Studies on the Role of Socs3 and Stat3 in Development and Function of the Immune System
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

An Immunoevasive Strategy Through Clinically-Relevant Pan-Cancer Genomic and Transcriptomic Alterations of JAK-STAT Signaling Components
bioRxiv preprint doi: https://doi.org/10.1101/576645; this version posted March 14, 2019. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY-NC-ND 4.0 International license. An immunoevasive strategy through clinically-relevant pan-cancer genomic and transcriptomic alterations of JAK-STAT signaling components Wai Hoong Chang1 and Alvina G. Lai1, 1Nuffield Department of Medicine, University of Oxford, Old Road Campus, Oxford, OX3 7FZ, United Kingdom Since its discovery almost three decades ago, the Janus ki- Although cytokines are responsible for inflammation in nase (JAK)-signal transducer and activator of transcription cancer, spontaneous eradication of tumors by endoge- (STAT) pathway has paved the road for understanding inflam- nous immune processes rarely occurs. Moreover, the matory and immunity processes related to a wide range of hu- dynamic interaction between tumor cells and host immu- man pathologies including cancer. Several studies have demon- nity shields tumors from immunological ablation, which strated the importance of JAK-STAT pathway components in overall limits the efficacy of immunotherapy in the clinic. regulating tumor initiation and metastatic progression, yet, the extent of how genetic alterations influence patient outcome is far from being understood. Focusing on 133 genes involved in Cytokines can be pro- or anti-inflammatory and are inter- JAK-STAT signaling, we found that copy number alterations dependent on each other’s function to maintain immune underpin transcriptional dysregulation that differs within and homeostasis(3). -

Impact of Chromosome 9 Numerical Imbalances in Oral Squamous Cell Carcinoma: a Pilot Grid-Based Centromere Analysis
diagnostics Communication Impact of Chromosome 9 Numerical Imbalances in Oral Squamous Cell Carcinoma: A Pilot Grid-Based Centromere Analysis 1, 1, 2, Efthymios Kyrodimos y , Aristeidis Chrysovergis y , Nicholas Mastronikolis y, Evangelos Tsiambas 3,*, Christos Riziotis 4,5,* , Dimitrios Roukas 6, Panagiotis Fotiades 7, Chara Stavraka 8 , Vasileios Ragos 9, Minas Paschopoulos 10 and Vasileios Papanikolaou 1 1 1st ENT Department, Hippocration General Hospital, University of Athens, 115 27 Athens, Greece; [email protected] (E.K.); [email protected] (A.C.); [email protected] (V.P.) 2 ENT Department, Medical School, University of Patras, 265 04 Patras, Greece; [email protected] 3 Department of Cytopathology, 417 Veterans Army Hospital (NIMTS), 115 21 Athens, Greece 4 Theoretical and Physical Chemistry Institute, Photonics for Nanoapplications Laboratory, National Hellenic Research Foundation, 11635 Athens, Greece 5 Defence & Security Research Institute, University of Nicosia, CY-2417 Nicosia, Cyprus 6 Department of Psychiatry, 417 Veterans Army Hospital (NIMTS), 115 21 Athens, Greece; [email protected] 7 Department of Surgery, 424 General Army Hospital, 564 29 Thessaloniki, Greece; [email protected] 8 Department of Medical Oncology, Guy’s and St Thomas National Health System Foundation Trust, London SE1 9RT, UK; [email protected] 9 Department of Maxillofacial Surgery, Medical School, University of Ioannina, 455 00 Ioannina, Greece; [email protected] 10 Department of Obstetrics and Gynaecology, School of Health Sciences, University of Ioannina, 455 00 Ioannina, Greece; [email protected] * Correspondence: [email protected] (E.T.); [email protected] (C.R.); Tel.: +00306946939414 (E.T.) These authors are equally contributed. y Received: 16 June 2020; Accepted: 14 July 2020; Published: 21 July 2020 Abstract: Oral squamous cell carcinoma (OSCC) is considered an aggressive malignancy, mainly due to its increased propensity to provide local and distant lymph node metastases. -

