Stem Center Community Support Division Activity Report
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Workingpaper
WORKINGPAPER UNU-EHS PUBLICATION SERIES No. 10 | March 2013 Ecosystems and disaster risk reduction in the context of the Great East Japan Earthquake and Tsunami – a scoping study Report to the Keidanren Nature Conservation Fund Edited by Fabrice Renaud and Radhika Murti INSTITUTE FOR ENVIRONMENT AND HUMAN SECURITY (UNU-EHS) UN UNIVERSITY UNU-EHS Institute for Environment and Human Security United Nations University Institute for Environment and Human Security (UNU-EHS) UN Campus Hermann-Ehlers-Str. 10 53113 Bonn, Germany www.ehs.unu.edu e-mail: [email protected] Copyright UNU-EHS and IUCN 2013 Cover design: Andrea Wendeler N0. 10 | March 2013 The views expressed in this publication are those of the author(s). Publication does not imply endorsement by UNU-EHS or the United Nations University of any of the views expressed. The designation of geographical entities in this publication, and the presentation of the material, do not imply the expression of any opinion whatsoever on the part of IUCN or UNU-EHS concerning the legal status of any country, territory, or area, or of its authorities, or concerning the delimitation of its frontiers or boundaries. The views expressed in this publication do not necessarily reflect those of IUCN. Only available as PDF for download. 2 Working Paper Publication Series of UNU-EHS No. 10 | March 2013 Ecosystems and disaster risk reduction in the context of the Great East Japan Earthquake and Tsunami – a scoping study Report to the Keidanren Nature Conservation Fund Edited by Fabrice Renaud and Radhika Murti 3 Introduction Radhika Murti1 and Fabrice Renaud2 1 International Union for Conservation of Nature (IUCN); 2 United Nations University Institute for Environment and Human Security (UNU-EHS) The Hyogo Framework for Action (HFA) Priority for Action 4 on ‘reducing the underlying risk factors’ advo- cates the ‘sustainable use and management of ecosystems, including through better land-use planning and development activities to reduce risk and vulnerabilities’ (UNISDR, 2005). -

Strategies of the 77 Bank, Ltd Growth Strategy
Strategies of The 77 Bank, Ltd Growth Strategy Best Consulting Bank Human Resource Development In order to become a bank that is truly supported by its customers and to establish a solid management base for the future, we have set the image of the bank we aspire to become as the following, and actively trained specialist resources. Interview 01 “Best Consulting Bank” that responds to customersʼ needs by offering the optimum solutions Striving to solve the issues of quality assurance Corporate Support Department and manpower shortage on the front line of manufacturing. Kei Akama I was assigned to Tohoku Electronics Industry Co., Ltd. with Tohoku Electronics Industry has about 1,000 employees in the headquarters in Ishinomaki City, Miyagi Prefecture for one year entire group, I was forced to be keenly aware of the issue of the under the Local Company Trainee program that started in 2018. shortage of manpower at the manufacturing front line. I believe I was assigned to the Quality Assurance Department, where I that these valuable experiences as a trainee at a local company dealt with automobile manufacturers and interacted with manu- can be utilized in my current work. I am currently working in the facturing sites to ensure the quality of automobile-related parts. Corporate Support Office, providing support mainly to custom- I was interested in the manufacturing industry, including ers in the fishery processing industry in the coastal areas of the automobiles and machinery, and I thought I had acquired some prefecture that are still on the road to recovery from the Great prior knowledge before I was transferred to the company, but I East Japan Earthquake. -

