June 2019
QUARTERLY SUMMARY OF RADIO LISTENING Survey Period Ending 23rd June 2019 PART 1 - UNITED KINGDOM (INCLUDING CHANNEL ISLANDS AND ISLE OF MAN) Adults aged 15 and over: population 55,032,000 Survey Weekly Reach Average Hours Total Hours Share in Period '000 % per head per listener '000 TSA % All Radio Q 48788 89 18.4 20.8 1014982 100.0 All BBC Radio Q 34080 62 9.1 14.7 500172 49.3 All BBC Radio 15-44 Q 13333 53 4.8 9.2 122149 34.2 All BBC Radio 45+ Q 20748 70 12.7 18.2 378023 57.5 All BBC Network Radio1 Q 31474 57 8.0 14.0 440318 43.4 BBC Local Radio Q 7593 14 1.1 7.9 59855 5.9 All Commercial Radio Q 36147 66 8.9 13.5 487215 48.0 All Commercial Radio 15-44 Q 17965 71 8.8 12.3 221568 62.0 All Commercial Radio 45+ Q 18182 61 8.9 14.6 265647 40.4 All National Commercial1 Q 22656 41 3.8 9.3 211650 20.9 All Local Commercial (National TSA) Q 25762 47 5.0 10.7 275565 27.1 Other Radio Q 3927 7 0.5 7.0 27595 2.7 Source: RAJAR/Ipsos MORI/RSMB 1 See note on back cover. For survey periods and other definitions please see back cover. Please note that the information contained within this quarterly data release has yet to be announced or otherwise made public Embargoed until 00.01 am and as such could constitute relevant information for the purposes of section 118 of FSMA and non-public price sensitive 1st August 2019 information for the purposes of the Criminal Justice Act 1993. -

What Is Slightly Disturbing Is That Local Radio in This Country Is
What is slightly disturbing is that local radio in this country is suffering thanks in part to the impact of the credit crunch, but also because of the large debts that the companies involved already had. To take an example the case of Global Radio, they have a large amount of debt £210m (according to The Times) at the start of the year which is due in no small part to the purchase of Chrysalis (Radio) and Gcap Media. They have made cuts to the services and removed a large number of local brands to replace them with national ones, to a varying degree of success. There is an argument that says these companies made their bed and they should be lying in them right now, rather than being given hand outs in the form or relaxed regulation. As a former GCap Media shareholder I have a deeper understanding of this company opposed to others in the industry. I'm wary of the idea that lighter touch regulation will work given the way it has been shown not to work in the banking sector and the problems that some radio companies had in the recent past. For example the £1m fine that was accrued under the management of Ralph Bernard and Steve Orchard at Gcap and the failure of former Gcap stations to stick to their format after the takeover by Global. If a station isn't making money do you know what the causes of this are, costs are an easy thing to spread around and something that might actually be profitable can be shown to be loss making. -
Domain Station ID Station UDC Performance Date No of Days in Period Total Per Minute Rate Radio BR ONE BBC RADIO 1 B0001 Census
Total Per Domain Station ID Station UDC Performance Date No of Days in Period Minute Rate Radio BR ONE BBC RADIO 1 B0001 Census 90 £ 4.51 Radio BR TWO BBC RADIO 2 B0002 Census 90 £ 18.00 Radio BR1EXT BBC RADIO 1XTRA B0106 Census 90 £ 0.60 Radio BR4DIG BBC SCHOOL RADIO B0109 Census 90 £ 13.70 Radio BRASIA BBC RADIO ASIAN NETWORK B0064 Census 90 £ 1.47 Radio BRBEDS BBC THREE COUNTIES RADIO B0065 Census 90 £ 1.25 Radio BRBERK BBC RADIO BERKSHIRE B0103 Census 90 £ 1.19 Radio BRBRIS BBC RADIO BRISTOL B0066 Census 90 £ 1.16 Radio BRCAMB BBC RADIO CAMBRIDGESHIRE B0067 Census 90 £ 1.22 Radio BRCLEV BBC RADIO CLEVELAND B0068 Census 90 £ 1.22 Radio BRCMRU BBC RADIO CYMRU B0011 Census 90 £ 1.24 Radio BRCORN BBC RADIO CORNWALL B0069 Census 90 £ 1.29 Radio BRCOVN BBC RADIO COVENTRY B0070 Census 90 £ 1.18 Radio BRCUMB BBC RADIO CUMBRIA B0071 Census 90 £ 1.23 Radio BRDEVN BBC RADIO DEVON B0072 Census 90 £ 1.30 Radio BRDRBY BBC RADIO DERBY B0073 Census 90 £ 1.25 Radio BRESSX BBC ESSEX B0074 Census 90 £ 1.36 Radio BRFIVE BBC RADIO 5 B0005 Census 90 £ 4.89 Radio BRFOUR BBC RADIO 4 B0004 Census 90 £ 13.70 Radio BRFOYL BBC RADIO FOYLE B0019 Census 90 £ 1.76 Radio BRGLOS BBC RADIO GLOUCESTERSHIRE B0075 Census 90 £ 1.17 Radio BRGUER BBC RADIO GUERNSEY B0076 Census 90 £ 1.13 Radio BRHRWC BBC HEREFORD AND WORCESTER B0077 Census 90 £ 1.21 Radio BRHUMB BBC RADIO HUMBERSIDE B0078 Census 90 £ 1.29 Radio BRJERS BBC RADIO JERSEY B0079 Census 90 £ 1.14 Radio BRKENT BBC RADIO KENT B0080 Census 90 £ 1.32 Radio BRLANC BBC RADIO LANCASHIRE B0081 Census 90 £ 1.21 Radio -