Cutting Edge: Expression of IRF8 in Gastric Epithelial Cells Confers
Cutting Edge: Expression of IRF8 in Gastric Epithelial Cells Confers Protective Innate Immunity against Helicobacter pylori Infection This information is current as of September 27, 2021. Ming Yan, Hongsheng Wang, Jiafang Sun, Wei Liao, Peng Li, Yin Zhu, Chengfu Xu, Jungsoo Joo, Yan Sun, Sadia Abbasi, Alexander Kovalchuk, Nonghua Lv, Warren J. Leonard and Herbert C. Morse III J Immunol published online 3 February 2016 Downloaded from http://www.jimmunol.org/content/early/2016/02/02/jimmun ol.1500766 http://www.jimmunol.org/ Supplementary http://www.jimmunol.org/content/suppl/2016/02/02/jimmunol.150076 Material 6.DCSupplemental Why The JI? Submit online. • Rapid Reviews! 30 days* from submission to initial decision • No Triage! Every submission reviewed by practicing scientists by guest on September 27, 2021 • Fast Publication! 4 weeks from acceptance to publication *average Subscription Information about subscribing to The Journal of Immunology is online at: http://jimmunol.org/subscription Permissions Submit copyright permission requests at: http://www.aai.org/About/Publications/JI/copyright.html Email Alerts Receive free email-alerts when new articles cite this article. Sign up at: http://jimmunol.org/alerts The Journal of Immunology is published twice each month by The American Association of Immunologists, Inc., 1451 Rockville Pike, Suite 650, Rockville, MD 20852 Copyright © 2016 by The American Association of Immunologists, Inc. All rights reserved. Print ISSN: 0022-1767 Online ISSN: 1550-6606. Published February 3, 2016, doi:10.4049/jimmunol.1500766 Th eJournal of Cutting Edge Immunology Cutting Edge: Expression of IRF8 in Gastric Epithelial Cells Confers Protective Innate Immunity against Helicobacter pylori Infection x x Ming Yan,*,1 Hongsheng Wang,†,1 Jiafang Sun,† Wei Liao,‡, Peng Li,‡, { † Yin Zhu, ChengfuXu,*JungsooJoo,*YanSun,*SadiaAbbasi,{ x Alexander Kovalchuk,† Nonghua Lv, Warren J. -

SOCS-Mediated Immunomodulation of Natural Killer Cells T ⁎ Narelle Keating, Sandra E
Cytokine 118 (2019) 64–70 Contents lists available at ScienceDirect Cytokine journal homepage: www.elsevier.com/locate/cytokine Review article SOCS-mediated immunomodulation of natural killer cells T ⁎ Narelle Keating, Sandra E. Nicholson Walter and Eliza Hall Institute of Medical Research, Melbourne 3052, Australia Department of Medical Biology, University of Melbourne, Melbourne 3010, Australia ARTICLE INFO ABSTRACT Keywords: Natural killer (NK) cells are innate immune cells with an intrinsic ability to detect and kill infected and can- Cancer cerous cells. The success of therapies targeting immune checkpoints on CD8 cells has intensified interest in Immune checkpoints harnessing the cytolytic effector functions of NK cells for new cancer treatments. NK cell development, survival NK cells and effector activity is dependent on exposure to the cytokine interleukin (IL)-15. The suppressor ofcytokine SOCS proteins (SOCS) proteins (CIS; SOCS1-7) are important negative regulators of cytokine signaling, and both CIS and SOCS2 CIS are reported to have roles in regulating NK cell responses. Their immunomodulatory effects on NK cells suggest SOCS2 that these SOCS proteins are promising targets that can potentially form the basis of novel cancer therapies. Here we discuss the role of NK cells in tumor immunity as well as review the role of the SOCS proteins in regulating IL- 15 signaling and NK cell function. 1. Introduction success of the immune checkpoint inhibitors has stimulated efforts to harness the anti-tumor effector functions of NK cells. Whilst CTLA-4 is Cancer is a major cause of disease burden worldwide, with an es- expressed on the surface of activated murine NK cells, it does not ap- timated 8.2 million cancer-related deaths in 2012 [1] and 1,735,000 pear to be expressed on human NK cells [6]. -