2016 Economic Census for Business Activity (Definitive Report) Tabulations Across Industries Summary of Census Results
2016 Economic Census for Business Activity (Definitive Report) Tabulations across Industries Summary of Census Results I Overview ..................................................................................................................................... 1 II Situations of Number of Enterprises, etc., Sales, and Added Value .......................................... 3 1. Number of Enterprises, etc., Sales, and Added Value ........................................................... 3 2. Added Value Ratio ................................................................................................................. 13 3. Sales by Business Activity ..................................................................................................... 14 4. Capital Investment ................................................................................................................. 18 5. Electronic Commerce (e-commerce) ..................................................................................... 24 6. Situation of Added Value by Prefecture ................................................................................ 27 III Situations of Number of Establishments and Number of Persons Engaged ............................. 29 1. Number of Establishments and Number of Persons Engaged by Industry Division.............. 29 2. Number of Persons Engaged by Status in Employment ........................................................ 33 3. Number of Establishments and Number of Persons Engaged by Size of Persons Engaged -

Post-Earthquake Reconstruction Continues to Blaze Trail Into
lakyara vol.190 Special Edition Post-earthquake reconstruction continues to blaze trail into uncharted territory - Interview with Shinya Endo, General Manager, Miyagi Prefecture Civil Engineering Department - 18.March 2014 Special Edition Post-earthquake reconstruction continues to blaze trail into uncharted territory vol.190 Executive Summary Miyagi Prefecture was particularly hard-hit by the catastrophic Great East Japan Earthquake of March 2011. It is now implementing a ten-year reconstruction plan in three phases. The first phase (three years) is restoration to the pre-earthquake status quo. In the second phase (four years), the Prefecture plans to revitalize (upgrade) its infrastructure to where it would have been if the earthquake had never occurred. In the third phase (three years), the Prefecture aims to better fortify itself against future natural disasters. With no model to follow for any of the three phases, Miyagi Prefecture is grappling with difficult challenges on a daily basis. NRI's Fumihiko Kamio spoke to Shinya Endo, head of Miyagi Prefecture's reconstruction program, about the challenges that lie ahead in 2014, the first year of the ten-year plan's revitalization phase. Shinya Endo General Manager, Miyagi Prefecture Civil Engineering Department Hired by Miyagi Prefecture in 1979. Has worked at prefecture's Ishinomaki Civil Engineering Office, Urban Planning Section, Sendai-Higashi Civil Engineering, Kessennuma Civil Engineering, Road Construction Section, Civil Engineering General Affairs Section, Tokyo Office, and Planning Department's Policy Section. Promoted to Deputy General Manager of Civil Engineering Department in April 2011 after managing Urban Planning Section and Roads Section. Assumed current post in April 2013. -