Town FM Application
General information (a) Name of Applicant, Address, Telephone and E-mail Note for new applicants: This must be a single legal entity: either a body corporate or a named individual person. If the former, a copy of the certificate of incorporation must be included with the application. Town FM Limited Address: 12 Alpha Business Park White House Road Ipswich IP1 5LT Telephone: 01603 703300 E-mail: [email protected] (b) Main Contact (For Public Purposes) Please nominate at least one individual to deal with any press or public enquiries, stating: Name: Phil Caborn Telephone (daytime): 01603 703300 Address: 12 Alpha Business Park, White House Road, Ipswich, IP1 5LT E-mail: [email protected] (c) Station Name (if decided) Town FM (d) Main Contact (For Ofcom Purposes) Please nominate one individual to whom questions of clarification and/or amplification should be sent, stating: Name: Richard Johnson Address: Celador Radio, County Gates, Ashton Road, Bristol, BS3 2JH E-mail: [email protected] This information may be submitted in confidence, separately from the other responses in this section. 1 Section 105(A): Ability to maintain proposed service 1. Ownership and control of company which will operate the licence (a) Board of Directors i) Provide the name, occupation, other directorships, other media interests, and, if not a director of an existing Ofcom radio licensee, the relevant media experience, of each director (executive and non-executive), including the proposed chairperson. Town FM – a local station underpinned by experience and passion For a small station, we recognise this is a big board. It is the board of Celador Radio with the addition of two local directors. -

QUARTERLY SUMMARY of RADIO LISTENING Survey Period Ending 17Th December 2017
QUARTERLY SUMMARY OF RADIO LISTENING Survey Period Ending 17th December 2017 PART 1 - UNITED KINGDOM (INCLUDING CHANNEL ISLANDS AND ISLE OF MAN) Adults aged 15 and over: population 54,466,000 Survey Weekly Reach Average Hours Total Hours Share in Period '000 % per head per listener '000 TSA % All Radio Q 48860 90 19.1 21.3 1038816 100.0 All BBC Radio Q 35019 64 10.1 15.7 548937 52.8 All BBC Radio 15-44 Q 13938 55 5.5 9.9 138350 36.5 All BBC Radio 45+ Q 21081 72 14.1 19.5 410588 62.3 All BBC Network Radio1 Q 32242 59 8.7 14.7 472924 45.5 BBC Local Radio Q 8297 15 1.4 9.2 76013 7.3 All Commercial Radio Q 35466 65 8.4 13.0 459392 44.2 All Commercial Radio 15-44 Q 17977 71 8.9 12.6 225773 59.5 All Commercial Radio 45+ Q 17489 60 8.0 13.4 233620 35.4 All National Commercial1 Q 20254 37 3.3 8.8 177508 17.1 All Local Commercial (National TSA) Q 26532 49 5.2 10.6 281885 27.1 Other Radio Q 3815 7 0.6 8.0 30486 2.9 Source: RAJAR/Ipsos MORI/RSMB 1 See note on back cover. For survey periods and other definitions please see back cover. Please note that the information contained within this quarterly data release has yet to be announced or otherwise made public Embargoed until 00.01 am and as such could constitute relevant information for the purposes of section 118 of FSMA and non-public price sensitive 8th February 2018 information for the purposes of the Criminal Justice Act 1993.