CISH Rabbit Pab
Leader in Biomolecular Solutions for Life Science CISH Rabbit pAb Catalog No.: A14527 Basic Information Background Catalog No. The protein encoded by this gene contains a SH2 domain and a SOCS box domain. The A14527 protein thus belongs to the cytokine-induced STAT inhibitor (CIS), also known as suppressor of cytokine signaling (SOCS) or STAT-induced STAT inhibitor (SSI), protein Observed MW family. CIS family members are known to be cytokine-inducible negative regulators of 37kDa cytokine signaling. The expression of this gene can be induced by IL2, IL3, GM-CSF and EPO in hematopoietic cells. Proteasome-mediated degradation of this protein has been Calculated MW shown to be involved in the inactivation of the erythropoietin receptor. Multiple 28kDa/29kDa/30kDa transcript variants encoding different isoforms have been found for this gene. Category Primary antibody Applications WB,IF Cross-Reactivity Human, Mouse, Rat Recommended Dilutions Immunogen Information WB 1:500 - 1:2000 Gene ID Swiss Prot 1154 Q9NSE2 IF 1:50 - 1:200 Immunogen Recombinant fusion protein containing a sequence corresponding to amino acids 17-130 of human CISH (NP_659508.1). Synonyms CISH;BACTS2;CIS;CIS-1;G18;SOCS Contact Product Information www.abclonal.com Source Isotype Purification Rabbit IgG Affinity purification Storage Store at -20℃. Avoid freeze / thaw cycles. Buffer: PBS with 0.02% sodium azide,50% glycerol,pH7.3. Validation Data Western blot analysis of extracts of 293T cells, using CISH antibody (A14527) at 1:500 dilution. Secondary antibody: HRP Goat Anti-Rabbit IgG (H+L) (AS014) at 1:10000 dilution. Lysates/proteins: 25ug per lane. Blocking buffer: 3% nonfat dry milk in TBST. -

The Emerging Role of Suppressors of Cytokine Signaling (SOCS) in the Development and Progression of Leukemia
cancers Review The Emerging Role of Suppressors of Cytokine Signaling (SOCS) in the Development and Progression of Leukemia Esra’a Keewan 1,2 and Ksenia Matlawska-Wasowska 1,2,* 1 Department of Pediatrics, Division of Hematology and Oncology, University of New Mexico Health Sciences Center, Albuquerque, NM 87131, USA; [email protected] 2 Comprehensive Cancer Center, University of New Mexico, Albuquerque, NM 87131, USA * Correspondence: [email protected]; Tel.: +1-505-272-6177 Simple Summary: The suppressors of cytokine signaling (SOCS) are known cytokine-inducible negative regulators of JAK/STAT and other cell signaling pathways. Deregulation of SOCS expression is linked to various tumor types and inflammatory diseases. While SOCS play a crucial role in the regulation of immune cell function, their roles in hematological malignancies have not been elucidated thus far. In this review, we summarize the current knowledge on the roles of SOCS in leukemia development and progression. We delineate the paradoxical activities of SOCS in different leukemia types and the regulatory mechanisms underlying SOCS deregulation in leukemia. Lastly, we discuss the possible implications of SOCS deregulation for leukemia diagnosis and prognosis. This paper provides new insights into the roles of SOCS in the pathobiology of leukemia and leukemia research. Abstract: Cytokines are pleiotropic signaling molecules that execute an essential role in cell-to-cell communication through binding to cell surface receptors. Receptor binding activates intracellular Citation: Keewan, E.; signaling cascades in the target cell that bring about a wide range of cellular responses, including Matlawska-Wasowska, K. The induction of cell proliferation, migration, differentiation, and apoptosis. -