Miyagi Prefecture Is Blessed with an Abundance of Natural Beauty and Numerous Historic Sites. Its Capital, Sendai, Boasts a Popu
MIYAGI ACCESS & DATA Obihiro Shin chitose Domestic and International Air Routes Tomakomai Railway Routes Oshamanbe in the Tohoku Region Muroran Shinkansen (bullet train) Local train Shin Hakodate Sapporo (New Chitose) Ōminato Miyagi Prefecture is blessed with an abundance of natural beauty and Beijing Dalian numerous historic sites. Its capital, Sendai, boasts a population of over a million people and is Sendai仙台空港 Sendai Airport Seoul Airport Shin- filled with vitality and passion. Miyagi’s major attractions are introduced here. Komatsu Aomori Aomori Narita Izumo Hirosaki Nagoya(Chubu) Fukuoka Hiroshima Hachinohe Osaka(Itami) Shanghai Ōdate Osaka(kansai) Kuji Kobe Okinawa(Naha) Oga Taipei kansen Akita Morioka Honolulu Akita Shin Miyako Ōmagari Hanamaki Kamaishi Yokote Kitakami Guam Bangkok to the port of Hokkaido Sakata Ichinoseki (Tomakomai) Shinjō Naruko Yamagata Shinkansen Ishinomaki Matsushima International Murakami Yamagata Sendai Port of Sendai Domestic Approx. ShiroishiZaō Niigata Yonezawa 90minutes Fukushima (fastest train) from Tokyo to Sendai Aizu- Tohoku on the Tohoku wakamatsu Shinkansen Shinkansen Nagaoka Kōriyama Kashiwazaki to the port of Nagoya Sendai's Climate Naoetsu Echigo Iwaki (℃)( F) yuzawa (mm) 30 120 Joetsu Shinkansen Nikko Precipitation 200 Temperature Nagano Utsunomiya Shinkansen Maebashi 20 90 Mito Takasaki 100 10 60 Omiya Tokyo 0 30 Chiba 0 1 2 3 4 5 6 7 8 9 10 11 12 Publication Date : December 2019 Publisher : Asia Promotion Division, Miyagi Prefectural Government Address : 3-8-1 Honcho, Aoba-ku, Sendai, Miyagi -

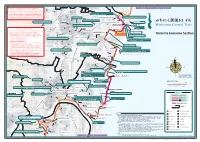
Map Indicating Locations of Activities by Rescue Teams from Foreign Countries/Territories International Organizations, Etc
Map Indicating Locations of Activities by Rescue Teams from Foreign Countries/Territories International Organizations, etc. [as of April 22] Rescue Team Operation by countries Republic of Korea(3/14~3/23) 107 Rescue Workers, 2 Search Dogs Sendai, MIYAGI Singapore(3/13~3/15) 5 Rescue Workers, 5 Search Dog Soma, FUKUSHIMA Germany(3/14~3/15) 41 Rescue Workers, 3 Search Dogs Minami Sanriku, MIYAGI Switzerland(3/14~3/16) 27 Rescue Workers, 9 Search Dogs Minami Sanriku, MIYAGI USA(3/15~3/19) 144 Rescue Workers(incl. Search Dogs) AOMORI Hachinohe Ofunato, Kamaishi, IWATE China(3/14~3/20) 15 Rescue Workers Ofunato, IWATE UK(3/15~3/17) 77 Rescue Workers(including 8 journalists), 2 Search Dogs Ofunato, Kamaishi, IWATE, Kakuda, MIYAGI Mexico(3/15~3/17) 12 Rescue Workers, 6 Search Dogs Natori, MIYAGI Australia(3/16~3/19) 75 Rescue Workers, 2 Search Dogs Minami Sanriku, MIYAGI IWATE New zealand(3/16~3/18) 52 Rescue Workers Minami Sanriku, MIYAGI France(3/16~3/23) 134 Rescue Workers(incl. 11Monacans) After operation in Natori, MIYAGI, They had moved to Hachinohe, AOMORI Kamaishi Taiwan(3/16~3/18) 28 Rescue Workers Natori, Iwanuma, MIYAGI Russia(3/16~3/18) Ofunato 75 First Rescue Workers, 80 Second Rescue Workers Ishinomaki, MIYAGI Mongolia(3/17~3/19) kesennuma 12 Rescue Workers Sendai, Natori, Iwanuma, MIYAGI Minami Sanriku Turkey(3/20 ~4/8) MIYAGI 32 Rescue Workers Tagajo, Ishinomaki, Nanagahama, MIYAGI Ishinomaki Indonesia(3/19~23) 11 Rescue Workers, staff, 4 Medical staff Kesennuma, Shiogama, Ishinomaki, MIYAGI Onagawa South Africa(3/19~3/25) 45 Rescue Workers Shiogama Iwanuma, Natori, Tagajo, Ishinomaki, MIYAGI Israel(3/29 ~) Nanagahama 53 Medical Assistance Workers Minami Sanriku, MIYAGI Tagajo India(3/29 ~ 4/6) Sendai 46 Support Workers Onagawa, MIYAGI Natori Assitance other than rescue teams: USA(3/13~) Italy(3/16~3/21) Taiwa 11-members of Nuclear Regulation Committee Specialists, 34-members of 6-members of Investigation Mission (Rescue, Iwanuma Taiwa Department of Energy operate in Tokyo, Yokota, Nuclear Safety Specialists) operated in Tokyo. -