Characterization of BMS-911543, a Functionally Selective Small-Molecule Inhibitor of JAK2
Leukemia (2012) 26, 280–288 & 2012 Macmillan Publishers Limited All rights reserved 0887-6924/12 www.nature.com/leu ORIGINAL ARTICLE Characterization of BMS-911543, a functionally selective small-molecule inhibitor of JAK2 AV Purandare1, TM McDevitt1, H Wan1, D You1, B Penhallow1, X Han1, R Vuppugalla1, Y Zhang1, SU Ruepp1, GL Trainor1, L Lombardo1, D Pedicord1, MM Gottardis1, P Ross-Macdonald1, H de Silva1, J Hosbach1, SL Emanuel1, Y Blat1, E Fitzpatrick1, TL Taylor1, KW McIntyre1, E Michaud1, C Mulligan1, FY Lee1, A Woolfson1, TL Lasho2, A Pardanani2, A Tefferi2 and MV Lorenzi1 1Research and Development, Bristol-Myers Squibb, Princeton, NJ, USA and 2Department of Medicine, Mayo Clinic, Rochester, MN, USA We report the characterization of BMS-911543, a potent and with decreased lymphocyte development through defects in selective small-molecule inhibitor of the Janus kinase (JAK) type I (IFN-a) and type II (IL-2) cytokine signaling, whereas family member, JAK2. Functionally, BMS-911543 displayed human TYK2 deficiency is associated with impaired anti- potent anti-proliferative and pharmacodynamic (PD) effects in cell lines dependent upon JAK2 signaling, and had little activity microbial and allergic responses indicating important roles of in cell types dependent upon other pathways, such as JAK1 these family members in the regulation of key aspects of and JAK3. BMS-911543 also displayed anti-proliferative re- immune cell development and maintenance.6,7 In contrast, sponses in colony growth assays using primary progenitor JAK2 has been implicated in erythropoiesis through its associa- V617F cells isolated from patients with JAK2 -positive myelopro- tion with the selective association with the single chain cytokine liferative neoplasms (MPNs). -
Reliability of Chromogenic in Situ Hybridization for Detecting HER-2
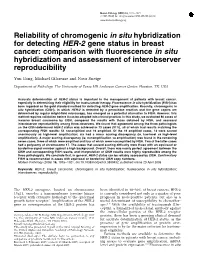
Modern Pathology (2005) 18, 1015–1021 & 2005 USCAP, Inc All rights reserved 0893-3952/05 $30.00 www.modernpathology.org Reliability of chromogenic in situ hybridization for detecting HER-2 gene status in breast cancer: comparison with fluorescence in situ hybridization and assessment of interobserver reproducibility Yun Gong, Michael Gilcrease and Nour Sneige Department of Pathology, The University of Texas MD Anderson Cancer Center, Houston, TX, USA Accurate determination of HER-2 status is important in the management of patients with breast cancer, especially in determining their eligibility for trastuzumab therapy. Fluorescence in situ hybridization (FISH) has been regarded as the gold standard method for detecting HER-2 gene amplification. Recently, chromogenic in situ hybridization (CISH), in which HER-2 is detected by a peroxidase reaction and the gene copies are determined by regular bright-field microscopy, has emerged as a potential alternative to FISH. However, this method requires validation before it can be adopted into clinical practice. In this study, we evaluated 80 cases of invasive breast carcinoma by CISH, compared the results with those obtained by FISH, and assessed interobserver reproducibility among three observers. We found that agreement among the three pathologists on the CISH-determined HER-2 status was achieved in 73 cases (91%), all of which had results matching the corresponding FISH results: 54 nonamplified and 19 amplified. Of the 19 amplified cases, 13 were scored unanimously as high-level amplification; six had a minor scoring discrepancy (ie, low-level vs high-level amplification). A major scoring discrepancy (ie, nonamplification vs amplification) was found in the remaining seven cases, three of which were amplified and four of which were nonamplified by FISH. -