The Japan Tohoku Tsunami of March 11, 2011
EERI Special Earthquake Report — November 2011 Learning from Earthquakes The Japan Tohoku Tsunami of March 11, 2011 This report summarizes the field Fukushima Prefecture because high US$300 billion, making it the most reconnaissance observations of radiation levels from the damaged costly disaster of all time (VoA, the EERI team led by Lori Dengler, Fukushima Dai-Ichi nuclear power 2011). Humboldt State University, and plant have prevented field teams from There is no question that the Megumi Sugimoto, Earthquake working there. Much of the informa- tsunami was responsible for the Research Institute, University of tion in this preliminary report may huge scale of the catastrophe. A Tokyo, who visited the hardest-hit change as more data and reports are preliminary report released in April areas of Miyagi and Iwate Prefec- released. 2011 summarizing autopsy results tures in April and May 2011. It also The publication of this report is showed 92% of the victims died as includes observations from two In- supported by EERI under National a result of drowning (SEEDS Asia, ternational Tsunami Survey Teams Science Foundation grant #CMMI- 2011). If it is assumed that most of (ITSTs) deployed to study tsunami 1142058. the missing were washed to sea or deposits. The first team visited the deposited in accessible areas by Sendai area in May and was made Introduction the tsunami, the tsunami casualty up of Kazuhisa Goto, Chiba Insti- contribution increases to over 96%. tute of Technology; Shigehiro Fuji- The Mw 9.0 earthquake produced no, University of Tsukuba; Witek a great tsunami that killed nearly This report summarizes field recon- Szczuciski, Adam Mickiewicz Uni- 20,000 people and wreaked destruc- naissance efforts and reports, em- versity, Poland; Yuichi Nishimura, tion along the Tohoku (eastern) phasizing factors that exacerbated Hokkaido University; Daisuke Su- coast of Japan. -

The Great Eastern Japan Earthquake 11 March 2011
1 THE GREAT EASTERN JAPAN EARTHQUAKE 11 MARCH 2011 – LESSONS LEARNED AND RESEARCH QUESTIONS UNU-EHS Institute for Environment and Human Security 11 March 2013, UN Campus, Bonn Editors: Dinil Pushpalal, Jakob Rhyner, Vilma Hossini 2 Imprint United Nations University Institute for Environment and Human Security (UNU-EHS) UN Campus, Hermann-Ehlers-Str. 10, 53113 Bonn, Germany Tel.: + 49-228-815-0200, Fax: + 49-228-815-0299 e-mail: [email protected] Design: Andrea Wendeler Copy-Editing: WordLink Proofreading: Janine Kandel, Sijia Yi, Stanislava Stoyanova Print: Druckerei Paffenholz, Bonn, Germany Print run: 250 Printed in an environmentally friendly manner. The views expressed in this publication are those of the author(s). Publication does not imply endorsement by the United Nations University of any of the views expressed. ISSN: 2075-0498 e-ISSN: 2304-0467 ISBN: 978-3-944535-20-3 e-ISBN: 978-3-944535-21-0 Cover photo: dugspr/flickr THE GREAT EAST JAPAN EARTHQUAKE 11 MARCH 2011 – LESSONS LEARNED AND RESEARCH QUESTIONS CONFERENCE PROCEEDINGS Editors: Dinil Pushpalal, Jakob Rhyner, Vilma Hossini Reviewed by UNU-EHS Foreword 4 11 March 2011 will always be remembered. Remembered by people in Japan, who experienced it as the worst day of their lives when confronted with great loss, fear and uncertainty. But, also, remembered around the world as a day when disaster took on unthinkable dimensions given the intensity as well progressing catenation that emerged that day. Yet, we must admit that it easily might have been even worse: the bulk of the radioactive cloud was blown out to the open sea and not towards Tokyo. -

< 3 Trails Version >
Guide Book Special hikes through magnificent landscapes and hot springs let you explore the region’s distinct history and culture with your five senses. Come experience this healing journey, Miyagi Olle. At long last, a healing journey through magnificent landscapes and rich history < 3 Trails Version > Issue Date: First Edition September 2019 Miyagi Olle Trail, a Healing Journey Matsushima, its picturesque bay dotted with islands large and small, is the start of the journey to Miyagi Prefecture, a region rich with natural beauty. In the west is a range of mountains stretching from Mt. Zao to Mt. Funagata to Mt. Kurikoma. In the center, rice fields stretch out as far as the eye can see, with a beauty that changes from season to sea- son, and is ideal for experiencing traditional culture. The coastal area was badly damaged by tsunami caused by the 2011 Great East Japan Earthquake, but the coastal and mountain trails are being restored to their former beauty. Disaster became the opportunity which sparked the creation of the Miyagi Olle Trail, and with assistance from the Jeju Olle Foundation, in 2018 the Miyagi Olle Trail was created as a sister trail to those in Jeju (Korea), Kyushu and Mongolia. Miyagi Olle Trail has diverse routes, ranging from trails which travel by the endless stretch of the Pacific Ocean, to the natural richness of forested trails, to country roads with opportunities to meet local res- idents. While there are similarities to the Jeju Olle and Kyushu Olle, Miyagi has its own unique features. Olle trails are characterized by people coexisting with nature, and this is firmly embedded in Miyagi Olle as well. -

Community Reconstruction in the Sendai Metropolitan Area After the Great East Japan Earthquake: a Comparative Urban Sociological Approach
Grant-in-Aid for Scientific Research (A) 19H00613 “Comprehensive Research on Local Contexts of Disaster Recovery” Annual Report 2019 Community Reconstruction in the Sendai Metropolitan Area after the Great East Japan Earthquake: A Comparative Urban Sociological Approach Muroi Kenji (Graduate School of Environmental Studies, Nagoya University) Abstract The areas most affected by the Great East Japan earthquake in 2011, were fishery villages in the northern Tohoku (Sanriku) region. Therefore, prior studies have mainly investigated the recovery process on a village basis. However, affected areas in the southern part of Miyagi Prefecture belong to the Sendai Metropolitan Area, where recovery processes were closely interrelated with the regional urban system. This paper aims to explore the characteristics and challenges of disaster recovery in an urban region by conducting a comparative analysis of several municipalities in the Sendai Metropolitan Area and probe the nature of the city from the viewpoint of disaster study. 1. Research Question and Analytical Framework This paper aims to explore the characteristics and challenges of disaster recovery in the southern part of Miyagi Prefecture following the Great East Japan Earthquake in 2011. While much research has been conducted since the earthquake, a large number of them have focused on the tsunami in the northern part of the Tohoku region, specifically in Iwate Prefecture and the northern part of Miyagi Prefecture (e.g., Kawamura et al. 2013, Okamura 2017), or the nuclear power plant accidents in Fukushima Prefecture (e.g., Hasegawa and Yamamoto 2017, Seki 2018). Therefore, prior studies have mainly investigated the recovery process on a village or a person basis. -