Direct Targets of Pstat5 Signalling in Erythropoiesis
RESEARCH ARTICLE Direct targets of pSTAT5 signalling in erythropoiesis Kevin R. Gillinder1, Hugh Tuckey1,2, Charles C. Bell1, Graham W. Magor1, Stephen Huang1,2, Melissa D. Ilsley1,2, Andrew C. Perkins1,2,3* 1 Cancer Genomics Group, Mater Research Institute - University of Queensland, Translational Research Institute, Woolloongabba, Brisbane, Queensland, Australia, 2 Faculty of Medicine and Biomedical Sciences, University of Queensland, St. Lucia, Brisbane, Queensland, Australia, 3 Princess Alexandra Hospital, Brisbane, Queensland, Australia a1111111111 * [email protected] a1111111111 a1111111111 a1111111111 Abstract a1111111111 Erythropoietin (EPO) acts through the dimeric erythropoietin receptor to stimulate prolifera- tion, survival, differentiation and enucleation of erythroid progenitor cells. We undertook two complimentary approaches to find EPO-dependent pSTAT5 target genes in murine ery- throid cells: RNA-seq of newly transcribed (4sU-labelled) RNA, and ChIP-seq for pSTAT5 OPEN ACCESS 30 minutes after EPO stimulation. We found 302 pSTAT5-occupied sites: ~15% of these Citation: Gillinder KR, Tuckey H, Bell CC, Magor GW, Huang S, Ilsley MD, et al. (2017) Direct reside in promoters while the rest reside within intronic enhancers or intergenic regions, targets of pSTAT5 signalling in erythropoiesis. some >100kb from the nearest TSS. The majority of pSTAT5 peaks contain a central palin- PLoS ONE 12(7): e0180922. https://doi.org/ dromic GAS element, TTCYXRGAA. There was significant enrichment for GATA motifs and 10.1371/journal.pone.0180922 CACCC-box motifs within the neighbourhood of pSTAT5-bound peaks, and GATA1 and/or Editor: Kevin D Bunting, Emory University, UNITED KLF1 co-occupancy at many sites. Using 4sU-RNA-seq we determined the EPO-induced STATES transcriptome and validated differentially expressed genes using dynamic CAGE data and Received: May 19, 2017 qRT-PCR. -

FUS Split CISH Probe TLS/CHOP, Hnrnp-P2
FUS Split CISH Probe TLS/CHOP, hnRNP-P2 Catalog Number: CS0010 Gene Summary: This gene encodes a multifunctional protein component of the heterogeneous nuclear Regulatory Status: For research use only (RUO) ribonucleoprotein (hnRNP) complex. The hnRNP complex is involved in pre-mRNA splicing and the export Product Description: FUS Split CISH Probe is of fully processed mRNA to the cytoplasm. This protein designed for the qualitative detection of translocations belongs to the FET family of RNA-binding proteins which involving the human FUS gene at 16p11.2 in have been implicated in cellular processes that include formalin-fixed, paraffin-embedded specimens by regulation of gene expression, maintenance of genomic chromogenic in situ hybridization (CISH). integrity and mRNA/microRNA processing. Alternative splicing results in multiple transcript variants. Defects in Applications: CISH-P this gene result in amyotrophic lateral sclerosis type 6. (See our web site product page for detailed applications [provided by RefSeq] information) Protocols: See our web site at http://www.abnova.com/support/protocols.asp or product page for detailed protocols Recommend Usage: The product is ready-to-use. No reconstitution, mixing, or dilution is required. Bring probe to room temperature (18-25°C) and mix briefly before use. Supplied Product: Reagent Provided: This Probe is composed of: 1. Digoxigenin-labeled polynucleotides, which target sequences mapping in 16p11.2* (chr16:30,663,949-30,840,569) distal to the FUS breakpoint region. 2. Dinitrophenyl-labeled polynucleotides, which target sequences mapping in 16p11.2* (chr16:31,213,259-31,927,155) proximal to the FUS breakpoint region. 3. Formamide based hybridization buffer. -

Beryllium-Induced Lung Disease Exhibits Expression Profiles Similar to Sarcoidosis
ORIGINAL ARTICLE BERYLLIUM-INDUCED LUNG DISEASE Beryllium-induced lung disease exhibits expression profiles similar to sarcoidosis Li Li1,2, Lori J. Silveira1, Nabeel Hamzeh1,2, May Gillespie1, Peggy M. Mroz1, Annyce S. Mayer1,2,3, Tasha E. Fingerlin1 and Lisa A. Maier1,2,3 Affiliations: 1Dept of Medicine, National Jewish Health, Denver, CO, USA. 2Division of Pulmonary and Critical Care Sciences, Dept of Medicine, School of Medicine, Denver, CO, USA. 3Environmental Occupational Health Dept, School of Public Health, University of Colorado, Denver, CO, USA. Correspondence: Li Li, Division of Environmental and Occupational Health Sciences, Dept of Medicine, National Jewish Health, 1400 Jackson Street, Denver, CO 80206, USA. E-mail: [email protected] ABSTRACT A subset of beryllium-exposed workers develop beryllium sensitisation (BeS) which precedes chronic beryllium disease (CBD). We conducted an in-depth analysis of differentially expressed candidate genes in CBD. We performed Affymetrix GeneChip 1.0 ST array analysis on peripheral blood mononuclear cells (PBMCs) from 10 CBD, 10 BeS and 10 beryllium-exposed, nondiseased controls stimulated with BeSO4 or medium. The differentially expressed genes were validated by high-throughput real-time PCR in this group and in an additional group of cases and nonexposed controls. The functional roles of the top candidate genes in CBD were assessed using a pharmacological inhibitor. CBD gene expression data were compared with whole blood and lung tissue in sarcoidosis from the Gene Expression Omnibus. We confirmed almost 450 genes that were significantly differentially expressed between CBD and controls. The top enrichment of genes was for JAK ( Janus kinase)–STAT (signal transducer and activator of transcription) signalling. -

Negative Regulation of Cytokine Signaling in Immunity
Downloaded from http://cshperspectives.cshlp.org/ on September 27, 2021 - Published by Cold Spring Harbor Laboratory Press Negative Regulation of Cytokine Signaling in Immunity Akihiko Yoshimura, Minako Ito, Shunsuke Chikuma, Takashi Akanuma, and Hiroko Nakatsukasa Department of Microbiology and Immunology, Keio University School of Medicine, Shinjuku-ku, Tokyo 160-8582, Japan Correspondence: [email protected] Cytokines are key modulators of immunity. Most cytokines use the Janus kinase and signal transducers and activators of transcription (JAK-STAT) pathway to promote gene tran- scriptional regulation, but their signals must be attenuated by multiple mechanisms. These include the suppressors of cytokine signaling (SOCS) family of proteins, which represent a main negative regulation mechanism for the JAK-STAT pathway. Cytokine-inducible Src homology 2 (SH2)-containing protein (CIS), SOCS1, and SOCS3 proteins regulate cytokine signals that control the polarization of CD4þ T cells and the maturation of CD8þ T cells. SOCS proteins also regulate innate immune cells and are involved in tumorigenesis. This review summarizes recent progress on CIS, SOCS1, and SOCS3 in T cells and tumor immunity. here are four types of the cytokine receptors: (ERK) pathway (see Fig. 1). Any receptor that T(1) receptors that activate nuclear factor activates intracellular signaling pathways has (NF)-kB and mitogen-activated protein (MAP) multiple negative feedback systems, which en- kinases (mainly p38 and c-Jun amino-terminal sures transient activation of the pathway and kinase [JNK]), such as receptors for the tumor downstream transcription factors. Typical neg- necrosis factor (TNF)-a family, the interleukin ative regulators are shown in Figure 1. Lack of (IL)-1 family, including IL-1b, IL-18, and IL- such negative regulators results in autoimmune 33, and the IL-17 family; (2) receptors that diseases, autoinflammatory diseases, and some- activate the Janus kinase and signal transducers times-fatal disorders, including cancer.