Natori to Iwanuma Section
140°49′ 50′ 51′ 52′ 53′ 54′ 55′ 56′ 57′ 58′ 59′ 141°00′ 01′ 02′ ※ Some parts of the Michinoku Coastal Trail lack sidewalks for Continue to Shiogama (city) to Tagajo to Sendai pedestrians, or have roads with heavy traffic. When you walk 258 JR 東 Sendai City on the trail, please follow the traffic rules and pay careful attention 118 273 to prevent accidents. On roads without sidewalks, pedestrians 北 5 Yuriage Bank Pine Trees (Andon Pines) 11’ 本 11’ should walk on the right side of the road. Avoid walking after dark, 線 閖上土手の松並 ( あんどん松 ) try to wear reflective gear or use flashlights to make yourself more 118 Kawamachi Terrace Yuriage Shopping Area visible. If you feel a road is too dangerous to walk, find another way: Koryu-ji Temple Yuriage Shochugakko-mae Bus Stop don’t hesitate to put your safety first. Yuriage’s red clams are nationally famous Yuriage Area place of refuge (roof of disaster recovery public housing) Tohoku Shinkansen Line Horaguchi Family Residence Grave of Fujiwara no Sanekata Yuriage Chuodanchi-mae Bus Stop Yuriage Yacht Harbor Natori Station 129 10 Ongoing reconstruction: 39 Natori Senju Kannon-do Temple follow construction signage 4 4 Hiyoriyama Hill 日和山 — Tsunami Safety Tips — 守病院 Careful, rebuilding road Shinsai Memorial Koen Bus Stop 10’ Morisekinoshita Station 10’ ● If you feel a major earthquake that makes it difficult to stand Miyagi Cancer Center Cycling Sports Center when you are near the coastline, evacuate immediately! Careful, many construction vehicles 127 (opens in 2020) ● If a Tsunami Warning/Advisory is issued by TV, radio, internet, 258 Natori Trail Center Natori to Iwanuma Section or loudspeaker, leave coastal or riverside area immediately and Tsunami Memorial Park Natori Miyagi Psychiatric Center 仙 Mitazono Station evacuate to high ground or a tsunami evacuation building. -

Shiogama(City) to Tagajo to Sendai Section
Sendai- Hokubu Road Access Continue to Ishinomaki(City) to Higashi-Matsushima to Shiogama(Urato Islands) Section Tohoku Expressway Prefectural Route 4 ● By Car 1h 15min 40min Morioka IC Wakayanagi Kannari IC Tome IC 3 Shiwahiko-jinja Shrine 1 Machikado Museum Sanriku Rifu Town 志波彦神社 Higashi-Shiogama Station Tohoku Expressway Sendai-Nanbu Road Sendai-Tobu Road Sanriku Expressway Sanriku Expressway Expressway 40min まちかど博物館 4h 30min 15min 20min 10min Urawa IC Sendai-minami IC Sendai Wakabayashi IC Sendaiko-kita IC Yamoto IC Ishinomaki Kanan IC 3 Shiogama-jinja Shrine Marine Gate Shiogama National Route 45 Shin-Rifu Station 鹽竈神社 Shiogama Tsunami 5min Disaster Prevention Center Tagajo Sta. National Route 45 4 ● By Train/Bus (Please check times in advance) 30min Mutsu Soshanomiya Shrine Hon-Shiogama Station 陸奥総社宮 2 “Kaisho no Yakata” Kokufu-Tagajo Sta. Former Kamei Residence Hon-Shiogama Sta. Shiogama Tourism JR Tohoku Main Line 海商の館 旧亀井邸 15 min Kasenuma Park Information Office Shiogama City Hospital Tokyo Sta. Sendai Sta. Nakanosakae Sta. Hon-Shiogama Sta. 1h 30m 20 min 10 min Taga-jinja Shrine Okama-jinja Shrine Tohoku Shinkansen JR Senseki Line JR Senseki Line Shiogama Station Nishi-Shiogama Station Subway Tozai Line 5 Taga Castle 15 min Government Office Remains Akaishi Hospital Arai Sta. 多賀城政庁跡 Taga Castle Stone Monument Saka General Hospital Sanriku Expressway (Tsubo no Ishibumi) Geba Station ※ Some parts of the Michinoku Coastal Trail lack sidewalks for Tagajo IC pedestrians, or have roads with heavy traffic. When you walk Iwakiri Station JR Tohoku Main LineKokufu-Tagajo Station on the trail, please follow the traffic rules and pay careful attention Rikuzen-Sanno Station to prevent accidents.